




Nicholas Chrimes
@chrimesy.com
Anaesthetist | Creator Vortex Approach | Co-founder Safe Airway Society | Director Universal Airway (PUMA) Guidelines | ANZCA/ASA/NZSA Airway SIG Executive Member
VortexApproach.org
UniversalAirway.org
SafeAirwaySociety.org
EZDrugID.org
VortexApproach.org
UniversalAirway.org
SafeAirwaySociety.org
EZDrugID.org
This is the original graphic before I simplified it. Pale blue lines represent lowest risk of cross reactivity.

November 14, 2025 at 2:38 AM
This is the original graphic before I simplified it. Pale blue lines represent lowest risk of cross reactivity.
Ideally refer for testing to find safe agents. Odd that this was not done during previous skin testing.
Otherwise pancuronium.
Otherwise pancuronium.

November 14, 2025 at 2:33 AM
Ideally refer for testing to find safe agents. Odd that this was not done during previous skin testing.
Otherwise pancuronium.
Otherwise pancuronium.
I didn’t define virtue signalling, I simply stated that complaining about alt text was being used to virtue signal.

September 1, 2025 at 10:20 AM
I didn’t define virtue signalling, I simply stated that complaining about alt text was being used to virtue signal.
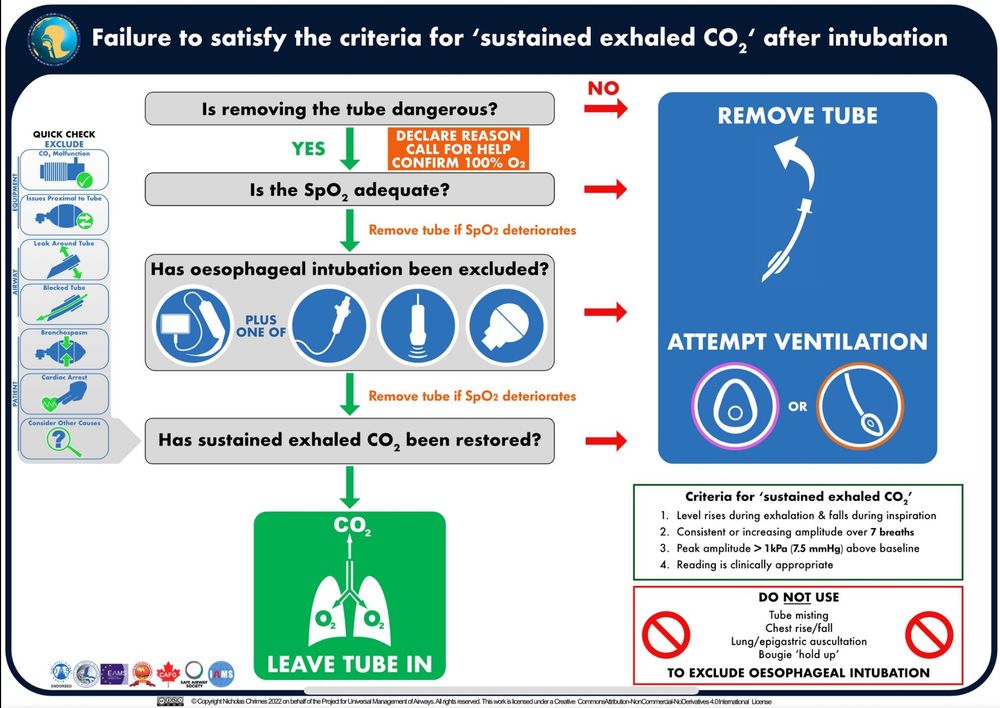
If you think it’s dangerous to remove the tube use a flexible bronchoscope to exclude oesophageal intubation.
September 1, 2025 at 10:10 AM
If you think it’s dangerous to remove the tube use a flexible bronchoscope to exclude oesophageal intubation.
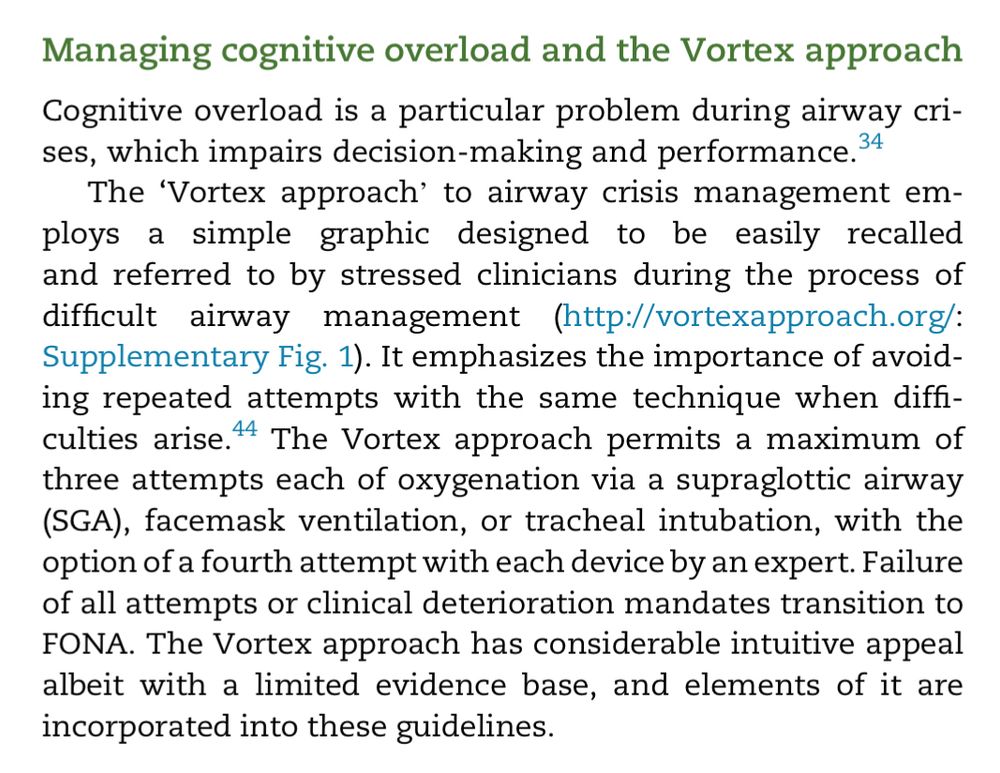
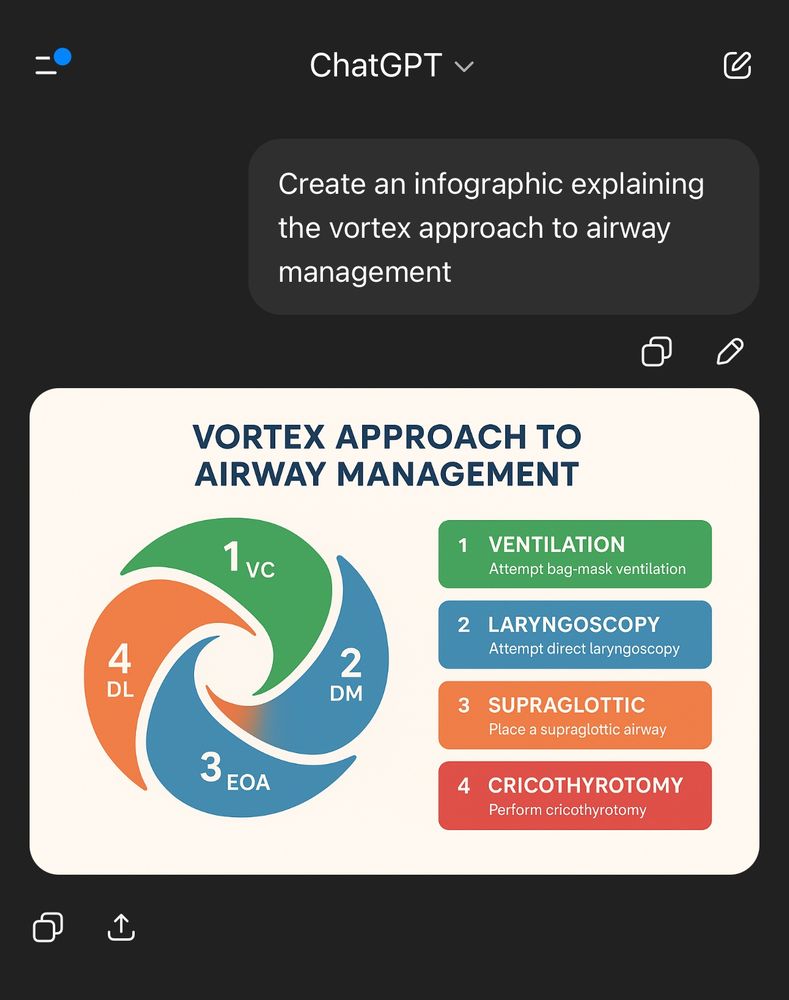
The incorporation of the Vortex into DAS 2018 was 3 fold:
1. Acknowledging the utility of the Vortex graphic as an adjunct to facilitate implementation of the guidelines.
2. The ability to approach choice of rescue lifelines non-linearly.
3. Prompts to optimise attempts
1. Acknowledging the utility of the Vortex graphic as an adjunct to facilitate implementation of the guidelines.
2. The ability to approach choice of rescue lifelines non-linearly.
3. Prompts to optimise attempts

August 31, 2025 at 12:25 AM
The incorporation of the Vortex into DAS 2018 was 3 fold:
1. Acknowledging the utility of the Vortex graphic as an adjunct to facilitate implementation of the guidelines.
2. The ability to approach choice of rescue lifelines non-linearly.
3. Prompts to optimise attempts
1. Acknowledging the utility of the Vortex graphic as an adjunct to facilitate implementation of the guidelines.
2. The ability to approach choice of rescue lifelines non-linearly.
3. Prompts to optimise attempts
You keep saying you use the DAS guidelines & never hear the Vortex mentioned, yet the Vortex is mentioned in both the 2015 & 2018 DAS guidelines. Perhaps the greatest support the Vortex has ever had has been from DAS. They’re adjuncts not alternatives.



August 30, 2025 at 5:46 PM
You keep saying you use the DAS guidelines & never hear the Vortex mentioned, yet the Vortex is mentioned in both the 2015 & 2018 DAS guidelines. Perhaps the greatest support the Vortex has ever had has been from DAS. They’re adjuncts not alternatives.
DAS acknowledged this in the 2015 @dasairway.bsky.social guidelines & incorporated the Vortex into their 2018 Critical Care guidelines.
das.uk.com/guidelines/d...
das.uk.com/guidelines/g...
das.uk.com/guidelines/d...
das.uk.com/guidelines/g...




August 30, 2025 at 7:22 AM
DAS acknowledged this in the 2015 @dasairway.bsky.social guidelines & incorporated the Vortex into their 2018 Critical Care guidelines.
das.uk.com/guidelines/d...
das.uk.com/guidelines/g...
das.uk.com/guidelines/d...
das.uk.com/guidelines/g...
SBP of 50mmHg is frightening.
This study shows middle cerebral artery blood flow velocity decreases 50% w *MAP* < 60mmHg
pubmed.ncbi.nlm.nih.gov/26879693/
This study shows middle cerebral artery blood flow velocity decreases 50% w *MAP* < 60mmHg
pubmed.ncbi.nlm.nih.gov/26879693/

August 16, 2025 at 9:50 AM
SBP of 50mmHg is frightening.
This study shows middle cerebral artery blood flow velocity decreases 50% w *MAP* < 60mmHg
pubmed.ncbi.nlm.nih.gov/26879693/
This study shows middle cerebral artery blood flow velocity decreases 50% w *MAP* < 60mmHg
pubmed.ncbi.nlm.nih.gov/26879693/
Didn’t we work out that the environmental impact of volatiles is actually “vanishingly small”?
pubmed.ncbi.nlm.nih.gov/38205585/
pubmed.ncbi.nlm.nih.gov/38205585/

August 11, 2025 at 10:30 AM
Didn’t we work out that the environmental impact of volatiles is actually “vanishingly small”?
pubmed.ncbi.nlm.nih.gov/38205585/
pubmed.ncbi.nlm.nih.gov/38205585/
Point 3 is the thrust of the editorial BUT to make that decision in a way that aligns with the patient’s rather than clinician’s values (thereby supporting patient autonomy rather than being paternalistic) a conversation about risk needs to be had.
![Merely giving the patient
information, rather than expert guidance, may produce
suboptimal decisions and unnecessary stress [21].
Preserving patient autonomy is achieved by ensuring a
patient’s care aligns with their personal values. Whether any
outcome constitutes a material risk to a particular individual
is influenced by an array of factors, including personality;
experience; culture; age; sex; career; and lifestyle. It is
important that the anaesthetist has the ability to recognise
when patient values and priorities differ from their own.
Determining this essentially requires a reversal of the flow of
information; rather than providing information so that the
patient can make decisions, the emphasis should be on
acquiring information so that the clinician can make
management decisions in line with the patient’s stated
values. This information may be derived during the consent
process, elsewhere in the patient consultation or from other
sources.](https://cdn.bsky.app/img/feed_thumbnail/plain/did:plc:zbaj5jk7jtux3cccy6owpofu/bafkreibb3ny4wfkeil7jwzhwrwjz6v4nbet4fdnwuhfa6iimlvrssy7fjm@jpeg)


![rpretive model´ [23] aligns with anaesthetic
care as it describes a circumstance where the patient is often
unaware of the relevant information and how their values
might affect the delivery of care. It allows the clinician to
determine the vulnerabilities and concerns of an individual
and then use their expertise to deliver the most appropriate
care, augmenting rather than diminishing patient
autonomy. This is consistent with the concept of autonomy
as a multidimensional capacity, requiring not only the
cognitive ability to make rational decisions but additional
aspects such as understanding, intentionality and freedom
from external constraints, which the patient may require
support from others to attain](https://cdn.bsky.app/img/feed_thumbnail/plain/did:plc:zbaj5jk7jtux3cccy6owpofu/bafkreiftrspmz2pzputq3ff3cfgcsmxk6farr2fy2n3quhgx74lc5jdvsq@jpeg)
August 6, 2025 at 5:06 PM
Point 3 is the thrust of the editorial BUT to make that decision in a way that aligns with the patient’s rather than clinician’s values (thereby supporting patient autonomy rather than being paternalistic) a conversation about risk needs to be had.
Except that:
1. You don’t necessarily have to have the surgery.
2. Even if you do have the surgery there are multiple ways to do the same thing, each with different risks, that can be chosen according to complications which the patient is particularly vulnerable to or concerned about.
1. You don’t necessarily have to have the surgery.
2. Even if you do have the surgery there are multiple ways to do the same thing, each with different risks, that can be chosen according to complications which the patient is particularly vulnerable to or concerned about.

August 6, 2025 at 4:06 AM
Except that:
1. You don’t necessarily have to have the surgery.
2. Even if you do have the surgery there are multiple ways to do the same thing, each with different risks, that can be chosen according to complications which the patient is particularly vulnerable to or concerned about.
1. You don’t necessarily have to have the surgery.
2. Even if you do have the surgery there are multiple ways to do the same thing, each with different risks, that can be chosen according to complications which the patient is particularly vulnerable to or concerned about.
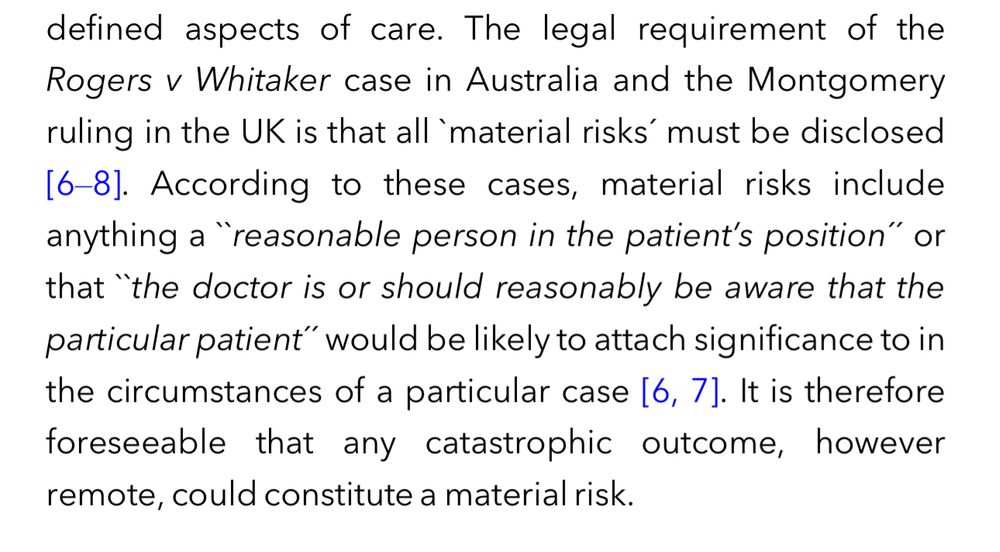
Montgomery also says "anything the clinician is or should reasonably be aware that a particular person would consider significant". So if you are aware or even suspect that a specific patient might have a particular (though objectively unreasonable) concern about, that's a material risk.
August 4, 2025 at 9:09 AM
Montgomery also says "anything the clinician is or should reasonably be aware that a particular person would consider significant". So if you are aware or even suspect that a specific patient might have a particular (though objectively unreasonable) concern about, that's a material risk.
I'm far too young to remember that. 😉
(actually I loved the Rockford Files speaking of James Garner)
(actually I loved the Rockford Files speaking of James Garner)
August 4, 2025 at 8:55 AM
I'm far too young to remember that. 😉
(actually I loved the Rockford Files speaking of James Garner)
(actually I loved the Rockford Files speaking of James Garner)
Awareness can be viewed as both a harmful outcome and a mechanism for harm. It's an unpleasant experience in its own right and a potential precipitant for psychological injury.
August 4, 2025 at 8:49 AM
Awareness can be viewed as both a harmful outcome and a mechanism for harm. It's an unpleasant experience in its own right and a potential precipitant for psychological injury.
That’s a common approach but anyone can have awareness & it’s entirely reasonable for a patient to say “if I’d known that was a risk, I wouldn’t have had this done” (or would have asked if you could have done things differently to reduce the likelihood) about any rare catastrophic risk.
August 3, 2025 at 8:07 PM
That’s a common approach but anyone can have awareness & it’s entirely reasonable for a patient to say “if I’d known that was a risk, I wouldn’t have had this done” (or would have asked if you could have done things differently to reduce the likelihood) about any rare catastrophic risk.
It doesn’t matter what the doctor considers a material risk, nor does it necessarily have to be a risk that a ‘reasonable person’ would consider material. It can just be something the doctor should reasonably be aware that a particular patient might consider significant (however unreasonably).

August 3, 2025 at 10:50 AM
It doesn’t matter what the doctor considers a material risk, nor does it necessarily have to be a risk that a ‘reasonable person’ would consider material. It can just be something the doctor should reasonably be aware that a particular patient might consider significant (however unreasonably).
Categorical terms are unhelpful in isolation but can be useful in assoc w descriptors to aid conceptualisation.
We speculate that it may be easier for pts to conceptualise likelihood if descriptors are framed in terms of how often clinicians encounter them cf proportion of pts experiencing them.
We speculate that it may be easier for pts to conceptualise likelihood if descriptors are framed in terms of how often clinicians encounter them cf proportion of pts experiencing them.

August 3, 2025 at 10:38 AM
Categorical terms are unhelpful in isolation but can be useful in assoc w descriptors to aid conceptualisation.
We speculate that it may be easier for pts to conceptualise likelihood if descriptors are framed in terms of how often clinicians encounter them cf proportion of pts experiencing them.
We speculate that it may be easier for pts to conceptualise likelihood if descriptors are framed in terms of how often clinicians encounter them cf proportion of pts experiencing them.
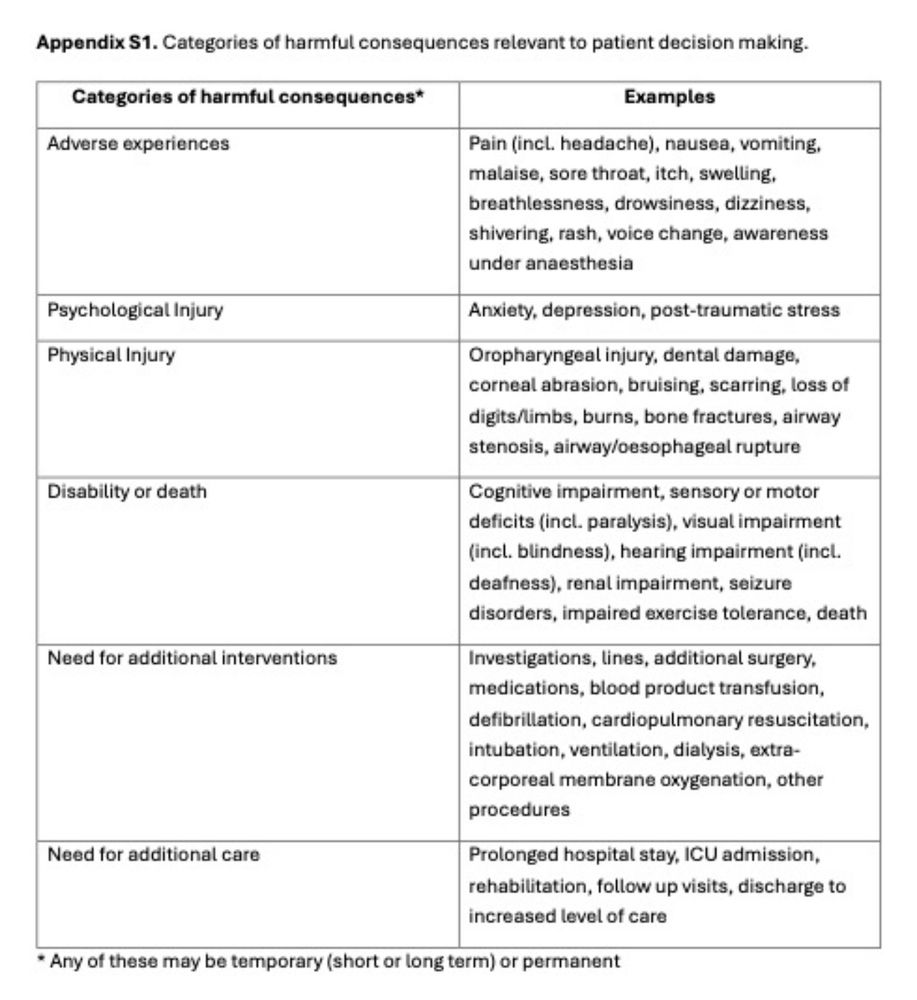
Here’s an example of how potentially harmful outcomes of anaesthesia can be categorised into 6 groups.
From ‘The paradox of informed consent’. Free for a limited time in @anaesjournal.bsky.social 🔓🔑⏳
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1...
From ‘The paradox of informed consent’. Free for a limited time in @anaesjournal.bsky.social 🔓🔑⏳
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1...

August 2, 2025 at 10:58 PM
Here’s an example of how potentially harmful outcomes of anaesthesia can be categorised into 6 groups.
From ‘The paradox of informed consent’. Free for a limited time in @anaesjournal.bsky.social 🔓🔑⏳
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1...
From ‘The paradox of informed consent’. Free for a limited time in @anaesjournal.bsky.social 🔓🔑⏳
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1...
Yet 70L/min (mouth closed) consistently provides ETO2 >90%
(while 70L/min mouth open is consistently crap)
(while 70L/min mouth open is consistently crap)



August 2, 2025 at 10:33 PM
Yet 70L/min (mouth closed) consistently provides ETO2 >90%
(while 70L/min mouth open is consistently crap)
(while 70L/min mouth open is consistently crap)
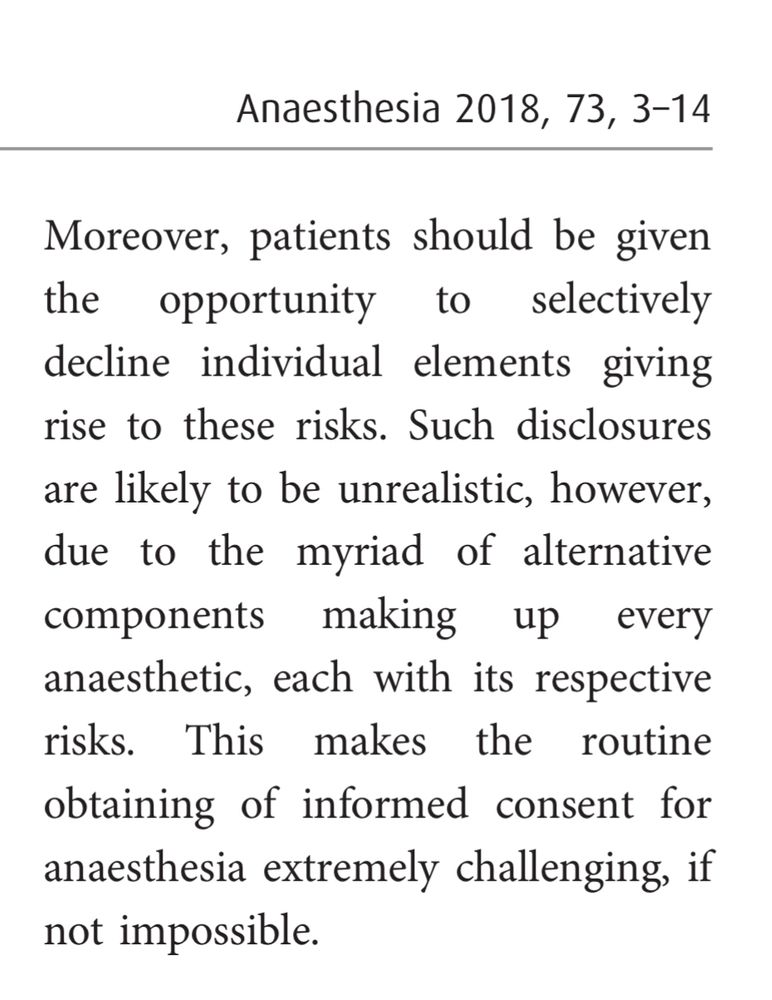
But as the uncommon risks are the catastrophic ones it’s very difficult to mount an argument that they don’t constitute ‘material risks’ to the patient that necessitate consent.
August 2, 2025 at 11:44 AM
But as the uncommon risks are the catastrophic ones it’s very difficult to mount an argument that they don’t constitute ‘material risks’ to the patient that necessitate consent.
When engaging in the consent process should we be alerting patients to *mechanisms* of harm or to harmful *outcomes*?
‘The paradox of informed consent’
Free full text in @anaesjournal.bsky.social for a limited time.
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1...
‘The paradox of informed consent’
Free full text in @anaesjournal.bsky.social for a limited time.
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1...

August 2, 2025 at 1:31 AM
When engaging in the consent process should we be alerting patients to *mechanisms* of harm or to harmful *outcomes*?
‘The paradox of informed consent’
Free full text in @anaesjournal.bsky.social for a limited time.
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1...
‘The paradox of informed consent’
Free full text in @anaesjournal.bsky.social for a limited time.
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/abs/10.1...
I’m simply floating an idea. Consenting for mechanisms of harm has always been the convention but we should examine why we do this & whether or not it contributes to autonomous decision making.
Perhaps we need to consent for consequences to the patient instead.
Perhaps we need to consent for consequences to the patient instead.
August 1, 2025 at 8:32 PM
I’m simply floating an idea. Consenting for mechanisms of harm has always been the convention but we should examine why we do this & whether or not it contributes to autonomous decision making.
Perhaps we need to consent for consequences to the patient instead.
Perhaps we need to consent for consequences to the patient instead.
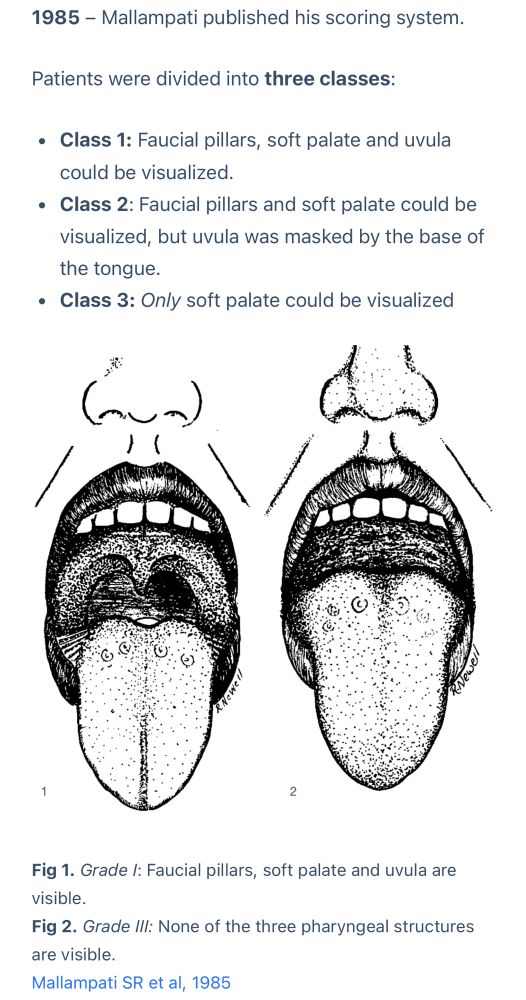
That’s a bit different from the original 1985 description.
Even after 3 got altered & 4 added w the Samsoon modification in 1987, I’ve never heard of the tonsils getting involved!
Even after 3 got altered & 4 added w the Samsoon modification in 1987, I’ve never heard of the tonsils getting involved!

July 31, 2025 at 11:07 PM
That’s a bit different from the original 1985 description.
Even after 3 got altered & 4 added w the Samsoon modification in 1987, I’ve never heard of the tonsils getting involved!
Even after 3 got altered & 4 added w the Samsoon modification in 1987, I’ve never heard of the tonsils getting involved!
From the ‘similar articles’ it seems it’s been done quite a lot, with a distinct theme emerging…
I love “fair interrater reliability beyond that expected by chance”. Really setting a low bar there.
ASA Status, not perfect but better than a coin toss!
I love “fair interrater reliability beyond that expected by chance”. Really setting a low bar there.
ASA Status, not perfect but better than a coin toss!




July 31, 2025 at 10:40 PM
From the ‘similar articles’ it seems it’s been done quite a lot, with a distinct theme emerging…
I love “fair interrater reliability beyond that expected by chance”. Really setting a low bar there.
ASA Status, not perfect but better than a coin toss!
I love “fair interrater reliability beyond that expected by chance”. Really setting a low bar there.
ASA Status, not perfect but better than a coin toss!