




Kaspar Bachmann
@kasparbachmann.bsky.social
MD | ICU Physician & Researcher
Passionate about gastrointestinal dysfunction, nutrition as well as ECMO and cardiopulmonary physiology. Enthusiast in #MatLab, signal analysis and data-driven research: https://pubmed.ncbi.nlm.nih.gov/?term=Kaspar+bachman
Passionate about gastrointestinal dysfunction, nutrition as well as ECMO and cardiopulmonary physiology. Enthusiast in #MatLab, signal analysis and data-driven research: https://pubmed.ncbi.nlm.nih.gov/?term=Kaspar+bachman

January 3, 2025 at 10:31 AM

December 6, 2024 at 3:21 PM
A PFO can act as a pressure valve in acute PE, but a PFO and DVT may also cause problems. I think depending on the thrombus load/anticoagulation strategy and specifics of the case, an IVCF merits a discussion.
Video Reference: www.jacc.org/doi/10.1016/...
Video Reference: www.jacc.org/doi/10.1016/...
December 3, 2024 at 12:38 PM
A PFO can act as a pressure valve in acute PE, but a PFO and DVT may also cause problems. I think depending on the thrombus load/anticoagulation strategy and specifics of the case, an IVCF merits a discussion.
Video Reference: www.jacc.org/doi/10.1016/...
Video Reference: www.jacc.org/doi/10.1016/...
To add to the discussion, Gattinoni and colleagues published similar arguments in 2015, worth a read in my opinion. ccforum.biomedcentral.com/articles/10....

December 1, 2024 at 6:53 AM
To add to the discussion, Gattinoni and colleagues published similar arguments in 2015, worth a read in my opinion. ccforum.biomedcentral.com/articles/10....
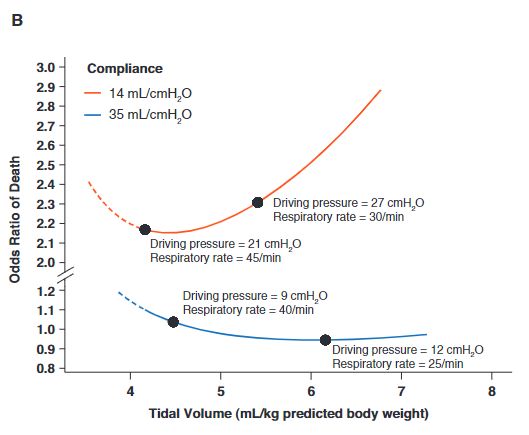
I agree, in a Vt range of 6-8 ml, the main component is dP. However, if you target low/very low dP (12-15) in a patient with poor compliance (very low tidal ventilation) and the increase in respiratory rate becomes relevant, I think. The figure is from the excellent paper you referenced (thanks).
November 29, 2024 at 12:52 PM
I agree, in a Vt range of 6-8 ml, the main component is dP. However, if you target low/very low dP (12-15) in a patient with poor compliance (very low tidal ventilation) and the increase in respiratory rate becomes relevant, I think. The figure is from the excellent paper you referenced (thanks).
The problem with decreasing driving pressure (or low Vt, which depending on the compliance is the same), is that RR has to go high to maintain gas exchange. This is especially pronounced in high deadspace states. Critical Care 2020, 24(Suppl 1):P090, (Page 35)

November 29, 2024 at 12:09 PM
The problem with decreasing driving pressure (or low Vt, which depending on the compliance is the same), is that RR has to go high to maintain gas exchange. This is especially pronounced in high deadspace states. Critical Care 2020, 24(Suppl 1):P090, (Page 35)
💯 the patient had severe mitral regurgitation. This lead to a postcapillary pulmonary hypertension with a high LVEDP. The prominent V-Wave in MR is sometimes challenging when introducing a PAC, as the signal stays „pulsatile“ and if not careful, can be misinterpreted.
rdcu.be/d05K0
rdcu.be/d05K0

November 22, 2024 at 6:33 AM
💯 the patient had severe mitral regurgitation. This lead to a postcapillary pulmonary hypertension with a high LVEDP. The prominent V-Wave in MR is sometimes challenging when introducing a PAC, as the signal stays „pulsatile“ and if not careful, can be misinterpreted.
rdcu.be/d05K0
rdcu.be/d05K0
November 20, 2024 at 4:06 PM
The common interpretation is that high stroke volume variation indicates fluid responsiveness. We show that SVV increases not only from preload dependency but also from RV afterload sensitivity. This explains why SVV often fails as a predictor of fluid responsiveness in RV dysfunction. 10/n

November 18, 2024 at 3:25 PM
The common interpretation is that high stroke volume variation indicates fluid responsiveness. We show that SVV increases not only from preload dependency but also from RV afterload sensitivity. This explains why SVV often fails as a predictor of fluid responsiveness in RV dysfunction. 10/n
The relationship between coupling and ejection fraction: EF = 1/(1 + 1/coupling).When coupling = 2: EF ≈ 67% When coupling = 1: EF ≈ 50%. RV-PA coupling (Ees/Ea ratio) maintains a value near 2. This results in a EF of 60-67%, indicating optimal energy transfer from RV to circulation 7/n

November 18, 2024 at 3:25 PM
The relationship between coupling and ejection fraction: EF = 1/(1 + 1/coupling).When coupling = 2: EF ≈ 67% When coupling = 1: EF ≈ 50%. RV-PA coupling (Ees/Ea ratio) maintains a value near 2. This results in a EF of 60-67%, indicating optimal energy transfer from RV to circulation 7/n
When ECMO flow decreases by 1L/min, blood flow increases by 0.5L/min. Pulmonary artery pressure rises by 1.8mmHg. During hypoxic pulmonary vasoconstriction, contractility (Ees) increased by 1.4 mmHg/mL. With pulmonary embolism, the RV enhanced its contractility by 0.4 mmHg/mL. 6/n

November 18, 2024 at 3:25 PM
When ECMO flow decreases by 1L/min, blood flow increases by 0.5L/min. Pulmonary artery pressure rises by 1.8mmHg. During hypoxic pulmonary vasoconstriction, contractility (Ees) increased by 1.4 mmHg/mL. With pulmonary embolism, the RV enhanced its contractility by 0.4 mmHg/mL. 6/n
The RV responds to increased afterload by enhancing contractility. Increases in #VenousReturn (i.e. preload) are met with dilation. This maintains the relationship between the RV and pulmonary elastance, i.e. mantains the RV-PA coupling. 4/n

November 18, 2024 at 3:25 PM
The RV responds to increased afterload by enhancing contractility. Increases in #VenousReturn (i.e. preload) are met with dilation. This maintains the relationship between the RV and pulmonary elastance, i.e. mantains the RV-PA coupling. 4/n
As ECMO flow decreases, blood returns to the right heart, increasing preload. We wanted to analyze RV function (single beat method): We fitted a sine wave to the pressure curve to estimate maximum isovlumentric pressure, which can be used to estimate Ees (Elastance/Contractility of the RV). 3/n

November 18, 2024 at 3:25 PM
As ECMO flow decreases, blood returns to the right heart, increasing preload. We wanted to analyze RV function (single beat method): We fitted a sine wave to the pressure curve to estimate maximum isovlumentric pressure, which can be used to estimate Ees (Elastance/Contractility of the RV). 3/n
Post a picture you took (no description) to bring some Zen into the timeline.

November 17, 2024 at 8:32 AM
Post a picture you took (no description) to bring some Zen into the timeline.

My old boss wrote an awesome publication on this: Low shunt (top left): SpO2 stays high despite poor cardiac output. High shunt (bottom right): SpO2 plummets unless cardiac output is very high. Figure reproduced from Takala, ICM 2007 using #MatLab
link.springer.com/article/10.1...
link.springer.com/article/10.1...

November 16, 2024 at 5:22 PM
My old boss wrote an awesome publication on this: Low shunt (top left): SpO2 stays high despite poor cardiac output. High shunt (bottom right): SpO2 plummets unless cardiac output is very high. Figure reproduced from Takala, ICM 2007 using #MatLab
link.springer.com/article/10.1...
link.springer.com/article/10.1...
The problem with the trial is that REBOA increased the time to definitive hemorrhage control (Table 2), so one might wonder if „speed“ were increased, there could still be a benefit.

November 15, 2024 at 11:55 AM
The problem with the trial is that REBOA increased the time to definitive hemorrhage control (Table 2), so one might wonder if „speed“ were increased, there could still be a benefit.