



@seanbademian.bsky.social
Reposted

Ten things that -for no good reason- we don't do in the ICU:
OK, in general a "less is more" approach is reasonable & there is a "rationale" behind many of the following but the truth is that they don't make sense if scrutinized
Here it begins:
1. Holding tube feeds or any nutrition,
OK, in general a "less is more" approach is reasonable & there is a "rationale" behind many of the following but the truth is that they don't make sense if scrutinized
Here it begins:
1. Holding tube feeds or any nutrition,
August 24, 2025 at 2:56 PM
Ten things that -for no good reason- we don't do in the ICU:
OK, in general a "less is more" approach is reasonable & there is a "rationale" behind many of the following but the truth is that they don't make sense if scrutinized
Here it begins:
1. Holding tube feeds or any nutrition,
OK, in general a "less is more" approach is reasonable & there is a "rationale" behind many of the following but the truth is that they don't make sense if scrutinized
Here it begins:
1. Holding tube feeds or any nutrition,
Reposted

P-values are fraught with hazard, but SO IS BAYESIAN STATISTICS
the Achilles heel of Bayesian stats is that someone determines a pre-test probability distribution (usually arbitrarily)
The pre-test probability is often too high
This inflates the final posterior probability
🧵 #1/4 #EMIMCC
the Achilles heel of Bayesian stats is that someone determines a pre-test probability distribution (usually arbitrarily)
The pre-test probability is often too high
This inflates the final posterior probability
🧵 #1/4 #EMIMCC

August 14, 2025 at 12:10 PM
P-values are fraught with hazard, but SO IS BAYESIAN STATISTICS
the Achilles heel of Bayesian stats is that someone determines a pre-test probability distribution (usually arbitrarily)
The pre-test probability is often too high
This inflates the final posterior probability
🧵 #1/4 #EMIMCC
the Achilles heel of Bayesian stats is that someone determines a pre-test probability distribution (usually arbitrarily)
The pre-test probability is often too high
This inflates the final posterior probability
🧵 #1/4 #EMIMCC
Reposted
(Basic) ICU Hemodynamic “Secrets” - Part1:
I know you know them, but let’s remind ourselves of some basic hemodynamic "secrets":
I know you know them, but let’s remind ourselves of some basic hemodynamic "secrets":
August 16, 2025 at 6:23 PM
(Basic) ICU Hemodynamic “Secrets” - Part1:
I know you know them, but let’s remind ourselves of some basic hemodynamic "secrets":
I know you know them, but let’s remind ourselves of some basic hemodynamic "secrets":
Reposted
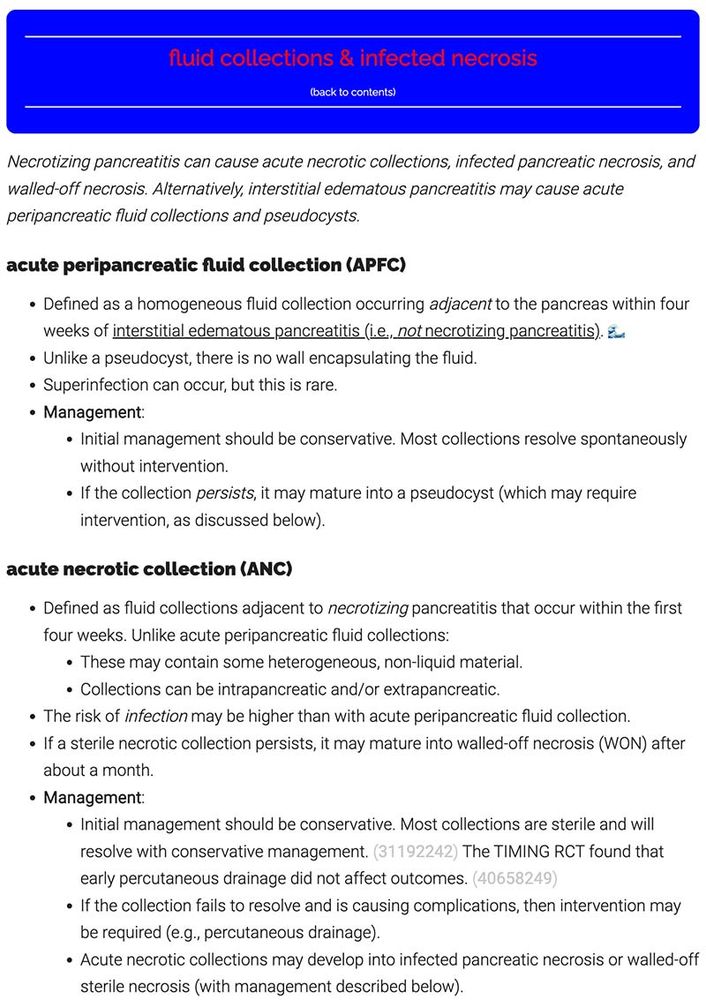
new RCT just came out on the management of acute necrotic collections (ANC) that may complicate necrotizing pancreatitis
ANCs are early sterile collections containing fluid and sometimes debris
they *lack* a well-defined wall (unlike pseudocysts or walled-off necrosis)...
🧵 #1/ #EMIMCC
ANCs are early sterile collections containing fluid and sometimes debris
they *lack* a well-defined wall (unlike pseudocysts or walled-off necrosis)...
🧵 #1/ #EMIMCC
August 2, 2025 at 1:27 PM
new RCT just came out on the management of acute necrotic collections (ANC) that may complicate necrotizing pancreatitis
ANCs are early sterile collections containing fluid and sometimes debris
they *lack* a well-defined wall (unlike pseudocysts or walled-off necrosis)...
🧵 #1/ #EMIMCC
ANCs are early sterile collections containing fluid and sometimes debris
they *lack* a well-defined wall (unlike pseudocysts or walled-off necrosis)...
🧵 #1/ #EMIMCC
Reposted
just learned this & mind blown 🤯
CKD-EPI, MDRD etc give us GFR corrected for body surface area (ml/min/1.73m2)
BUT we're supposed to use the *absolute* GFR (ml/min) for drug dosing (eg KDIGO 2024 guidelines below; FDA agrees)
in obesity, the computer's ml/min/1.73m2 can be way too low #EMIMCC
CKD-EPI, MDRD etc give us GFR corrected for body surface area (ml/min/1.73m2)
BUT we're supposed to use the *absolute* GFR (ml/min) for drug dosing (eg KDIGO 2024 guidelines below; FDA agrees)
in obesity, the computer's ml/min/1.73m2 can be way too low #EMIMCC

April 14, 2025 at 3:01 PM
just learned this & mind blown 🤯
CKD-EPI, MDRD etc give us GFR corrected for body surface area (ml/min/1.73m2)
BUT we're supposed to use the *absolute* GFR (ml/min) for drug dosing (eg KDIGO 2024 guidelines below; FDA agrees)
in obesity, the computer's ml/min/1.73m2 can be way too low #EMIMCC
CKD-EPI, MDRD etc give us GFR corrected for body surface area (ml/min/1.73m2)
BUT we're supposed to use the *absolute* GFR (ml/min) for drug dosing (eg KDIGO 2024 guidelines below; FDA agrees)
in obesity, the computer's ml/min/1.73m2 can be way too low #EMIMCC
Reposted
is contrast nephropathy in the room with us right now?
another article showing that contrast nephropathy isn’t a thing
I wonder how long these articles will keep getting published, since I kinda thought this was settled 🤷♂️
https://www.jem-journal.com/article/S0736-4679(24)00372-X/abstract #EMIMCC
another article showing that contrast nephropathy isn’t a thing
I wonder how long these articles will keep getting published, since I kinda thought this was settled 🤷♂️
https://www.jem-journal.com/article/S0736-4679(24)00372-X/abstract #EMIMCC


April 10, 2025 at 11:46 PM
is contrast nephropathy in the room with us right now?
another article showing that contrast nephropathy isn’t a thing
I wonder how long these articles will keep getting published, since I kinda thought this was settled 🤷♂️
https://www.jem-journal.com/article/S0736-4679(24)00372-X/abstract #EMIMCC
another article showing that contrast nephropathy isn’t a thing
I wonder how long these articles will keep getting published, since I kinda thought this was settled 🤷♂️
https://www.jem-journal.com/article/S0736-4679(24)00372-X/abstract #EMIMCC
Reposted
fantastic investigator thread about delving deeper into the BALANCE trial (7 vs 14 day antibiotics for bacteremia) to look for heterogeneity of treatment effect 😁
I was allready a BALANCE trial fanboy… this analysis makes it even more appealing. #EMIMCC
I was allready a BALANCE trial fanboy… this analysis makes it even more appealing. #EMIMCC

Excited to share our newest paper from my PhD: a post-hoc analysis of the BALANCE trial where we explored heterogeneity of treatment effect (HTE) in duration of antibiotic treatment for patients with bloodstream infection. A thread:
doi.org/10.1016/j.ec...
#IDSky @eclinicalmed.bsky.social
doi.org/10.1016/j.ec...
#IDSky @eclinicalmed.bsky.social
Redirecting
doi.org
April 11, 2025 at 11:16 PM
fantastic investigator thread about delving deeper into the BALANCE trial (7 vs 14 day antibiotics for bacteremia) to look for heterogeneity of treatment effect 😁
I was allready a BALANCE trial fanboy… this analysis makes it even more appealing. #EMIMCC
I was allready a BALANCE trial fanboy… this analysis makes it even more appealing. #EMIMCC
Reposted
April 6, 2025 at 7:29 PM
Reposted
Our old friend @zentensivist.bsky.social gives us a masterclass in the advanced tricks of PA catheter placement icuscenarios.com/lightning-ro...
#medsky #emimcc
#medsky #emimcc
Lightning rounds 50: Mastering PA catheter placement with Matt Siuba – Critical Care Scenarios
icuscenarios.com
March 5, 2025 at 2:59 PM
Our old friend @zentensivist.bsky.social gives us a masterclass in the advanced tricks of PA catheter placement icuscenarios.com/lightning-ro...
#medsky #emimcc
#medsky #emimcc
Reposted
ICU Hemodynamic Secrets:
Whenever I manage a critically ill patient, I am interested in knowing the blood pressure & at least an estimate of the cardiac output (CO). Since placing a pulmonary artery catheter takes some time & effort, I am usually employing workarounds based on #POCUS:
Whenever I manage a critically ill patient, I am interested in knowing the blood pressure & at least an estimate of the cardiac output (CO). Since placing a pulmonary artery catheter takes some time & effort, I am usually employing workarounds based on #POCUS:

March 2, 2025 at 6:33 PM
ICU Hemodynamic Secrets:
Whenever I manage a critically ill patient, I am interested in knowing the blood pressure & at least an estimate of the cardiac output (CO). Since placing a pulmonary artery catheter takes some time & effort, I am usually employing workarounds based on #POCUS:
Whenever I manage a critically ill patient, I am interested in knowing the blood pressure & at least an estimate of the cardiac output (CO). Since placing a pulmonary artery catheter takes some time & effort, I am usually employing workarounds based on #POCUS:
Reposted

Dr Rola and Haycock on APRV paper
'Zou et al. Physiologic APRV-TCAV Study: Our Thoughts'
#pulmsky #critcaresky #emimcc
.
vimeo.com/1061864674
'Zou et al. Physiologic APRV-TCAV Study: Our Thoughts'
#pulmsky #critcaresky #emimcc
.
vimeo.com/1061864674

Zou et al. Physiologic APRV-TCAV Study: Our Thoughts. #FOAMed #FOAMcc
This is "Zou et al. Physiologic APRV-TCAV Study: Our Thoughts. #FOAMed #FOAMcc" by @ThinkingCC / CCUS Institute on Vimeo, the home for high quality videos…
vimeo.com
March 3, 2025 at 12:02 AM
Dr Rola and Haycock on APRV paper
'Zou et al. Physiologic APRV-TCAV Study: Our Thoughts'
#pulmsky #critcaresky #emimcc
.
vimeo.com/1061864674
'Zou et al. Physiologic APRV-TCAV Study: Our Thoughts'
#pulmsky #critcaresky #emimcc
.
vimeo.com/1061864674
Reposted

I had the pleasure of teaching lung #pocus at a “train the trainers” course, with the ever excellent @avkwong.bsky.social and Cian McDermott as faculty
Some reflections from the day:
(1/n)
Some reflections from the day:
(1/n)
February 27, 2025 at 9:45 AM
I had the pleasure of teaching lung #pocus at a “train the trainers” course, with the ever excellent @avkwong.bsky.social and Cian McDermott as faculty
Some reflections from the day:
(1/n)
Some reflections from the day:
(1/n)
Reposted
version for new AF in ICU pt who needs urgent (not emergent) cardioversion:
1) start protocoled Mg gtt 1 g/hr
2) amio load & gtt
3) wait a few hrs
4) 1 mg ibutilide
5) if still in AF: DCCV
meds build up & work together
Mg/ibutilide/amio are synergistic
Mg prevents ibutilide-induced TdP #EMIMCC
1) start protocoled Mg gtt 1 g/hr
2) amio load & gtt
3) wait a few hrs
4) 1 mg ibutilide
5) if still in AF: DCCV
meds build up & work together
Mg/ibutilide/amio are synergistic
Mg prevents ibutilide-induced TdP #EMIMCC

Recent Onset AF Cardioversion:
- Amiodarone: Success rate 60-65%, delayed onset
- Procainamide: Success rate 60-65%, works (or doesn’t) in ~ 60 min
- Electricity: 95-97% success rate, immediate, no side effects
#MedSky #EMIMCC
youtube.com/shorts/cRAtL...
- Amiodarone: Success rate 60-65%, delayed onset
- Procainamide: Success rate 60-65%, works (or doesn’t) in ~ 60 min
- Electricity: 95-97% success rate, immediate, no side effects
#MedSky #EMIMCC
youtube.com/shorts/cRAtL...

AF Cardioversion #criticalcare #emergencymedicine #resuscitation #cardiology
YouTube video by EMSwami
youtube.com
February 11, 2025 at 11:34 PM
version for new AF in ICU pt who needs urgent (not emergent) cardioversion:
1) start protocoled Mg gtt 1 g/hr
2) amio load & gtt
3) wait a few hrs
4) 1 mg ibutilide
5) if still in AF: DCCV
meds build up & work together
Mg/ibutilide/amio are synergistic
Mg prevents ibutilide-induced TdP #EMIMCC
1) start protocoled Mg gtt 1 g/hr
2) amio load & gtt
3) wait a few hrs
4) 1 mg ibutilide
5) if still in AF: DCCV
meds build up & work together
Mg/ibutilide/amio are synergistic
Mg prevents ibutilide-induced TdP #EMIMCC
Reposted

1/
One of the BIGGEST #POCUS misconceptions is that B lines 🟰 pulmonary edema 🤦♀️
Did you know that there is actually a wide DDx for B lines?
Check out my latest video about #LungUltrasound for interstitial syndromes 👀; or read on for the highlights 👇 🧵
#emimcc
www.youtube.com/watch?v=eSuA...
One of the BIGGEST #POCUS misconceptions is that B lines 🟰 pulmonary edema 🤦♀️
Did you know that there is actually a wide DDx for B lines?
Check out my latest video about #LungUltrasound for interstitial syndromes 👀; or read on for the highlights 👇 🧵
#emimcc
www.youtube.com/watch?v=eSuA...

Lung Ultrasound for Interstitial Syndromes
YouTube video by UBC IM POCUS
www.youtube.com
February 6, 2025 at 6:33 PM
1/
One of the BIGGEST #POCUS misconceptions is that B lines 🟰 pulmonary edema 🤦♀️
Did you know that there is actually a wide DDx for B lines?
Check out my latest video about #LungUltrasound for interstitial syndromes 👀; or read on for the highlights 👇 🧵
#emimcc
www.youtube.com/watch?v=eSuA...
One of the BIGGEST #POCUS misconceptions is that B lines 🟰 pulmonary edema 🤦♀️
Did you know that there is actually a wide DDx for B lines?
Check out my latest video about #LungUltrasound for interstitial syndromes 👀; or read on for the highlights 👇 🧵
#emimcc
www.youtube.com/watch?v=eSuA...
Reposted

As someone who is a fan of both decremental PEEP trials & monitoring P0.1 this paper is 🫶
Trying to personalise PEEP during PSV is tough, & we don’t all have EIT/oesophageal manometry!
Pick the PEEP resulting in lowest P0.1, makes a lot of sense 😬
link.springer.com/article/10.1...
#EMIMCC
Trying to personalise PEEP during PSV is tough, & we don’t all have EIT/oesophageal manometry!
Pick the PEEP resulting in lowest P0.1, makes a lot of sense 😬
link.springer.com/article/10.1...
#EMIMCC

Personalized positive end-expiratory pressure in spontaneously breathing patients with acute respiratory distress syndrome by simultaneous electrical impedance tomography and transpulmonary pressure m...
Purpose Personalized positive end-expiratory pressure (PEEP) might foster lung and diaphragm protection in patients with acute respiratory distress syndrome (ARDS) who are undergoing pressure support ...
link.springer.com
February 3, 2025 at 8:09 PM
As someone who is a fan of both decremental PEEP trials & monitoring P0.1 this paper is 🫶
Trying to personalise PEEP during PSV is tough, & we don’t all have EIT/oesophageal manometry!
Pick the PEEP resulting in lowest P0.1, makes a lot of sense 😬
link.springer.com/article/10.1...
#EMIMCC
Trying to personalise PEEP during PSV is tough, & we don’t all have EIT/oesophageal manometry!
Pick the PEEP resulting in lowest P0.1, makes a lot of sense 😬
link.springer.com/article/10.1...
#EMIMCC
Reposted

The late, great Dr. Gattinoni dedicated his life to medicine, and his focus on respiratory failure is awe-inspiring. This short, three-page paper illustrates the journey of PEEP. 🎩 tip to the authors.
eddyjoemd.com/foamed
eddyjoemd.com/foamed

February 3, 2025 at 11:13 AM
The late, great Dr. Gattinoni dedicated his life to medicine, and his focus on respiratory failure is awe-inspiring. This short, three-page paper illustrates the journey of PEEP. 🎩 tip to the authors.
eddyjoemd.com/foamed
eddyjoemd.com/foamed


Reposted
milrinone pharmacology drives me crazy
half-life is ~2 hrs (longer in renal dysfunction, which our patients often have)
without a bolus, levels won't hit steady state for >4 hr
how does it make mathematical sense to give this drug without a bolus in an acutely sick patient?
🧵#1/2
half-life is ~2 hrs (longer in renal dysfunction, which our patients often have)
without a bolus, levels won't hit steady state for >4 hr
how does it make mathematical sense to give this drug without a bolus in an acutely sick patient?
🧵#1/2

January 27, 2025 at 2:13 PM
milrinone pharmacology drives me crazy
half-life is ~2 hrs (longer in renal dysfunction, which our patients often have)
without a bolus, levels won't hit steady state for >4 hr
how does it make mathematical sense to give this drug without a bolus in an acutely sick patient?
🧵#1/2
half-life is ~2 hrs (longer in renal dysfunction, which our patients often have)
without a bolus, levels won't hit steady state for >4 hr
how does it make mathematical sense to give this drug without a bolus in an acutely sick patient?
🧵#1/2
Reposted

Cardiogenic Shock After Acute Myocardial Infarction ― Revascularization, Mechanical Support & Beyond
CCR Journal Watch
criticalcarereviews.com/latest-evide...
Get the latest critical care literature every weekend via the CCR Newsletter - subscribe at criticalcarereviews.com/newsletters/...
CCR Journal Watch
criticalcarereviews.com/latest-evide...
Get the latest critical care literature every weekend via the CCR Newsletter - subscribe at criticalcarereviews.com/newsletters/...

January 14, 2025 at 10:41 AM
Cardiogenic Shock After Acute Myocardial Infarction ― Revascularization, Mechanical Support & Beyond
CCR Journal Watch
criticalcarereviews.com/latest-evide...
Get the latest critical care literature every weekend via the CCR Newsletter - subscribe at criticalcarereviews.com/newsletters/...
CCR Journal Watch
criticalcarereviews.com/latest-evide...
Get the latest critical care literature every weekend via the CCR Newsletter - subscribe at criticalcarereviews.com/newsletters/...
Reposted
I am SO thrilled to share this paper, which has truly been a labour of love on a topic I care about deeply.
"Demystifying Volume Status: An Ultrasound-Guided Physiologic Framework," now published online in @accpchest
Let us know what you think!
#emimcc
journal.chestnet.org/article/S001...
"Demystifying Volume Status: An Ultrasound-Guided Physiologic Framework," now published online in @accpchest
Let us know what you think!
#emimcc
journal.chestnet.org/article/S001...
Demystifying Volume Status: An Ultrasound-Guided Physiologic Framework
Accurate assessment of a patient’s volume status is crucial in many conditions, informing
decisions on fluid prescribing, vasoactive agents, and decongestive therapies. Determining
a patient’s volume ...
journal.chestnet.org
January 13, 2025 at 4:47 PM
I am SO thrilled to share this paper, which has truly been a labour of love on a topic I care about deeply.
"Demystifying Volume Status: An Ultrasound-Guided Physiologic Framework," now published online in @accpchest
Let us know what you think!
#emimcc
journal.chestnet.org/article/S001...
"Demystifying Volume Status: An Ultrasound-Guided Physiologic Framework," now published online in @accpchest
Let us know what you think!
#emimcc
journal.chestnet.org/article/S001...
Reposted
love this 😍
I've been promoting a roc-first strategy but I often get pushback implying that I'm an evil, inhumane ogre
but it works well & there's now data to support
if you disagree, pls direct all anger at @emswami.bsky.social
*ducks and runs*
(rationale: emcrit.org/pulmcrit/pul...) #EMIMCC
I've been promoting a roc-first strategy but I often get pushback implying that I'm an evil, inhumane ogre
but it works well & there's now data to support
if you disagree, pls direct all anger at @emswami.bsky.social
*ducks and runs*
(rationale: emcrit.org/pulmcrit/pul...) #EMIMCC
RSI Med Sequencing:
-Improved 1st pass success w/ paralytic 1st(PMID: 39425254)
-All about onset of action: Roc 1.2 mg/kg ~ 60 sec. Ketamine/etomidate ~ 30 sec + propofol ~15-20
-If push same time, induction agent will kick in first -> apnea w/o paralysis
#MedSky #EMIMCC
youtube.com/shorts/xjtIx...
-Improved 1st pass success w/ paralytic 1st(PMID: 39425254)
-All about onset of action: Roc 1.2 mg/kg ~ 60 sec. Ketamine/etomidate ~ 30 sec + propofol ~15-20
-If push same time, induction agent will kick in first -> apnea w/o paralysis
#MedSky #EMIMCC
youtube.com/shorts/xjtIx...

Resequencing RSI Meds #emergencymed #emergencymedicine #criticalcare #airway
YouTube video by EMSwami
youtube.com
December 23, 2024 at 4:55 PM
love this 😍
I've been promoting a roc-first strategy but I often get pushback implying that I'm an evil, inhumane ogre
but it works well & there's now data to support
if you disagree, pls direct all anger at @emswami.bsky.social
*ducks and runs*
(rationale: emcrit.org/pulmcrit/pul...) #EMIMCC
I've been promoting a roc-first strategy but I often get pushback implying that I'm an evil, inhumane ogre
but it works well & there's now data to support
if you disagree, pls direct all anger at @emswami.bsky.social
*ducks and runs*
(rationale: emcrit.org/pulmcrit/pul...) #EMIMCC
Reposted
a patient presents with DKA and this blood count
how can you tell that there's a serious infection going on here
(not just the usual DKA due to gastroenteritis, insulin pump malfunction, viral URI, etc.)?
🧵 1/5 #EMIMCC
how can you tell that there's a serious infection going on here
(not just the usual DKA due to gastroenteritis, insulin pump malfunction, viral URI, etc.)?
🧵 1/5 #EMIMCC

December 17, 2024 at 7:35 PM
a patient presents with DKA and this blood count
how can you tell that there's a serious infection going on here
(not just the usual DKA due to gastroenteritis, insulin pump malfunction, viral URI, etc.)?
🧵 1/5 #EMIMCC
how can you tell that there's a serious infection going on here
(not just the usual DKA due to gastroenteritis, insulin pump malfunction, viral URI, etc.)?
🧵 1/5 #EMIMCC