




Nicholas Chrimes
@chrimesy.com
Anaesthetist | Creator Vortex Approach | Co-founder Safe Airway Society | Director Universal Airway (PUMA) Guidelines | ANZCA/ASA/NZSA Airway SIG Executive Member
VortexApproach.org
UniversalAirway.org
SafeAirwaySociety.org
EZDrugID.org
VortexApproach.org
UniversalAirway.org
SafeAirwaySociety.org
EZDrugID.org
If you’re not going to use cricoid, you shouldn’t be doing RSI at all, just standard intubations on everyone.
November 15, 2025 at 7:07 PM
If you’re not going to use cricoid, you shouldn’t be doing RSI at all, just standard intubations on everyone.
No one has shown *in a randomised controlled trial* that it does what they say it will do (which is true of all components of RSI) but there’s lots of other experimental evidence that it blocks passage of material bw stomach & pharynx (whereas no other component of RSI has any evidence at all!).
November 15, 2025 at 7:04 PM
No one has shown *in a randomised controlled trial* that it does what they say it will do (which is true of all components of RSI) but there’s lots of other experimental evidence that it blocks passage of material bw stomach & pharynx (whereas no other component of RSI has any evidence at all!).
This is the original graphic before I simplified it. Pale blue lines represent lowest risk of cross reactivity.

November 14, 2025 at 2:38 AM
This is the original graphic before I simplified it. Pale blue lines represent lowest risk of cross reactivity.
Ideally refer for testing to find safe agents. Odd that this was not done during previous skin testing.
Otherwise pancuronium.
Otherwise pancuronium.

November 14, 2025 at 2:33 AM
Ideally refer for testing to find safe agents. Odd that this was not done during previous skin testing.
Otherwise pancuronium.
Otherwise pancuronium.
Reposted by Nicholas Chrimes
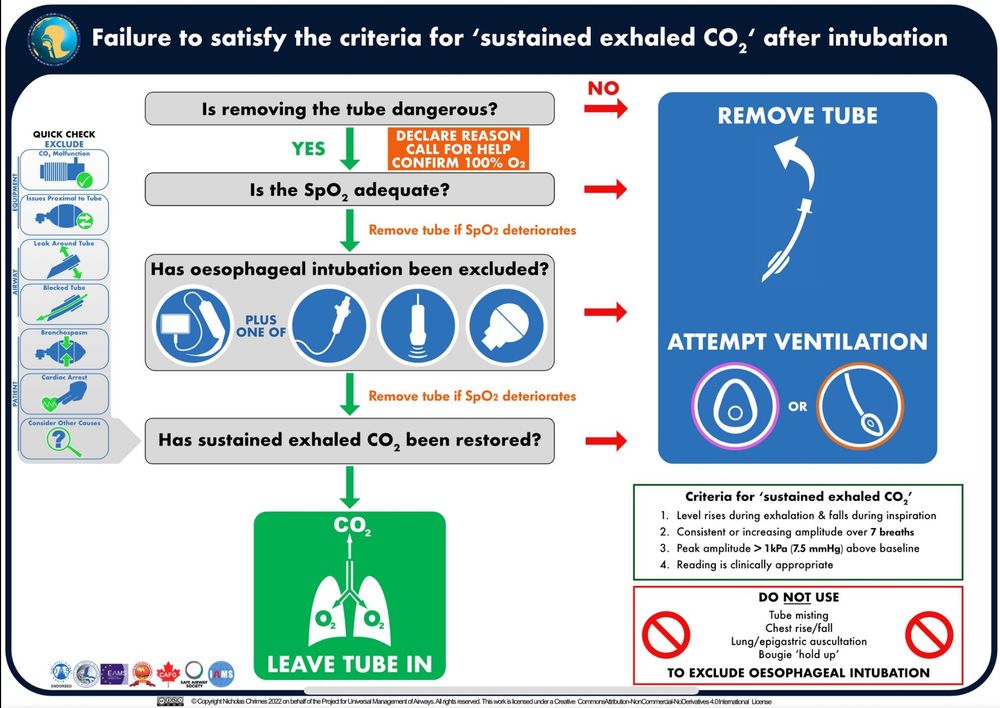
Awful. I'm just going to leave this here: yes, bronchospasm can account for a flat capnograph, but no, you can't assume that's the reason and you must take the tube out or (if that's genuinely dangerous) exclude oesophageal intubation using a bronchoscope.
onlinelibrary.wiley.com/share/author...
onlinelibrary.wiley.com/share/author...

September 1, 2025 at 11:22 AM
Awful. I'm just going to leave this here: yes, bronchospasm can account for a flat capnograph, but no, you can't assume that's the reason and you must take the tube out or (if that's genuinely dangerous) exclude oesophageal intubation using a bronchoscope.
onlinelibrary.wiley.com/share/author...
onlinelibrary.wiley.com/share/author...
Had enough of this conversation. See ya.
September 1, 2025 at 11:19 AM
Had enough of this conversation. See ya.
You seem intent on not revealing the secret meaning of virtue signalling.
September 1, 2025 at 11:17 AM
You seem intent on not revealing the secret meaning of virtue signalling.
Terrible analogy.
Why are you telling them you did that?
Why are you telling them you did that?
September 1, 2025 at 10:29 AM
Terrible analogy.
Why are you telling them you did that?
Why are you telling them you did that?
If you think you’re the exception to falling into the traps that recur (in the hands of good clinicians) in *every* case of unrecognised oesophageal intubation, you’re at risk of one day becoming the most dangerous person in the room.
Just follow the guideline.
Just follow the guideline.
September 1, 2025 at 10:25 AM
If you think you’re the exception to falling into the traps that recur (in the hands of good clinicians) in *every* case of unrecognised oesophageal intubation, you’re at risk of one day becoming the most dangerous person in the room.
Just follow the guideline.
Just follow the guideline.
I didn’t define virtue signalling, I simply stated that complaining about alt text was being used to virtue signal.

September 1, 2025 at 10:20 AM
I didn’t define virtue signalling, I simply stated that complaining about alt text was being used to virtue signal.
‘Bam!’ if I wasn’t using alt text. 🙄
September 1, 2025 at 10:13 AM
‘Bam!’ if I wasn’t using alt text. 🙄
I am doing it. That’s not the point.
September 1, 2025 at 10:11 AM
I am doing it. That’s not the point.
If you think it’s dangerous to remove the tube use a flexible bronchoscope to exclude oesophageal intubation.
September 1, 2025 at 10:10 AM
If you think it’s dangerous to remove the tube use a flexible bronchoscope to exclude oesophageal intubation.
Further there’s been cases where the tube has actually been going through the cords & then out through a damaged anterior tracheal wall into the mediastinum.
September 1, 2025 at 10:10 AM
Further there’s been cases where the tube has actually been going through the cords & then out through a damaged anterior tracheal wall into the mediastinum.
In EVERY case of unrecognised oesophageal intubation we reviewed, when the original intubator performed repeat laryngoscopy they incorrectly identified that the tube was in the trachea. Repeat laryngoscopy is to *identify* oesophageal intubation (& hasten tube removal) not to exclude it.
September 1, 2025 at 10:10 AM
In EVERY case of unrecognised oesophageal intubation we reviewed, when the original intubator performed repeat laryngoscopy they incorrectly identified that the tube was in the trachea. Repeat laryngoscopy is to *identify* oesophageal intubation (& hasten tube removal) not to exclude it.
Not in any way the same thing.
September 1, 2025 at 8:04 AM
Not in any way the same thing.
I’m already using it.
September 1, 2025 at 8:03 AM
I’m already using it.
The whole art of intubating w HAVL is knowing how far to pull the stylet back to allow the tube to advance around the secondary curve into the trachea: too little it won’t advance, too much it buckles above the cords. Has to be done by the operator not an assistant otherwise nuance lost.
Universal HAVL: 100% grade 1 view & 1st pass success since 2020. 😘👌
September 1, 2025 at 4:48 AM
The whole art of intubating w HAVL is knowing how far to pull the stylet back to allow the tube to advance around the secondary curve into the trachea: too little it won’t advance, too much it buckles above the cords. Has to be done by the operator not an assistant otherwise nuance lost.
Use vs follow. I like that.
August 31, 2025 at 8:07 AM
Use vs follow. I like that.
Then the problem was operator skill not the device.
August 31, 2025 at 8:07 AM
Then the problem was operator skill not the device.