




Ravi Madan
@ravimadan.bsky.social
Clinical researcher focused on #ProstateCancer, early recurrence (#BCR/PSMA+ BCR) & #immunotherapy. Views are my own & do not represent the National Cancer Institute #Medsky
Lots of ❓s in defining benefits of “#oligomet” or “#MDT” therapy in #ProstateCancer
❓ADT+/-ARPI? How long?
❓PFS vs Eugonadal PFS?
❓how many mets? Where?
🔑❓what imaging 🩻❓
#PSMA mets🚫🟰CT/Bone scan mets
shorturl.at/n3JwU
Std of Care? Or just something we can do?
❓ADT+/-ARPI? How long?
❓PFS vs Eugonadal PFS?
❓how many mets? Where?
🔑❓what imaging 🩻❓
#PSMA mets🚫🟰CT/Bone scan mets
shorturl.at/n3JwU
Std of Care? Or just something we can do?
November 11, 2025 at 12:55 PM
Lots of ❓s in defining benefits of “#oligomet” or “#MDT” therapy in #ProstateCancer
❓ADT+/-ARPI? How long?
❓PFS vs Eugonadal PFS?
❓how many mets? Where?
🔑❓what imaging 🩻❓
#PSMA mets🚫🟰CT/Bone scan mets
shorturl.at/n3JwU
Std of Care? Or just something we can do?
❓ADT+/-ARPI? How long?
❓PFS vs Eugonadal PFS?
❓how many mets? Where?
🔑❓what imaging 🩻❓
#PSMA mets🚫🟰CT/Bone scan mets
shorturl.at/n3JwU
Std of Care? Or just something we can do?
We don’t need to fear the Dark in #ProstateCancer
But we will have to acknowledge that #PSMA targeted therapy will likely impact the sensitivity of #PSMA imaging
This likely impacts the desire to use PSMA in restating (still unclear how to do that) & drug development #PSMAdark
But we will have to acknowledge that #PSMA targeted therapy will likely impact the sensitivity of #PSMA imaging
This likely impacts the desire to use PSMA in restating (still unclear how to do that) & drug development #PSMAdark
As #ESMO25 brings new data on #PSMA it may be time to consider what happens when you target a surface antigen in cancer. How will that impact diagnostic sensitivity of that target?
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe


November 5, 2025 at 3:29 PM
We don’t need to fear the Dark in #ProstateCancer
But we will have to acknowledge that #PSMA targeted therapy will likely impact the sensitivity of #PSMA imaging
This likely impacts the desire to use PSMA in restating (still unclear how to do that) & drug development #PSMAdark
But we will have to acknowledge that #PSMA targeted therapy will likely impact the sensitivity of #PSMA imaging
This likely impacts the desire to use PSMA in restating (still unclear how to do that) & drug development #PSMAdark
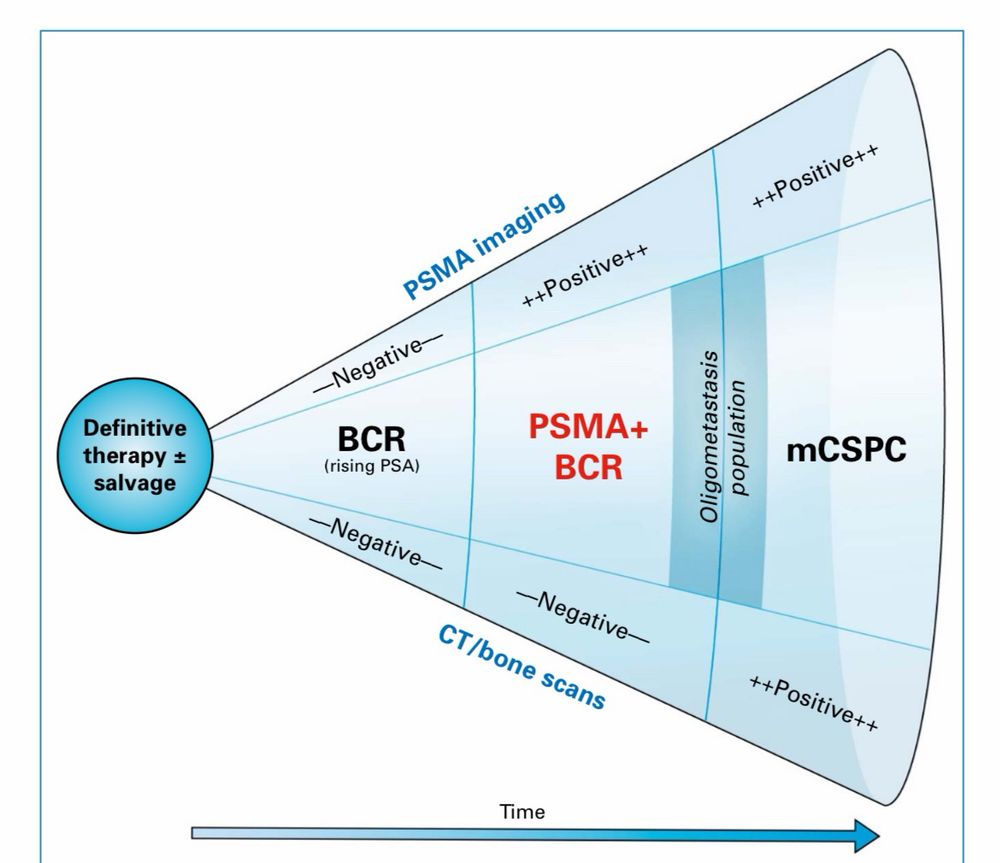
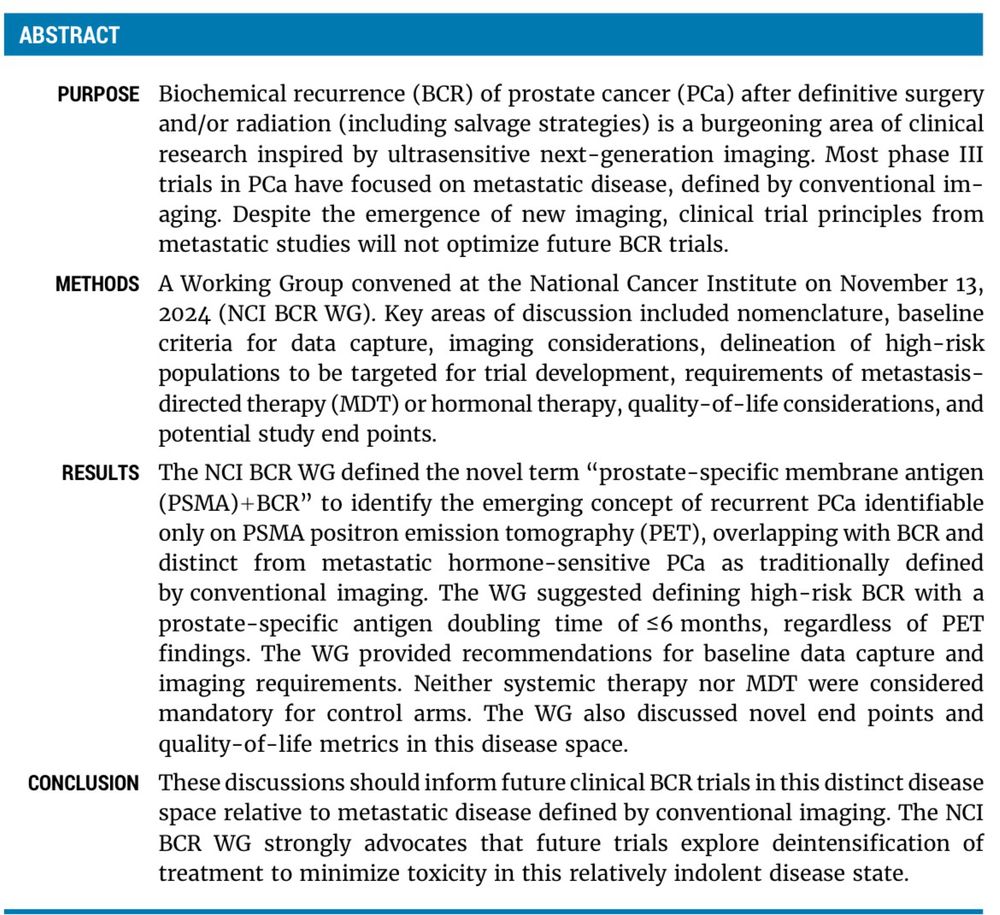
#PSMA+BCR
That is how @theNCI #BCR Working Group unanimously agreed to define pts w/PSMA findings & neg CT/bone scan after definitive tx
Retains all that is known about #BCR while drawing a distinction vs. mCSPC
More than semantics for #ProstateCancer pts & clinicians
@ascocancer.bsky.social
That is how @theNCI #BCR Working Group unanimously agreed to define pts w/PSMA findings & neg CT/bone scan after definitive tx
Retains all that is known about #BCR while drawing a distinction vs. mCSPC
More than semantics for #ProstateCancer pts & clinicians
@ascocancer.bsky.social


October 28, 2025 at 3:05 PM
#PSMA+BCR
That is how @theNCI #BCR Working Group unanimously agreed to define pts w/PSMA findings & neg CT/bone scan after definitive tx
Retains all that is known about #BCR while drawing a distinction vs. mCSPC
More than semantics for #ProstateCancer pts & clinicians
@ascocancer.bsky.social
That is how @theNCI #BCR Working Group unanimously agreed to define pts w/PSMA findings & neg CT/bone scan after definitive tx
Retains all that is known about #BCR while drawing a distinction vs. mCSPC
More than semantics for #ProstateCancer pts & clinicians
@ascocancer.bsky.social
#EMBARK #BCR📈 #ProstateCancer I have a forrest plot ?
2 subgroups w/LACK of clear benefit are⬆️CV risk(competing mortality-logical)
But why would pts under⬇️65 not🚫 have clear benefit?
This is a subgp where competing mortality shouldn’t be an issue & Tx should help ⁉️🧐
2 subgroups w/LACK of clear benefit are⬆️CV risk(competing mortality-logical)
But why would pts under⬇️65 not🚫 have clear benefit?
This is a subgp where competing mortality shouldn’t be an issue & Tx should help ⁉️🧐

October 23, 2025 at 12:27 PM
#EMBARK #BCR📈 #ProstateCancer I have a forrest plot ?
2 subgroups w/LACK of clear benefit are⬆️CV risk(competing mortality-logical)
But why would pts under⬇️65 not🚫 have clear benefit?
This is a subgp where competing mortality shouldn’t be an issue & Tx should help ⁉️🧐
2 subgroups w/LACK of clear benefit are⬆️CV risk(competing mortality-logical)
But why would pts under⬇️65 not🚫 have clear benefit?
This is a subgp where competing mortality shouldn’t be an issue & Tx should help ⁉️🧐
Reposted by Ravi Madan
As #ESMO25 brings new data on #PSMA it may be time to consider what happens when you target a surface antigen in cancer. How will that impact diagnostic sensitivity of that target?
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
October 14, 2025 at 2:11 PM
As #ESMO25 brings new data on #PSMA it may be time to consider what happens when you target a surface antigen in cancer. How will that impact diagnostic sensitivity of that target?
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
#EMBARK #ESMO25 creates the need to risk stratify pts
Here is data published last year which demonstrates that #ProstateCancer specific death is rare among unselected #BCR pts.
EMBARK Tx is for high risk pts (eg PSA DT<6mos)
tinyurl.com/y69hb5ue
Here is data published last year which demonstrates that #ProstateCancer specific death is rare among unselected #BCR pts.
EMBARK Tx is for high risk pts (eg PSA DT<6mos)
tinyurl.com/y69hb5ue

October 19, 2025 at 1:29 PM
#EMBARK #ESMO25 creates the need to risk stratify pts
Here is data published last year which demonstrates that #ProstateCancer specific death is rare among unselected #BCR pts.
EMBARK Tx is for high risk pts (eg PSA DT<6mos)
tinyurl.com/y69hb5ue
Here is data published last year which demonstrates that #ProstateCancer specific death is rare among unselected #BCR pts.
EMBARK Tx is for high risk pts (eg PSA DT<6mos)
tinyurl.com/y69hb5ue
Lots @ #ESMO25 re: #BCR #ProstateCancer but over-treatment of this indolent disease remains an important issue
How does #PSMA imaging factor in? See poster #2393P presented by @HelenMoonMD Saturday
+PSMA findings in BCR pts shouldn’t be the reason to treat as rPD is rare @1yr
How does #PSMA imaging factor in? See poster #2393P presented by @HelenMoonMD Saturday
+PSMA findings in BCR pts shouldn’t be the reason to treat as rPD is rare @1yr



October 18, 2025 at 9:43 AM
Lots @ #ESMO25 re: #BCR #ProstateCancer but over-treatment of this indolent disease remains an important issue
How does #PSMA imaging factor in? See poster #2393P presented by @HelenMoonMD Saturday
+PSMA findings in BCR pts shouldn’t be the reason to treat as rPD is rare @1yr
How does #PSMA imaging factor in? See poster #2393P presented by @HelenMoonMD Saturday
+PSMA findings in BCR pts shouldn’t be the reason to treat as rPD is rare @1yr
As #ESMO25 brings new data on #PSMA it may be time to consider what happens when you target a surface antigen in cancer. How will that impact diagnostic sensitivity of that target?
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
October 14, 2025 at 2:11 PM
As #ESMO25 brings new data on #PSMA it may be time to consider what happens when you target a surface antigen in cancer. How will that impact diagnostic sensitivity of that target?
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
From The NCI #PSMA files
73 yo male PSA=17 PSADT=11.6mos
PSMA=5+ nodes in pelvis RP & torso
(All~5mm). Neg CT and bone scan
No🚫Treatment
1 yr later
PSA=40 PSADT=13.1 mos
PSMA stable across 2 scans over 12 mos
#PSMA+ #BCR #ProstateCancer is an indolent process-OK to monitor these pts
73 yo male PSA=17 PSADT=11.6mos
PSMA=5+ nodes in pelvis RP & torso
(All~5mm). Neg CT and bone scan
No🚫Treatment
1 yr later
PSA=40 PSADT=13.1 mos
PSMA stable across 2 scans over 12 mos
#PSMA+ #BCR #ProstateCancer is an indolent process-OK to monitor these pts

homer simpson is holding a hammer next to a sign that says caution
ALT: homer simpson is holding a hammer next to a sign that says caution
media.tenor.com
September 26, 2025 at 2:58 PM
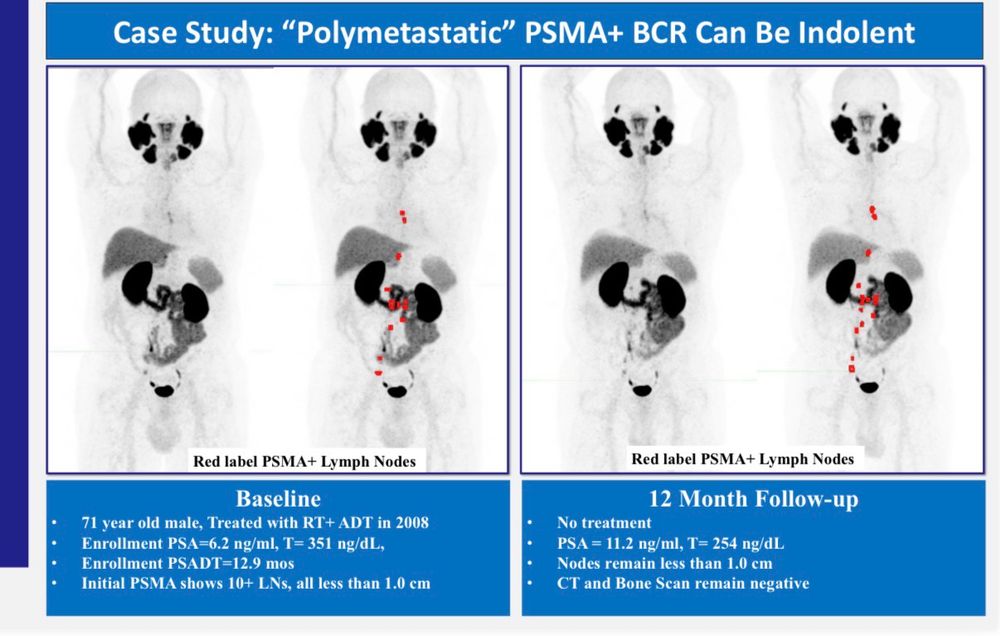
From The NCI #PSMA files
73 yo male PSA=17 PSADT=11.6mos
PSMA=5+ nodes in pelvis RP & torso
(All~5mm). Neg CT and bone scan
No🚫Treatment
1 yr later
PSA=40 PSADT=13.1 mos
PSMA stable across 2 scans over 12 mos
#PSMA+ #BCR #ProstateCancer is an indolent process-OK to monitor these pts
73 yo male PSA=17 PSADT=11.6mos
PSMA=5+ nodes in pelvis RP & torso
(All~5mm). Neg CT and bone scan
No🚫Treatment
1 yr later
PSA=40 PSADT=13.1 mos
PSMA stable across 2 scans over 12 mos
#PSMA+ #BCR #ProstateCancer is an indolent process-OK to monitor these pts
Important to distinguish #serosal findings on #PSMA 🩻vs. #parenchymal
Serosal lesions are better seen on #PSMA vs CT/MRI in #ProstateCancer but likely have an indolent course even with no 🚫therapy (even on the liver!)
Dr. Melissa Abel at el @natrevurol.nature.com
rdcu.be/eBwPs
Serosal lesions are better seen on #PSMA vs CT/MRI in #ProstateCancer but likely have an indolent course even with no 🚫therapy (even on the liver!)
Dr. Melissa Abel at el @natrevurol.nature.com
rdcu.be/eBwPs

Ominous-appearing serosal findings on PSMA imaging might belie indolent clinical course
Nature Reviews Urology - Understanding of metastatic prostate cancer is mainly defined by macroscopic findings, but prostate-specific membrane antigen (PSMA) PET has increased sensitivity. PSMA+...
rdcu.be
August 21, 2025 at 12:02 PM
Important to distinguish #serosal findings on #PSMA 🩻vs. #parenchymal
Serosal lesions are better seen on #PSMA vs CT/MRI in #ProstateCancer but likely have an indolent course even with no 🚫therapy (even on the liver!)
Dr. Melissa Abel at el @natrevurol.nature.com
rdcu.be/eBwPs
Serosal lesions are better seen on #PSMA vs CT/MRI in #ProstateCancer but likely have an indolent course even with no 🚫therapy (even on the liver!)
Dr. Melissa Abel at el @natrevurol.nature.com
rdcu.be/eBwPs
Restaging w/ #PSMA Imaging in #mCRPC #ProstateCancer: When Seeing More Is Detrimental to Care
Sadly a year later this remains true & the frequency of this is 📈
@ascocancer.bsky.social @ascopost.bsky.social
ascopubs.org/doi/pdf/10.1...
Sadly a year later this remains true & the frequency of this is 📈
@ascocancer.bsky.social @ascopost.bsky.social
ascopubs.org/doi/pdf/10.1...
August 4, 2025 at 8:05 PM
Restaging w/ #PSMA Imaging in #mCRPC #ProstateCancer: When Seeing More Is Detrimental to Care
Sadly a year later this remains true & the frequency of this is 📈
@ascocancer.bsky.social @ascopost.bsky.social
ascopubs.org/doi/pdf/10.1...
Sadly a year later this remains true & the frequency of this is 📈
@ascocancer.bsky.social @ascopost.bsky.social
ascopubs.org/doi/pdf/10.1...
Reposted by Ravi Madan

We have known for more than 20 years that chemotherapy has clinically significant efficacy in metastatic #ProstateCancer #pcsm, including improved overall survival. It has not stopped working just because new agents are available or are being tested.
July 26, 2025 at 11:49 PM
We have known for more than 20 years that chemotherapy has clinically significant efficacy in metastatic #ProstateCancer #pcsm, including improved overall survival. It has not stopped working just because new agents are available or are being tested.
Reposted by Ravi Madan
Two opinions that to my surprise are either unpopular or not widely held:
1. The control arm of a randomised trial should be best standard of care.
2. A PFS benefit against an inactive comparator is not a major advance, if progressive disease is required for eligibility.
1. The control arm of a randomised trial should be best standard of care.
2. A PFS benefit against an inactive comparator is not a major advance, if progressive disease is required for eligibility.
July 26, 2025 at 10:40 PM
Two opinions that to my surprise are either unpopular or not widely held:
1. The control arm of a randomised trial should be best standard of care.
2. A PFS benefit against an inactive comparator is not a major advance, if progressive disease is required for eligibility.
1. The control arm of a randomised trial should be best standard of care.
2. A PFS benefit against an inactive comparator is not a major advance, if progressive disease is required for eligibility.
Reposted by Ravi Madan

Pleasure to highlight your work with #UroToday @ravimadan.bsky.social - as we all consider how best to treat PSMA avid disease.
Do #PSMA+ findings in #BCR #ProstateCancer require immediate treatment?
NO based on emerging data @theNCI
Appreciate @tiansterzhangmd.bsky.social & #Urotoday for the opportunity to discuss
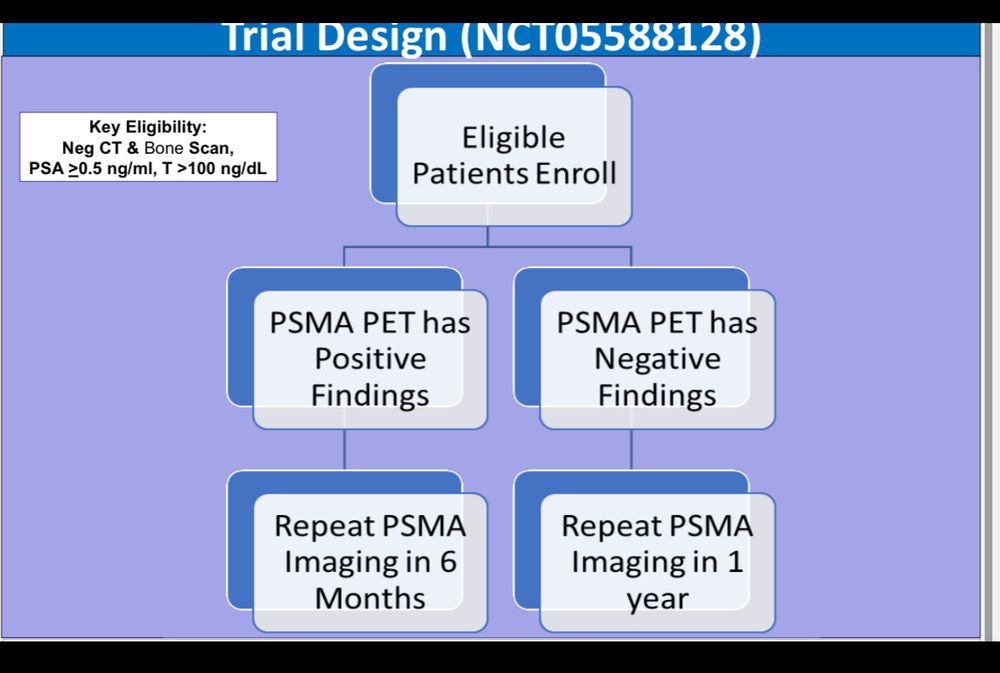
Ongoing trial of PSMA scans in BCR is still enrolling shorturl.at/36nGQ
www.urotoday.com/categories-m...
NO based on emerging data @theNCI
Appreciate @tiansterzhangmd.bsky.social & #Urotoday for the opportunity to discuss
Ongoing trial of PSMA scans in BCR is still enrolling shorturl.at/36nGQ
www.urotoday.com/categories-m...

PSMA PET in Biochemical Recurrence: When to Treat vs When to Wait - Ravi Madan
Tian Zhang interviews Ravi Madan about a prospective study monitoring PSMA PET-positive biochemically recurrent prostate cancer patients. The trial enrolls patients with PSA > 0.5 and negative convent...
www.urotoday.com
July 19, 2025 at 11:17 PM
Pleasure to highlight your work with #UroToday @ravimadan.bsky.social - as we all consider how best to treat PSMA avid disease.
Do #PSMA+ findings in #BCR #ProstateCancer require immediate treatment?
NO based on emerging data @theNCI
Appreciate @tiansterzhangmd.bsky.social & #Urotoday for the opportunity to discuss
Ongoing trial of PSMA scans in BCR is still enrolling shorturl.at/36nGQ
www.urotoday.com/categories-m...
NO based on emerging data @theNCI
Appreciate @tiansterzhangmd.bsky.social & #Urotoday for the opportunity to discuss
Ongoing trial of PSMA scans in BCR is still enrolling shorturl.at/36nGQ
www.urotoday.com/categories-m...
PSMA PET in Biochemical Recurrence: When to Treat vs When to Wait - Ravi Madan
Tian Zhang interviews Ravi Madan about a prospective study monitoring PSMA PET-positive biochemically recurrent prostate cancer patients. The trial enrolls patients with PSA > 0.5 and negative convent...
www.urotoday.com
July 18, 2025 at 1:14 PM
Do #PSMA+ findings in #BCR #ProstateCancer require immediate treatment?
NO based on emerging data @theNCI
Appreciate @tiansterzhangmd.bsky.social & #Urotoday for the opportunity to discuss
Ongoing trial of PSMA scans in BCR is still enrolling shorturl.at/36nGQ
www.urotoday.com/categories-m...
NO based on emerging data @theNCI
Appreciate @tiansterzhangmd.bsky.social & #Urotoday for the opportunity to discuss
Ongoing trial of PSMA scans in BCR is still enrolling shorturl.at/36nGQ
www.urotoday.com/categories-m...
Great discussions #ProstateCancer posters #ASCO25 @ascocancer.bsky.social
#PSMA+ #BCR is indolent & pts do NOT require urgent therapy in most cases
We should be ⚠️ cautious about over-treatment
🔗shorturl.at/NtxdF
Trial continues to accrue @theNCI
www.clinicaltrials.gov/study/NCT055...
#PSMA+ #BCR is indolent & pts do NOT require urgent therapy in most cases
We should be ⚠️ cautious about over-treatment
🔗shorturl.at/NtxdF
Trial continues to accrue @theNCI
www.clinicaltrials.gov/study/NCT055...



June 4, 2025 at 9:13 AM
Great discussions #ProstateCancer posters #ASCO25 @ascocancer.bsky.social
#PSMA+ #BCR is indolent & pts do NOT require urgent therapy in most cases
We should be ⚠️ cautious about over-treatment
🔗shorturl.at/NtxdF
Trial continues to accrue @theNCI
www.clinicaltrials.gov/study/NCT055...
#PSMA+ #BCR is indolent & pts do NOT require urgent therapy in most cases
We should be ⚠️ cautious about over-treatment
🔗shorturl.at/NtxdF
Trial continues to accrue @theNCI
www.clinicaltrials.gov/study/NCT055...
Most expected #Arches 5 yr follow up data to be pro-forma #ASCO25
@ascocancer.bsky.social
But then this data popped up 👀
Less clear benefit of Enza+ADT in low volume #mCSPC
Should this raise ?s for #mCSPC intensification w/#parp & #LU-psma
Implications for over treating PSMA+ recurrence?
@ascocancer.bsky.social
But then this data popped up 👀
Less clear benefit of Enza+ADT in low volume #mCSPC
Should this raise ?s for #mCSPC intensification w/#parp & #LU-psma
Implications for over treating PSMA+ recurrence?

June 4, 2025 at 2:59 AM
It remains disappointing that (unlike the Lu-PSMA trials) the #PARP inhibitor trials do not include cross over and thus continue to leave the key question of sequence unanswered. This limits understanding of clinical optimization
#AMPLITUDE #ASCO25 @ascocancer.bsky.social
#AMPLITUDE #ASCO25 @ascocancer.bsky.social

June 4, 2025 at 2:57 AM
It remains disappointing that (unlike the Lu-PSMA trials) the #PARP inhibitor trials do not include cross over and thus continue to leave the key question of sequence unanswered. This limits understanding of clinical optimization
#AMPLITUDE #ASCO25 @ascocancer.bsky.social
#AMPLITUDE #ASCO25 @ascocancer.bsky.social
How to discern important new data @ ASCO?
Look beyond data that repackages known truths but do NOT really advance our understanding
Common examples:
1. Less cancer is better than more cancer
2. Responders do better
3. More treatments vs. less improve PFS
Happy #ASCO25
@ascocancer.bsky.social
Look beyond data that repackages known truths but do NOT really advance our understanding
Common examples:
1. Less cancer is better than more cancer
2. Responders do better
3. More treatments vs. less improve PFS
Happy #ASCO25
@ascocancer.bsky.social
May 29, 2025 at 1:21 PM
How to discern important new data @ ASCO?
Look beyond data that repackages known truths but do NOT really advance our understanding
Common examples:
1. Less cancer is better than more cancer
2. Responders do better
3. More treatments vs. less improve PFS
Happy #ASCO25
@ascocancer.bsky.social
Look beyond data that repackages known truths but do NOT really advance our understanding
Common examples:
1. Less cancer is better than more cancer
2. Responders do better
3. More treatments vs. less improve PFS
Happy #ASCO25
@ascocancer.bsky.social
Around this time of year we see the “How should #oncology #fellows navigate the ASCO mtg?” advice.
My take:
👉🏽Very Carefully 🤓
Distinguish science from showmanship and make sure the substance of a presentation aligns with the “take home message”
Happy ASCO ☺️
@ascocancer.bsky.social
#ASCO25
My take:
👉🏽Very Carefully 🤓
Distinguish science from showmanship and make sure the substance of a presentation aligns with the “take home message”
Happy ASCO ☺️
@ascocancer.bsky.social
#ASCO25

May 29, 2025 at 3:17 AM
Around this time of year we see the “How should #oncology #fellows navigate the ASCO mtg?” advice.
My take:
👉🏽Very Carefully 🤓
Distinguish science from showmanship and make sure the substance of a presentation aligns with the “take home message”
Happy ASCO ☺️
@ascocancer.bsky.social
#ASCO25
My take:
👉🏽Very Carefully 🤓
Distinguish science from showmanship and make sure the substance of a presentation aligns with the “take home message”
Happy ASCO ☺️
@ascocancer.bsky.social
#ASCO25
Rorschach Test for #ProstateCancer in 2025
Treat w/your favorite approach +/- your 2nd favorite approach?
Or acknowledge lack of data supporting long term benefits in this case & defer tx?
@theNCI continues to enroll #BCR pts on #PSMA monitoring trial
www.clinicaltrials.gov/study/NCT055...
Treat w/your favorite approach +/- your 2nd favorite approach?
Or acknowledge lack of data supporting long term benefits in this case & defer tx?
@theNCI continues to enroll #BCR pts on #PSMA monitoring trial
www.clinicaltrials.gov/study/NCT055...

May 22, 2025 at 2:20 PM
Rorschach Test for #ProstateCancer in 2025
Treat w/your favorite approach +/- your 2nd favorite approach?
Or acknowledge lack of data supporting long term benefits in this case & defer tx?
@theNCI continues to enroll #BCR pts on #PSMA monitoring trial
www.clinicaltrials.gov/study/NCT055...
Treat w/your favorite approach +/- your 2nd favorite approach?
Or acknowledge lack of data supporting long term benefits in this case & defer tx?
@theNCI continues to enroll #BCR pts on #PSMA monitoring trial
www.clinicaltrials.gov/study/NCT055...
Case from the #NCI #PSMA files
67 yo w/#BCR #ProstateCancer
4 yrs s/p RP (declined salvage)
PSA=1.0
PSA DT=11 mos(“high risk”per European criteria)
PSMA shows only 6 mm obturator node next to ureter (SUVmax=26)
—no treatment
18 months later PSA is 1.1
LN=8mm
No new findings on PSMA
67 yo w/#BCR #ProstateCancer
4 yrs s/p RP (declined salvage)
PSA=1.0
PSA DT=11 mos(“high risk”per European criteria)
PSMA shows only 6 mm obturator node next to ureter (SUVmax=26)
—no treatment
18 months later PSA is 1.1
LN=8mm
No new findings on PSMA
May 15, 2025 at 1:13 PM
Case from the #NCI #PSMA files
67 yo w/#BCR #ProstateCancer
4 yrs s/p RP (declined salvage)
PSA=1.0
PSA DT=11 mos(“high risk”per European criteria)
PSMA shows only 6 mm obturator node next to ureter (SUVmax=26)
—no treatment
18 months later PSA is 1.1
LN=8mm
No new findings on PSMA
67 yo w/#BCR #ProstateCancer
4 yrs s/p RP (declined salvage)
PSA=1.0
PSA DT=11 mos(“high risk”per European criteria)
PSMA shows only 6 mm obturator node next to ureter (SUVmax=26)
—no treatment
18 months later PSA is 1.1
LN=8mm
No new findings on PSMA
Reposted by Ravi Madan

Do these clinical trial failures demonstrate a failure of traditional pre-clinical models to reflect the human disease?
In addition to the complete avoidance of biomarker-driven clinical trials to find the subset of patients that would benefit.? @asharpmedonc.bsky.social @pcf-science.bsky.social
In addition to the complete avoidance of biomarker-driven clinical trials to find the subset of patients that would benefit.? @asharpmedonc.bsky.social @pcf-science.bsky.social
Dr. Susan Slovin from MSK asks some key questions regarding #ProstateCancer #Immunotherapy
@ascocancer.bsky.social
ascopubs.org/doi/10.1200/...
@ascocancer.bsky.social
ascopubs.org/doi/10.1200/...
Immune Checkpoint Combos in Metastatic Castration-Resistant Prostate Cancer: Where Are We Going, What Are We Doing, and Why?
ascopubs.org
March 17, 2025 at 1:48 PM
Do these clinical trial failures demonstrate a failure of traditional pre-clinical models to reflect the human disease?
In addition to the complete avoidance of biomarker-driven clinical trials to find the subset of patients that would benefit.? @asharpmedonc.bsky.social @pcf-science.bsky.social
In addition to the complete avoidance of biomarker-driven clinical trials to find the subset of patients that would benefit.? @asharpmedonc.bsky.social @pcf-science.bsky.social
Dr. Susan Slovin from MSK asks some key questions regarding #ProstateCancer #Immunotherapy
@ascocancer.bsky.social
ascopubs.org/doi/10.1200/...
@ascocancer.bsky.social
ascopubs.org/doi/10.1200/...
Immune Checkpoint Combos in Metastatic Castration-Resistant Prostate Cancer: Where Are We Going, What Are We Doing, and Why?
ascopubs.org
March 17, 2025 at 1:21 PM
Dr. Susan Slovin from MSK asks some key questions regarding #ProstateCancer #Immunotherapy
@ascocancer.bsky.social
ascopubs.org/doi/10.1200/...
@ascocancer.bsky.social
ascopubs.org/doi/10.1200/...