



Razvan Azamfirei
@razvan.azamfirei.com
critical care | tweets mine (the good ones) | old man yelling at a cloud | @pennanesthesia | @HopkinsMedicine | @Yale | https://azamfirei.com
I finally caught up with my 8-week backlog of @criticalcarereviews.com emails. I'm unsurprised to say that nothing has changed.
This is totally not a sub-tweet directed at the Andromeda-Shock-2-stans.
This is totally not a sub-tweet directed at the Andromeda-Shock-2-stans.
October 31, 2025 at 2:50 AM
I finally caught up with my 8-week backlog of @criticalcarereviews.com emails. I'm unsurprised to say that nothing has changed.
This is totally not a sub-tweet directed at the Andromeda-Shock-2-stans.
This is totally not a sub-tweet directed at the Andromeda-Shock-2-stans.
This definitely comes with experience and feeling comfortable interpreting the data by yourself.
I always skip the introduction and go straight into the methods, followed by the results, last paragraph of the discussion ± supplement.
I always skip the introduction and go straight into the methods, followed by the results, last paragraph of the discussion ± supplement.
One of the most powerful skills you get with more and more experience is just understanding what you can ignore lol.
It’s made reading stats papers much easier 😂
It’s made reading stats papers much easier 😂
October 4, 2025 at 12:30 AM
This definitely comes with experience and feeling comfortable interpreting the data by yourself.
I always skip the introduction and go straight into the methods, followed by the results, last paragraph of the discussion ± supplement.
I always skip the introduction and go straight into the methods, followed by the results, last paragraph of the discussion ± supplement.
Reposted by Razvan Azamfirei

Yes. If you're worried about a lung fungus, mica/eraxis ain't it.
People reach for it because it's easy (where as vori/isavu/ampho aren't easy), but it's not useful here.
And if you think you found candida because your BAL said so....no you didn't.
People reach for it because it's easy (where as vori/isavu/ampho aren't easy), but it's not useful here.
And if you think you found candida because your BAL said so....no you didn't.

I sometimes see folks using echinocandins (micafungin et al) to cover "possible fungal pneumonia"
But, I'm not aware of *any* fungal pneumonias that can be treated adequately with echinocandin monotherapy 🤔
(I'm not counting Candida PNA because it has an incidence rate on par with Sasquatch)
But, I'm not aware of *any* fungal pneumonias that can be treated adequately with echinocandin monotherapy 🤔
(I'm not counting Candida PNA because it has an incidence rate on par with Sasquatch)

July 14, 2025 at 1:33 AM
Yes. If you're worried about a lung fungus, mica/eraxis ain't it.
People reach for it because it's easy (where as vori/isavu/ampho aren't easy), but it's not useful here.
And if you think you found candida because your BAL said so....no you didn't.
People reach for it because it's easy (where as vori/isavu/ampho aren't easy), but it's not useful here.
And if you think you found candida because your BAL said so....no you didn't.
What I value most about institutions of higher education is their moral compass, their natural inclination to speak truth to power, and how unflappable they are in the face of changing political winds.
March 20, 2025 at 1:41 AM
What I value most about institutions of higher education is their moral compass, their natural inclination to speak truth to power, and how unflappable they are in the face of changing political winds.
Dexmedetomidine-associated fever happens WAY more often than this, particularly in cardiac surgery patients.
Such an easy way to trick yourself into an unnecessary infectious workup and antibiotic course.
Such an easy way to trick yourself into an unnecessary infectious workup and antibiotic course.

2. Fever/Hyperthermia: happens probably in 5% of patients & is associated with higher/prolonged infusion rates. Some authors suggest that the opposite, fever control using a2-agonists in the settings of sepsis, may be related to hyperthermia-associated vasodilatation… 🤷♂️
February 16, 2025 at 7:56 PM
Dexmedetomidine-associated fever happens WAY more often than this, particularly in cardiac surgery patients.
Such an easy way to trick yourself into an unnecessary infectious workup and antibiotic course.
Such an easy way to trick yourself into an unnecessary infectious workup and antibiotic course.
The Hypotension-Prediction Index--a convoluted way of predicting hypotension by...checking whether the MAP is low--fails once again. Shocker.
"HPI-guided hemodynamic therapy did not reduce the incidence of postoperative AKI or overall complications [vs] standard care."
"HPI-guided hemodynamic therapy did not reduce the incidence of postoperative AKI or overall complications [vs] standard care."
Hemodynamic Management guided by the Hypotension Prediction ... : Anesthesiology
erate-to-high-risk elective abdominal surgery patients.
Methods:
This multicenter randomized trial was conducted from October 2022 to February 2024 across 28 hospitals evaluating HPI-guided managem...
journals.lww.com
February 1, 2025 at 3:26 AM
The Hypotension-Prediction Index--a convoluted way of predicting hypotension by...checking whether the MAP is low--fails once again. Shocker.
"HPI-guided hemodynamic therapy did not reduce the incidence of postoperative AKI or overall complications [vs] standard care."
"HPI-guided hemodynamic therapy did not reduce the incidence of postoperative AKI or overall complications [vs] standard care."
I'm just here for the DL/VL drama.
(this is pretty classic confounding by indication)
(this is pretty classic confounding by indication)

Published TODAY in @tandfonline BUMC Proceedings: Airway management of appendectomies
In this retrospective study, we found that most airways (88%) were managed with DL (97% 1st pass success) and that VL was less successful (76%) . VL pts were sicker🧵 #ansky
tandfonline.com/doi/full/10.10…
In this retrospective study, we found that most airways (88%) were managed with DL (97% 1st pass success) and that VL was less successful (76%) . VL pts were sicker🧵 #ansky
tandfonline.com/doi/full/10.10…

December 28, 2024 at 12:57 PM
I'm just here for the DL/VL drama.
(this is pretty classic confounding by indication)
(this is pretty classic confounding by indication)
Reposted by Razvan Azamfirei

Merry Christmas to everyone except for the people being unnecessarily pedantic about hypoxia and hypoxemia.
December 25, 2024 at 1:16 AM
Merry Christmas to everyone except for the people being unnecessarily pedantic about hypoxia and hypoxemia.
1) If you're looking for an excuse to deescalate (i.e., procalcitonin), just deescalate
2) I really want to see us move away from magic numbers (5, 7, 10, 14, etc.) but not sure that fixating on a different magic number is the way to go
2) I really want to see us move away from magic numbers (5, 7, 10, 14, etc.) but not sure that fixating on a different magic number is the way to go

Published in JAMA with #CCRdownunder:
In critically ill adults with suspected sepsis, antibiotic regimens were safely reduced when guided by measurement of procalcitonin but not by C-reactive protein. @criticalcarereviews.com
ja.ma/3BovM5v
In critically ill adults with suspected sepsis, antibiotic regimens were safely reduced when guided by measurement of procalcitonin but not by C-reactive protein. @criticalcarereviews.com
ja.ma/3BovM5v

December 9, 2024 at 11:28 PM
1) If you're looking for an excuse to deescalate (i.e., procalcitonin), just deescalate
2) I really want to see us move away from magic numbers (5, 7, 10, 14, etc.) but not sure that fixating on a different magic number is the way to go
2) I really want to see us move away from magic numbers (5, 7, 10, 14, etc.) but not sure that fixating on a different magic number is the way to go
Reposted by Razvan Azamfirei

“Professional ethics must guide us precisely when we are told that the situation is exceptional. Then there is no such thing as ‘just following orders.’”
~ Timothy Snyder
~ Timothy Snyder
December 7, 2024 at 9:20 PM
“Professional ethics must guide us precisely when we are told that the situation is exceptional. Then there is no such thing as ‘just following orders.’”
~ Timothy Snyder
~ Timothy Snyder
This is incredibly disturbing.

NEW: “Eat What You Kill”
Hailed as a savior upon his arrival in Helena, Dr. Thomas C. Weiner became a favorite of patients and his hospital’s highest earner. As the myth surrounding the high-profile oncologist grew, so did the trail of patient harm and suspicious deaths. @davidmcswane.bsky.social
Hailed as a savior upon his arrival in Helena, Dr. Thomas C. Weiner became a favorite of patients and his hospital’s highest earner. As the myth surrounding the high-profile oncologist grew, so did the trail of patient harm and suspicious deaths. @davidmcswane.bsky.social
A Hospital Helped a Beloved Doctor’s Practice Flourish Even as It Suspected He Was Hurting Patients
Hailed as a savior upon his arrival in Helena, Dr. Thomas C. Weiner became a favorite of patients and his hospital’s highest earner. As the myth surrounding the high-profile oncologist grew, so did…
propub.li
December 7, 2024 at 7:48 PM
This is incredibly disturbing.
Reposted by Razvan Azamfirei
A patient presented in need of an urgent but relatively minor surgery. Vitally stable.
Surgery goes fine, but ICU is called because their “sat is too low to extubate.”
No prior pulmonary or cardiac conditions.
#emimcc
Surgery goes fine, but ICU is called because their “sat is too low to extubate.”
No prior pulmonary or cardiac conditions.
#emimcc
November 30, 2024 at 11:07 PM
A patient presented in need of an urgent but relatively minor surgery. Vitally stable.
Surgery goes fine, but ICU is called because their “sat is too low to extubate.”
No prior pulmonary or cardiac conditions.
#emimcc
Surgery goes fine, but ICU is called because their “sat is too low to extubate.”
No prior pulmonary or cardiac conditions.
#emimcc
I'm just waiting for the day when we finally stop teaching people that pressors don’t work in acidotic patients.
November 26, 2024 at 2:55 AM
I'm just waiting for the day when we finally stop teaching people that pressors don’t work in acidotic patients.
I don’t have strong opinions about the result, but this study is grossly underpowered. I would not draw any definitive inferences from it.
❇️ Best of Surgical Critical Care❇️
A study was done to determine if adding ketamine to multi-modal analgesics improved pain control in adult blunt trauma patients with rib fractures. Ketamine infusion didn't decrease opiate use & its routine use is not recommended.
journals.lww.com/jtrauma/full...
A study was done to determine if adding ketamine to multi-modal analgesics improved pain control in adult blunt trauma patients with rib fractures. Ketamine infusion didn't decrease opiate use & its routine use is not recommended.
journals.lww.com/jtrauma/full...

November 22, 2024 at 7:13 PM
I don’t have strong opinions about the result, but this study is grossly underpowered. I would not draw any definitive inferences from it.
Reposted by Razvan Azamfirei
I add a couple of people every day but there are many more of you who work with critically ill patients. Drop a comment here and I'll add you! But check to see if you're already on it first 😁 go.bsky.app/NC7iD2K
November 17, 2024 at 1:17 PM
I add a couple of people every day but there are many more of you who work with critically ill patients. Drop a comment here and I'll add you! But check to see if you're already on it first 😁 go.bsky.app/NC7iD2K
Renal: "We must keep the correction rate below 12 mEq/day, but to avoid overcorrection/this is a high risk patient, we're going to recommend 8 mEq/day."
Primary team: "Wait—ODS is (really) bad, so we'll do 6 mEq/day."
Maybe this is will be the impetus for some high-quality prospective studies.
Primary team: "Wait—ODS is (really) bad, so we'll do 6 mEq/day."
Maybe this is will be the impetus for some high-quality prospective studies.

Honey, stop what you're doing, new hyponatremia research just dropped!
What's it say?
It looks like slow correction is associated with worse outcomes, like death and length of stay!
Was it just a small study?
No, it was a meta-analysis of almost 12,000 patients!
jamanetwork.com/journals/jam...
What's it say?
It looks like slow correction is associated with worse outcomes, like death and length of stay!
Was it just a small study?
No, it was a meta-analysis of almost 12,000 patients!
jamanetwork.com/journals/jam...
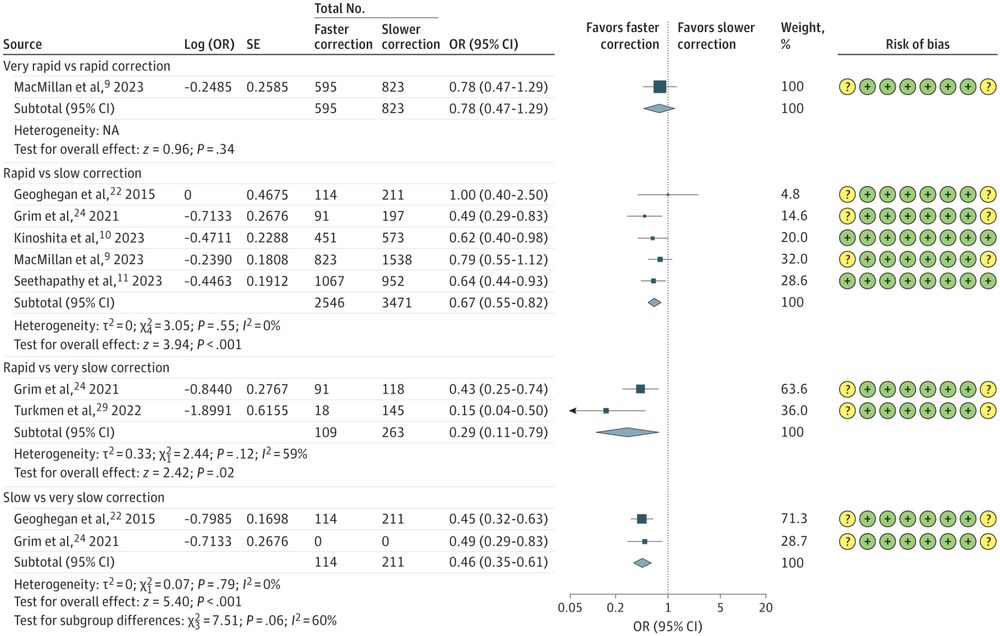
Correction Rates and Clinical Outcomes in Hospitalized Adults With Severe Hyponatremia
This systematic review and meta-analysis evaluates the association of sodium correction rates with mortality among hospitalized adults with severe hyponatremia.
jamanetwork.com
November 19, 2024 at 1:31 PM
Renal: "We must keep the correction rate below 12 mEq/day, but to avoid overcorrection/this is a high risk patient, we're going to recommend 8 mEq/day."
Primary team: "Wait—ODS is (really) bad, so we'll do 6 mEq/day."
Maybe this is will be the impetus for some high-quality prospective studies.
Primary team: "Wait—ODS is (really) bad, so we'll do 6 mEq/day."
Maybe this is will be the impetus for some high-quality prospective studies.
Spiciest opinion of the day! Can we still use negative binomial if we don't know how to spell poission though?

Given the #Rstats base vs tidy wars have been reignited, I want to create a new front for #statsky: poisson vs. negative binomial regression.
I firmly believe you should almost never use NB. My reasoning: stats.stackexchange.com/a/653731/116...
And always use a robust/bootstrap SE with poisson!
I firmly believe you should almost never use NB. My reasoning: stats.stackexchange.com/a/653731/116...
And always use a robust/bootstrap SE with poisson!

When to use negative binomial and Poisson regression
When would one use a negative binomial regression and when would one use Poisson regression with respect to the mean and variance?
stats.stackexchange.com
November 19, 2024 at 2:39 AM
Spiciest opinion of the day! Can we still use negative binomial if we don't know how to spell poission though?
One of the most amusing things in medicine is seeing how people dismiss high-quality evidence when it challenges their preferred practices (e.g., robotic surgery, regional anesthesia, TAVRs, TTM, etc.).
November 17, 2024 at 8:33 PM
One of the most amusing things in medicine is seeing how people dismiss high-quality evidence when it challenges their preferred practices (e.g., robotic surgery, regional anesthesia, TAVRs, TTM, etc.).
This common belief isn't entirely accurate. In acute blood loss, fluid shifts happen quickly—hemoglobin decreases in < 30 minutes, even without IV fluids.
The levels won't reflect the magnitude of the blood loss, but someone who lost 40% TBV will not have a normal hemoglobin. https://t.co/59...
The levels won't reflect the magnitude of the blood loss, but someone who lost 40% TBV will not have a normal hemoglobin. https://t.co/59...
November 19, 2024 at 2:33 AM
This common belief isn't entirely accurate. In acute blood loss, fluid shifts happen quickly—hemoglobin decreases in < 30 minutes, even without IV fluids.
The levels won't reflect the magnitude of the blood loss, but someone who lost 40% TBV will not have a normal hemoglobin. https://t.co/59...
The levels won't reflect the magnitude of the blood loss, but someone who lost 40% TBV will not have a normal hemoglobin. https://t.co/59...
Without exaggeration, the font change on PubMed Central by @NCBI is probably the worst thing to have ever happened to science in the history of science.
November 19, 2024 at 2:33 AM
Without exaggeration, the font change on PubMed Central by @NCBI is probably the worst thing to have ever happened to science in the history of science.
Here's your friendly reminder that Plasmalyte is NOT affected by the IV Fluid Shortage, just in case you needed another reason to switch.
November 19, 2024 at 2:32 AM
Here's your friendly reminder that Plasmalyte is NOT affected by the IV Fluid Shortage, just in case you needed another reason to switch.
Looks like we’re still trying to make REBOA happen. 🙃
Regardless, this graph is a bit misleading. Neither B nor C survived to discharge, but not mentioned in the graph. https://twitter.com/JAMASurgery/status/1838518771805233592
Regardless, this graph is a bit misleading. Neither B nor C survived to discharge, but not mentioned in the graph. https://twitter.com/JAMASurgery/status/1838518771805233592
November 19, 2024 at 2:32 AM
Looks like we’re still trying to make REBOA happen. 🙃
Regardless, this graph is a bit misleading. Neither B nor C survived to discharge, but not mentioned in the graph. https://twitter.com/JAMASurgery/status/1838518771805233592
Regardless, this graph is a bit misleading. Neither B nor C survived to discharge, but not mentioned in the graph. https://twitter.com/JAMASurgery/status/1838518771805233592
At least it’s not Xuebijing again. https://twitter.com/giovannilandoni/status/1837176108585996518
November 19, 2024 at 2:32 AM
At least it’s not Xuebijing again. https://twitter.com/giovannilandoni/status/1837176108585996518
It's #WorldSepsisDay. Did you remember to order your 30mL/kg normal saline boluses?
November 19, 2024 at 2:32 AM
It's #WorldSepsisDay. Did you remember to order your 30mL/kg normal saline boluses?