




Nicholas Chrimes
@chrimesy.com
Anaesthetist | Creator Vortex Approach | Co-founder Safe Airway Society | Director Universal Airway (PUMA) Guidelines | ANZCA/ASA/NZSA Airway SIG Executive Member
VortexApproach.org
UniversalAirway.org
SafeAirwaySociety.org
EZDrugID.org
VortexApproach.org
UniversalAirway.org
SafeAirwaySociety.org
EZDrugID.org
Pinned
Nicholas Chrimes
@chrimesy.com
· Jun 28
Universal HAVL: 100% grade 1 view & 1st pass success since 2020. 😘👌
This one’s for @drmikeclifford.bsky.social
Cricoid pressure has been selectively vilified out of RSI in many settings, yet it has less risks, a better rationale & more evidence for efficacy than any other cited component of RSI
Why aren’t we doing it routinely for all adult tracheal intubations?
Cricoid pressure has been selectively vilified out of RSI in many settings, yet it has less risks, a better rationale & more evidence for efficacy than any other cited component of RSI
Why aren’t we doing it routinely for all adult tracheal intubations?

Cricoid force: therapeutic, prophylactic or routine
Click on the article title to read more.
associationofanaesthetists-publications.onlinelibrary.wiley.com
November 15, 2025 at 9:00 AM
This one’s for @drmikeclifford.bsky.social
Cricoid pressure has been selectively vilified out of RSI in many settings, yet it has less risks, a better rationale & more evidence for efficacy than any other cited component of RSI
Why aren’t we doing it routinely for all adult tracheal intubations?
Cricoid pressure has been selectively vilified out of RSI in many settings, yet it has less risks, a better rationale & more evidence for efficacy than any other cited component of RSI
Why aren’t we doing it routinely for all adult tracheal intubations?
Reposted by Nicholas Chrimes
Awful. I'm just going to leave this here: yes, bronchospasm can account for a flat capnograph, but no, you can't assume that's the reason and you must take the tube out or (if that's genuinely dangerous) exclude oesophageal intubation using a bronchoscope.
onlinelibrary.wiley.com/share/author...
onlinelibrary.wiley.com/share/author...

September 1, 2025 at 11:22 AM
Awful. I'm just going to leave this here: yes, bronchospasm can account for a flat capnograph, but no, you can't assume that's the reason and you must take the tube out or (if that's genuinely dangerous) exclude oesophageal intubation using a bronchoscope.
onlinelibrary.wiley.com/share/author...
onlinelibrary.wiley.com/share/author...
Reposted by Nicholas Chrimes

Safe Airway Society (a not-for-profit org. in Australia & New Zealand; aiming to optimize safe, effective patient care through a collaborative, multidisciplinary approach to airway management across different healthcare roles & settings) leaves X (3.699 followers)
Bluesky: @safeairwaysociety.org
Bluesky: @safeairwaysociety.org


August 25, 2025 at 11:53 AM
Safe Airway Society (a not-for-profit org. in Australia & New Zealand; aiming to optimize safe, effective patient care through a collaborative, multidisciplinary approach to airway management across different healthcare roles & settings) leaves X (3.699 followers)
Bluesky: @safeairwaysociety.org
Bluesky: @safeairwaysociety.org
International Consensus Guidelines for Preventing Unrecognised Oesophageal Intubation.
Free full text in @anaesjournal.bsky.social
Supported by @dasairway.bsky.social @safeairwaysociety.org @asahq.bsky.social @rcoanews.bsky.social & many more…
www.universalairway.org/puoi/support
Free full text in @anaesjournal.bsky.social
Supported by @dasairway.bsky.social @safeairwaysociety.org @asahq.bsky.social @rcoanews.bsky.social & many more…
www.universalairway.org/puoi/support
September 1, 2025 at 5:45 AM
International Consensus Guidelines for Preventing Unrecognised Oesophageal Intubation.
Free full text in @anaesjournal.bsky.social
Supported by @dasairway.bsky.social @safeairwaysociety.org @asahq.bsky.social @rcoanews.bsky.social & many more…
www.universalairway.org/puoi/support
Free full text in @anaesjournal.bsky.social
Supported by @dasairway.bsky.social @safeairwaysociety.org @asahq.bsky.social @rcoanews.bsky.social & many more…
www.universalairway.org/puoi/support
Yet another case of death from unrecognised oesophageal intubation. The circumstances of the case are tragically similar to previous cases: good clinicians succumbing to cognitive bias.
Please familiarise yourself with the guidelines to avoid falling into the same trap.
@anzca.bsky.social
Please familiarise yourself with the guidelines to avoid falling into the same trap.
@anzca.bsky.social

Woman dies after breathing tube mistakenly inserted into food pipe
The 73-year-old suffered an unsurvivable brain injury after the error went unnoticed for 17 minutes during surgery.
www.1news.co.nz
September 1, 2025 at 5:40 AM
Yet another case of death from unrecognised oesophageal intubation. The circumstances of the case are tragically similar to previous cases: good clinicians succumbing to cognitive bias.
Please familiarise yourself with the guidelines to avoid falling into the same trap.
@anzca.bsky.social
Please familiarise yourself with the guidelines to avoid falling into the same trap.
@anzca.bsky.social
Reposted by Nicholas Chrimes

The most important use of VL is engaging the team. They can see what is happening. Your assistant can see if their airway manoeuvres are helping or hindering. DL is a lonely game.
August 30, 2025 at 8:40 PM
The most important use of VL is engaging the team. They can see what is happening. Your assistant can see if their airway manoeuvres are helping or hindering. DL is a lonely game.
Reposted by Nicholas Chrimes

Absolutely massive crowd in Naarm/Melbourne today. From the river to the sea.




August 24, 2025 at 2:52 AM
Absolutely massive crowd in Naarm/Melbourne today. From the river to the sea.
Reposted by Nicholas Chrimes

He’s wanted to declare martial law from day one.
Bypass all checks and rule as a tyrant.
Many have speculated how he’d do it.
Now his gambit is clear.
DC was a test.
He’s using manufactured crime stats to send troops into blue states & cities.
This is not a drill.
Democracy is at defcon 1.
Bypass all checks and rule as a tyrant.
Many have speculated how he’d do it.
Now his gambit is clear.
DC was a test.
He’s using manufactured crime stats to send troops into blue states & cities.
This is not a drill.
Democracy is at defcon 1.
August 23, 2025 at 11:21 PM
He’s wanted to declare martial law from day one.
Bypass all checks and rule as a tyrant.
Many have speculated how he’d do it.
Now his gambit is clear.
DC was a test.
He’s using manufactured crime stats to send troops into blue states & cities.
This is not a drill.
Democracy is at defcon 1.
Bypass all checks and rule as a tyrant.
Many have speculated how he’d do it.
Now his gambit is clear.
DC was a test.
He’s using manufactured crime stats to send troops into blue states & cities.
This is not a drill.
Democracy is at defcon 1.
Reposted by Nicholas Chrimes

Oh..patients don’t complain when you don’t use LA they just accept it hurts!
What I get is “Oh ..is it done?” Or “Wow..that was ok after all”
Also they don’t move and , should you miss, they don’t get wound up if you have to redo!
What I get is “Oh ..is it done?” Or “Wow..that was ok after all”
Also they don’t move and , should you miss, they don’t get wound up if you have to redo!
August 21, 2025 at 11:03 AM
Oh..patients don’t complain when you don’t use LA they just accept it hurts!
What I get is “Oh ..is it done?” Or “Wow..that was ok after all”
Also they don’t move and , should you miss, they don’t get wound up if you have to redo!
What I get is “Oh ..is it done?” Or “Wow..that was ok after all”
Also they don’t move and , should you miss, they don’t get wound up if you have to redo!
Reposted by Nicholas Chrimes
This is the midweek #MedSkyDebate thanks to @pieterpeach.com
Do you use LA for your cannula insertions?
Do you use LA for your cannula insertions?

Hey @maffygirl.medsky.social, maybe a mid week topic for the future.
“Our patients deserve better: We should use local anaesthetic infiltration for all large gauge intravenous cannulations in elective surgery.”
Eg youtu.be/GXA7D7IOZOc?...
#Ansky
“Our patients deserve better: We should use local anaesthetic infiltration for all large gauge intravenous cannulations in elective surgery.”
Eg youtu.be/GXA7D7IOZOc?...
#Ansky

The Painless Peripheral IV Cannulation
YouTube video by Pieter Peach
youtu.be
August 20, 2025 at 3:39 AM
This is the midweek #MedSkyDebate thanks to @pieterpeach.com
Do you use LA for your cannula insertions?
Do you use LA for your cannula insertions?
Not doing the right thing bc it’s too hard is simply not caring enough.
If the argument for why something - literally anything - should not be done, is that it's complicated, and hard, and you don't understand, blah blah, but good on you for caring... that's literally never a good point. It's always a deflection and never engages. It's PR for inertia
August 18, 2025 at 1:17 AM
Not doing the right thing bc it’s too hard is simply not caring enough.
Reposted by Nicholas Chrimes
If the argument for why something - literally anything - should not be done, is that it's complicated, and hard, and you don't understand, blah blah, but good on you for caring... that's literally never a good point. It's always a deflection and never engages. It's PR for inertia
August 18, 2025 at 12:33 AM
If the argument for why something - literally anything - should not be done, is that it's complicated, and hard, and you don't understand, blah blah, but good on you for caring... that's literally never a good point. It's always a deflection and never engages. It's PR for inertia
While CL has its issues (mainly that no one remembers what the gradings mean) POGO is a completely useless classification system. It can only subclassify easy views (CL 1 -2a) but is unable to discriminate bw challenging views (CL 2b - 4 are all potentially POGO 0%).

Still using Cormack-Lehane grading for VL? Why?!
Out today a new @bjaeducation.bsky.social article by @naomi-gostelow.bsky.social Bhavesh Patel and me looking at grading systems for VL.
#AnSky #MedSky
kwnsfk27.r.eu-west-1.awstrack.me/L0/https:%2F...
Out today a new @bjaeducation.bsky.social article by @naomi-gostelow.bsky.social Bhavesh Patel and me looking at grading systems for VL.
#AnSky #MedSky
kwnsfk27.r.eu-west-1.awstrack.me/L0/https:%2F...

Grading systems for tracheal intubation using videolaryngoscopy
The first videolaryngoscopes were marketed in 2001. In the two decades since, the
number of models available, diversity in design and popularity have all significantly
increased.1 Designs can be class...
www.bjaed.org
August 17, 2025 at 2:20 PM
While CL has its issues (mainly that no one remembers what the gradings mean) POGO is a completely useless classification system. It can only subclassify easy views (CL 1 -2a) but is unable to discriminate bw challenging views (CL 2b - 4 are all potentially POGO 0%).
Reposted by Nicholas Chrimes
Apart from my very niche case HOW LOW WILL YOU GO, or let BP go before you intervene?
Thanks to @chrimesy.com for the topic.
Thanks to @chrimesy.com for the topic.
Let’s keep up the #MedSkyDebate pace!!
Weekend topic is from Nicholas Chrimes @chrimesy.com
“Permissive hypotension: how low will you go?”
My personal low was a 8 hour AVM resection in a 30 year old, at 50 systolic throughout the resection
Brilliant outcome, minimal deficit
Weekend topic is from Nicholas Chrimes @chrimesy.com
“Permissive hypotension: how low will you go?”
My personal low was a 8 hour AVM resection in a 30 year old, at 50 systolic throughout the resection
Brilliant outcome, minimal deficit
a man in front of a microphone with the words how low can you go
ALT: a man in front of a microphone with the words how low can you go
media.tenor.com
August 16, 2025 at 10:43 AM
Apart from my very niche case HOW LOW WILL YOU GO, or let BP go before you intervene?
Thanks to @chrimesy.com for the topic.
Thanks to @chrimesy.com for the topic.
Reposted by Nicholas Chrimes
Let’s keep up the #MedSkyDebate pace!!
Weekend topic is from Nicholas Chrimes @chrimesy.com
“Permissive hypotension: how low will you go?”
My personal low was a 8 hour AVM resection in a 30 year old, at 50 systolic throughout the resection
Brilliant outcome, minimal deficit
Weekend topic is from Nicholas Chrimes @chrimesy.com
“Permissive hypotension: how low will you go?”
My personal low was a 8 hour AVM resection in a 30 year old, at 50 systolic throughout the resection
Brilliant outcome, minimal deficit
a man in front of a microphone with the words how low can you go
ALT: a man in front of a microphone with the words how low can you go
media.tenor.com
August 15, 2025 at 10:19 PM
Let’s keep up the #MedSkyDebate pace!!
Weekend topic is from Nicholas Chrimes @chrimesy.com
“Permissive hypotension: how low will you go?”
My personal low was a 8 hour AVM resection in a 30 year old, at 50 systolic throughout the resection
Brilliant outcome, minimal deficit
Weekend topic is from Nicholas Chrimes @chrimesy.com
“Permissive hypotension: how low will you go?”
My personal low was a 8 hour AVM resection in a 30 year old, at 50 systolic throughout the resection
Brilliant outcome, minimal deficit
Reposted by Nicholas Chrimes

You got away with it. I don’t believe hypotension is permissible.
20% drop of patient’s norm is fine, beyond that bad.
“the purpose of anaesthesia is to keep everything as boring as possible”
“boring” = physiological
20% drop of patient’s norm is fine, beyond that bad.
“the purpose of anaesthesia is to keep everything as boring as possible”
“boring” = physiological
August 16, 2025 at 4:46 AM
You got away with it. I don’t believe hypotension is permissible.
20% drop of patient’s norm is fine, beyond that bad.
“the purpose of anaesthesia is to keep everything as boring as possible”
“boring” = physiological
20% drop of patient’s norm is fine, beyond that bad.
“the purpose of anaesthesia is to keep everything as boring as possible”
“boring” = physiological
Reposted by Nicholas Chrimes

Trump: "I was very happy to hear him say if I was president that war would've never happened."
(Putin knows how to play Trump like a fiddle.)
(Putin knows how to play Trump like a fiddle.)
August 16, 2025 at 1:04 AM
Trump: "I was very happy to hear him say if I was president that war would've never happened."
(Putin knows how to play Trump like a fiddle.)
(Putin knows how to play Trump like a fiddle.)
The people who are crazy enough to think they can change the world are the ones who do.

I don't understand what's wrong with having big ideas that might not be able to be put into practice immediately, but give us something to aspire to. Big ideas expand the tent, they don't collapse it. Am I crazy? Maybe I'm crazy.

August 15, 2025 at 10:57 PM
The people who are crazy enough to think they can change the world are the ones who do.
If sustained exhaled CO2 is in doubt, oesophageal intubation must be ruled out!
🚨We have retired "no trace, wrong place" to align with PUMA guidelines.
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
August 14, 2025 at 7:24 PM
If sustained exhaled CO2 is in doubt, oesophageal intubation must be ruled out!
The PUMA guidelines for preventing unrecognised oesophageal intubation are also supported by @rcoanews.bsky.social @assocsas.bsky.social & many other organisations internationally across anaesthesia, ICU, EM & prehospital
Full list:
www.universalairway.org/puoi/support
@anaesjournal.bsky.social
Full list:
www.universalairway.org/puoi/support
@anaesjournal.bsky.social
August 14, 2025 at 7:11 PM
The PUMA guidelines for preventing unrecognised oesophageal intubation are also supported by @rcoanews.bsky.social @assocsas.bsky.social & many other organisations internationally across anaesthesia, ICU, EM & prehospital
Full list:
www.universalairway.org/puoi/support
@anaesjournal.bsky.social
Full list:
www.universalairway.org/puoi/support
@anaesjournal.bsky.social
Reposted by Nicholas Chrimes
Does attempting to meet legal requirements for informed consent have the potential to *undermine* patient autonomy?
From me, @hypoxicchicken.medsky.social & @maryannturner.bsky.social.
Free full text for a limited time i @anaesjournal.bsky.social
From me, @hypoxicchicken.medsky.social & @maryannturner.bsky.social.
Free full text for a limited time i @anaesjournal.bsky.social

The paradox of informed consent
Click on the article title to read more.
associationofanaesthetists-publications.onlinelibrary.wiley.com
August 1, 2025 at 2:23 PM
Does attempting to meet legal requirements for informed consent have the potential to *undermine* patient autonomy?
From me, @hypoxicchicken.medsky.social & @maryannturner.bsky.social.
Free full text for a limited time i @anaesjournal.bsky.social
From me, @hypoxicchicken.medsky.social & @maryannturner.bsky.social.
Free full text for a limited time i @anaesjournal.bsky.social
Reposted by Nicholas Chrimes

The Safe Airway Liaison Group in the UK have released a statement on displaying the waveform capnography trace in line with the @universalairway.org recommendations. The CO2 trace should be:
1. The bottom trace
2. White
3. Shaded in
www.salg.ac.uk/salg-publica...
1. The bottom trace
2. White
3. Shaded in
www.salg.ac.uk/salg-publica...
SALG | SALG Statement on Waveform Capnography
www.salg.ac.uk
August 14, 2025 at 6:21 PM
The Safe Airway Liaison Group in the UK have released a statement on displaying the waveform capnography trace in line with the @universalairway.org recommendations. The CO2 trace should be:
1. The bottom trace
2. White
3. Shaded in
www.salg.ac.uk/salg-publica...
1. The bottom trace
2. White
3. Shaded in
www.salg.ac.uk/salg-publica...
Reposted by Nicholas Chrimes

🚨We have retired "no trace, wrong place" to align with PUMA guidelines.
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
August 14, 2025 at 12:14 PM
🚨We have retired "no trace, wrong place" to align with PUMA guidelines.
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
Reposted by Nicholas Chrimes
Following on from @sarahmd.bsky.social's discussion, the midweek #MedSkyDebate is what are the cultural work practices you find interesting in other countries.
For me it's surgeons in the USA not putting their own surgical gloves on. That is just weird.
For me it's surgeons in the USA not putting their own surgical gloves on. That is just weird.

a group of surgeons wearing scrubs and masks are working in an operating room .
ALT: a group of surgeons wearing scrubs and masks are working in an operating room .
media.tenor.com
August 13, 2025 at 4:34 AM
Following on from @sarahmd.bsky.social's discussion, the midweek #MedSkyDebate is what are the cultural work practices you find interesting in other countries.
For me it's surgeons in the USA not putting their own surgical gloves on. That is just weird.
For me it's surgeons in the USA not putting their own surgical gloves on. That is just weird.
Reposted by Nicholas Chrimes

Was this the post you mentioned seeing a couple of weeks ago @chrimesy.com ?
bsky.app/profile/anes...
bsky.app/profile/anes...
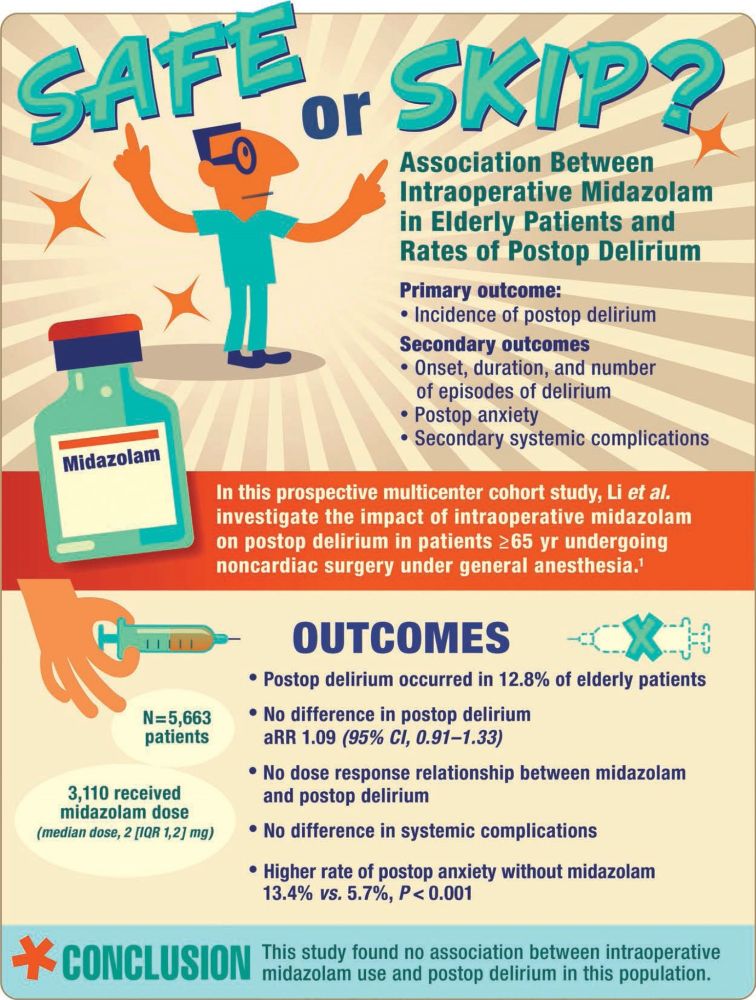
Revisit the February 2025 Infographic in Anesthesiology - Safe or Skip? Association Between Intraoperative Midazolam in Elderly Patients and Rates of Postop Delirium 🎨 ow.ly/Z7Tx50UH1jQ
August 12, 2025 at 6:22 PM
Was this the post you mentioned seeing a couple of weeks ago @chrimesy.com ?
bsky.app/profile/anes...
bsky.app/profile/anes...