




Kaspar Bachmann
@kasparbachmann.bsky.social
MD | ICU Physician & Researcher
Passionate about gastrointestinal dysfunction, nutrition as well as ECMO and cardiopulmonary physiology. Enthusiast in #MatLab, signal analysis and data-driven research: https://pubmed.ncbi.nlm.nih.gov/?term=Kaspar+bachman
Passionate about gastrointestinal dysfunction, nutrition as well as ECMO and cardiopulmonary physiology. Enthusiast in #MatLab, signal analysis and data-driven research: https://pubmed.ncbi.nlm.nih.gov/?term=Kaspar+bachman
My question is, does it truly matter? If there’s a strong signal, shouldn’t I be able to detect it using either method (and vice versa)? And if the signal is borderline, shouldn’t I arrive at the same interpretation if my application and understanding of the statistics used are accurate?
August 15, 2025 at 11:10 AM
My question is, does it truly matter? If there’s a strong signal, shouldn’t I be able to detect it using either method (and vice versa)? And if the signal is borderline, shouldn’t I arrive at the same interpretation if my application and understanding of the statistics used are accurate?
Reposted by Kaspar Bachmann

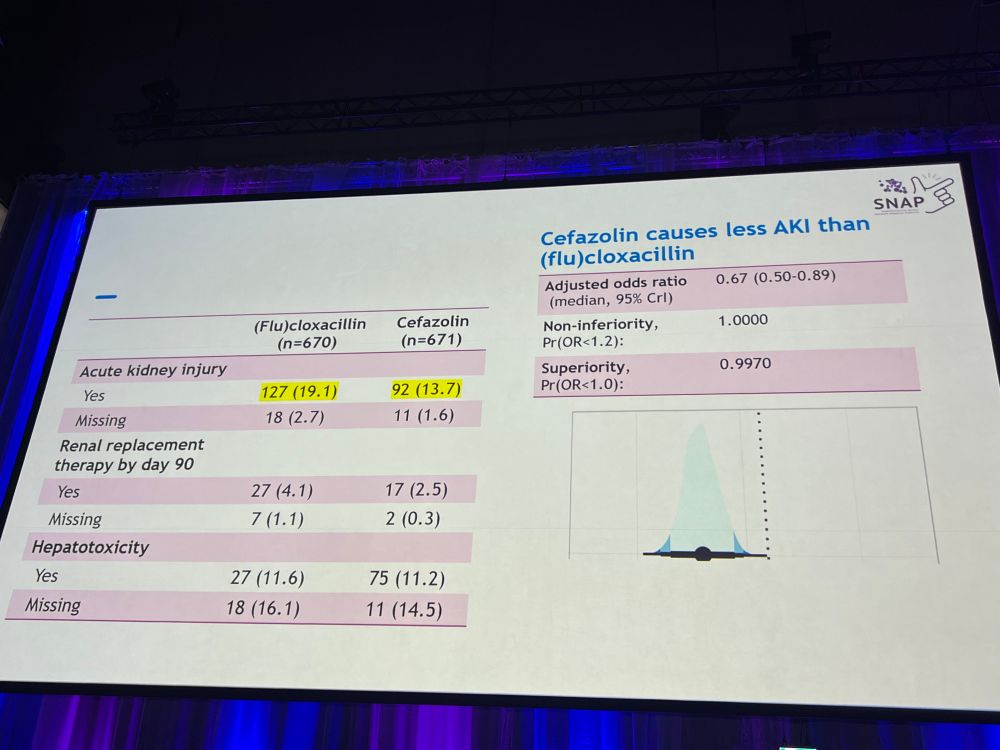
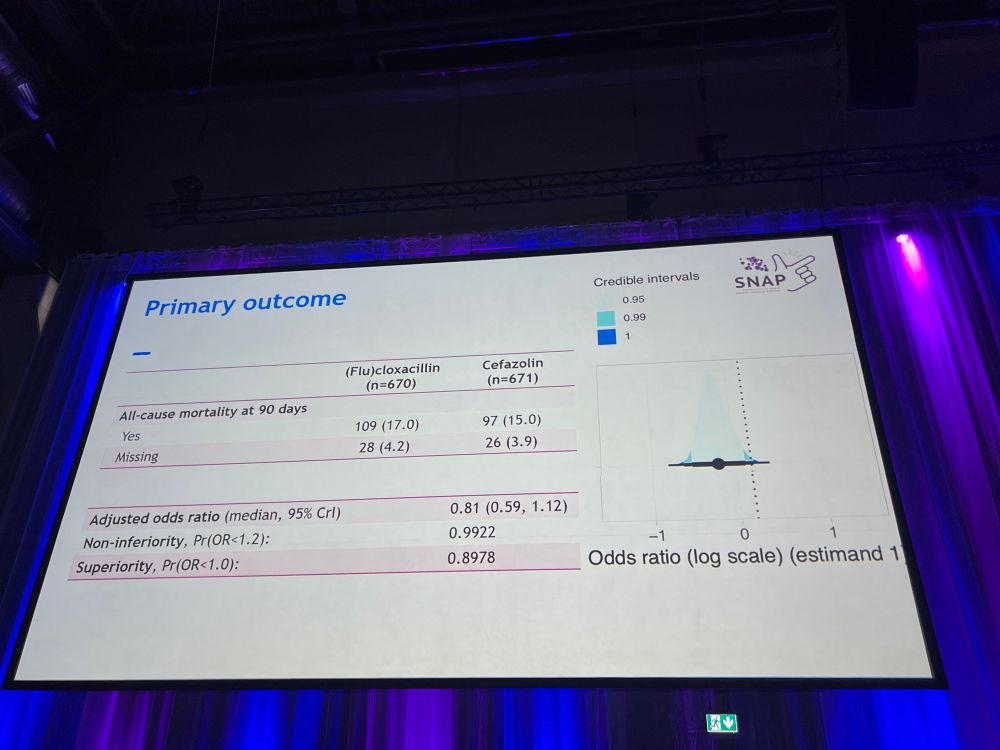
@gurujosh.bsky.social presents the results of the MSSA domain of the SNAP 🫰 trial at #ESCMID2025
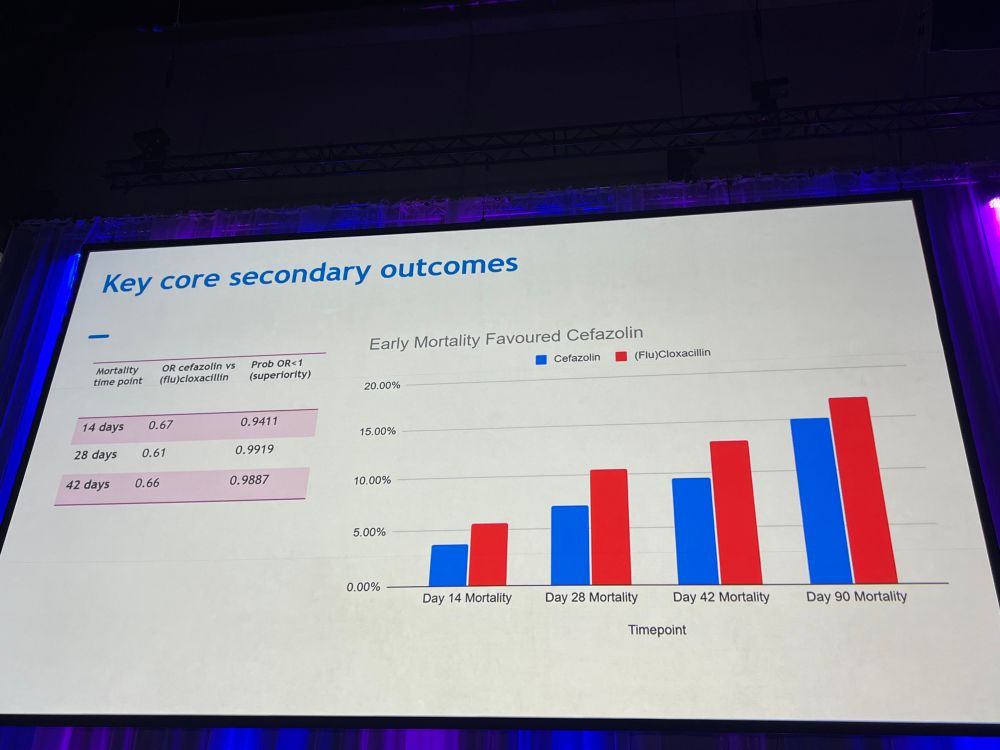
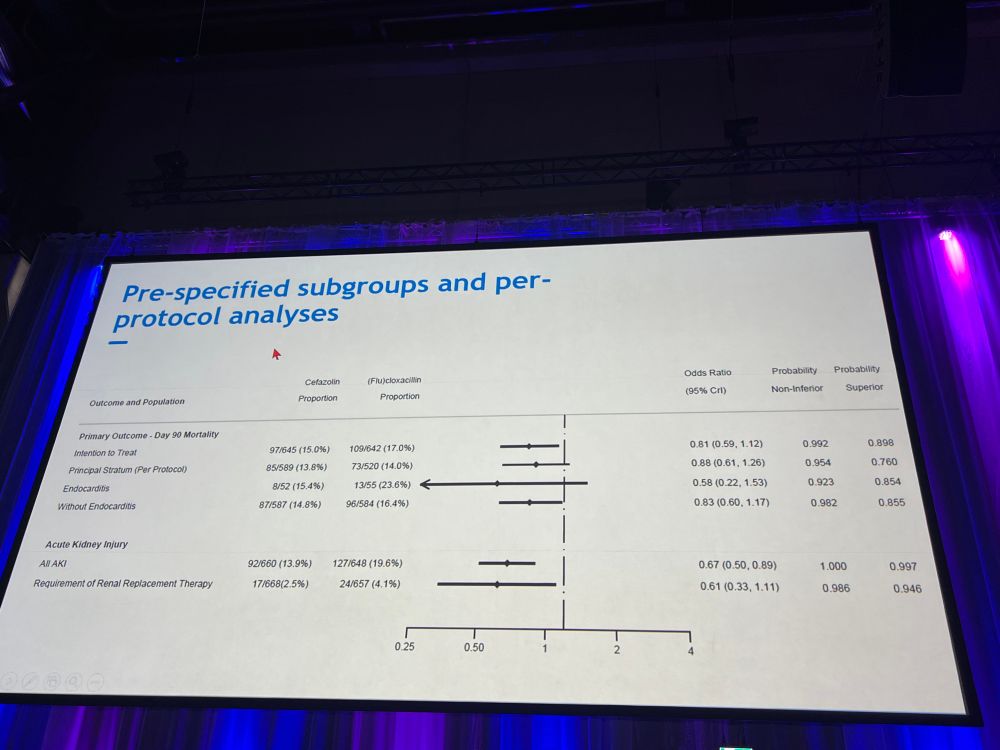
fluclox caused more acute kidney injury than cefazolin; early mortality favored cefazolin
Absolutely Herculean effort by the entire global trial team and practice changing data #teamcefazolin
fluclox caused more acute kidney injury than cefazolin; early mortality favored cefazolin
Absolutely Herculean effort by the entire global trial team and practice changing data #teamcefazolin
April 12, 2025 at 3:00 PM
@gurujosh.bsky.social presents the results of the MSSA domain of the SNAP 🫰 trial at #ESCMID2025
fluclox caused more acute kidney injury than cefazolin; early mortality favored cefazolin
Absolutely Herculean effort by the entire global trial team and practice changing data #teamcefazolin
fluclox caused more acute kidney injury than cefazolin; early mortality favored cefazolin
Absolutely Herculean effort by the entire global trial team and practice changing data #teamcefazolin
I don’t think that offering specific therapies out of the context of goals of care is helpful and may negatively impact the discussion and patient trajectory.
January 25, 2025 at 10:13 PM
I don’t think that offering specific therapies out of the context of goals of care is helpful and may negatively impact the discussion and patient trajectory.
I think we want to define where a patient wants to be in 1/3/6/12 months and with what level of quality of life. We as a team can then offer specific therapies (i.e. Trach/PEG but also other options such as mech. assist devices), if and only if these therapies align with the defined goals of care.
January 25, 2025 at 10:13 PM
I think we want to define where a patient wants to be in 1/3/6/12 months and with what level of quality of life. We as a team can then offer specific therapies (i.e. Trach/PEG but also other options such as mech. assist devices), if and only if these therapies align with the defined goals of care.
Recently listened to this:
soundphysicians.com/podcast-epis...
Has some good pearls and pitfalls and some resources in the shownotes.
soundphysicians.com/podcast-epis...
Has some good pearls and pitfalls and some resources in the shownotes.
soundphysicians.com
January 1, 2025 at 7:06 AM
Recently listened to this:
soundphysicians.com/podcast-epis...
Has some good pearls and pitfalls and some resources in the shownotes.
soundphysicians.com/podcast-epis...
Has some good pearls and pitfalls and some resources in the shownotes.
Do you/does anyone know if there are data repositories with patient data, timepoints and vanco levels as well as reference clearence (maybe from observational studies)?
We could then use that to 1) validate and 2) develop new models.
We could then use that to 1) validate and 2) develop new models.
December 19, 2024 at 8:28 AM
Do you/does anyone know if there are data repositories with patient data, timepoints and vanco levels as well as reference clearence (maybe from observational studies)?
We could then use that to 1) validate and 2) develop new models.
We could then use that to 1) validate and 2) develop new models.
#emimcc
I plan to do a thread on the paper/topic soon. This project has kept me busy over the last two years and it has been a pleasure working alongside an awesome steering committee and Delphi panel. 🙏
I plan to do a thread on the paper/topic soon. This project has kept me busy over the last two years and it has been a pleasure working alongside an awesome steering committee and Delphi panel. 🙏
December 18, 2024 at 4:58 PM
#emimcc
I plan to do a thread on the paper/topic soon. This project has kept me busy over the last two years and it has been a pleasure working alongside an awesome steering committee and Delphi panel. 🙏
I plan to do a thread on the paper/topic soon. This project has kept me busy over the last two years and it has been a pleasure working alongside an awesome steering committee and Delphi panel. 🙏
No, this was just a (very simple) approximation; imagine a trial that onlynlooked atbthis group and enrolled that number of patients. As the groups are exclusive, this was a first step to get a feeling of how much of a difference there really is…
December 12, 2024 at 12:58 PM
No, this was just a (very simple) approximation; imagine a trial that onlynlooked atbthis group and enrolled that number of patients. As the groups are exclusive, this was a first step to get a feeling of how much of a difference there really is…
The immunocompromised group was stopped for futility. I think that these groups are not powered enough to draw any conclusion and the difference is just statistical noise. Early intubation may be warranted in these patients who can deteriorate rapidly, also for early diagnosis via bronch/lavage.
December 12, 2024 at 10:01 AM
The immunocompromised group was stopped for futility. I think that these groups are not powered enough to draw any conclusion and the difference is just statistical noise. Early intubation may be warranted in these patients who can deteriorate rapidly, also for early diagnosis via bronch/lavage.
I agree, for cardiogenic NIPPV treats the not only the lungs but also the heart; this is why the results were suprising to me and I struggle with interpretation.
December 12, 2024 at 9:54 AM
I agree, for cardiogenic NIPPV treats the not only the lungs but also the heart; this is why the results were suprising to me and I struggle with interpretation.
CVP has the same function: it is the intersection of RV function curve and venous return, so it tells you how well the RV handles the VR and if there is RV dysfunction for that given state. It is no measure of volume status or responsiveness (but probably tolerance, as is VEXUS).
December 11, 2024 at 10:33 PM
CVP has the same function: it is the intersection of RV function curve and venous return, so it tells you how well the RV handles the VR and if there is RV dysfunction for that given state. It is no measure of volume status or responsiveness (but probably tolerance, as is VEXUS).