




Ravi Madan
@ravimadan.bsky.social
Clinical researcher focused on #ProstateCancer, early recurrence (#BCR/PSMA+ BCR) & #immunotherapy. Views are my own & do not represent the National Cancer Institute #Medsky
👏🏼Interesting study #SBRT+/-#LuPSMA @ascocancer.bsky.social
⭐️Innovative design w/limited dosing of LuPSMA #oligorecurrent #ProstateCancer
❓What if all pts were MTD-Naive
🤔important differences in 🔑baseline characteristics favor combo
🤔PFS criteria w/❓clinical value
ascopubs.org/doi/pdf/10.1...
⭐️Innovative design w/limited dosing of LuPSMA #oligorecurrent #ProstateCancer
❓What if all pts were MTD-Naive
🤔important differences in 🔑baseline characteristics favor combo
🤔PFS criteria w/❓clinical value
ascopubs.org/doi/pdf/10.1...



November 14, 2025 at 1:53 AM
👏🏼Interesting study #SBRT+/-#LuPSMA @ascocancer.bsky.social
⭐️Innovative design w/limited dosing of LuPSMA #oligorecurrent #ProstateCancer
❓What if all pts were MTD-Naive
🤔important differences in 🔑baseline characteristics favor combo
🤔PFS criteria w/❓clinical value
ascopubs.org/doi/pdf/10.1...
⭐️Innovative design w/limited dosing of LuPSMA #oligorecurrent #ProstateCancer
❓What if all pts were MTD-Naive
🤔important differences in 🔑baseline characteristics favor combo
🤔PFS criteria w/❓clinical value
ascopubs.org/doi/pdf/10.1...
Clinical and #Genomic Differences Between Advanced Molecular Imaging-detected and Conventional Imaging-detected Metachronous Oligometastatic Castration-sensitive #ProstateCancer @EUplatinum
#PSMA
www.sciencedirect.com/science/arti...
#PSMA
www.sciencedirect.com/science/arti...
November 11, 2025 at 12:56 PM
Clinical and #Genomic Differences Between Advanced Molecular Imaging-detected and Conventional Imaging-detected Metachronous Oligometastatic Castration-sensitive #ProstateCancer @EUplatinum
#PSMA
www.sciencedirect.com/science/arti...
#PSMA
www.sciencedirect.com/science/arti...
Lots of ❓s in defining benefits of “#oligomet” or “#MDT” therapy in #ProstateCancer
❓ADT+/-ARPI? How long?
❓PFS vs Eugonadal PFS?
❓how many mets? Where?
🔑❓what imaging 🩻❓
#PSMA mets🚫🟰CT/Bone scan mets
shorturl.at/n3JwU
Std of Care? Or just something we can do?
❓ADT+/-ARPI? How long?
❓PFS vs Eugonadal PFS?
❓how many mets? Where?
🔑❓what imaging 🩻❓
#PSMA mets🚫🟰CT/Bone scan mets
shorturl.at/n3JwU
Std of Care? Or just something we can do?
November 11, 2025 at 12:55 PM
Lots of ❓s in defining benefits of “#oligomet” or “#MDT” therapy in #ProstateCancer
❓ADT+/-ARPI? How long?
❓PFS vs Eugonadal PFS?
❓how many mets? Where?
🔑❓what imaging 🩻❓
#PSMA mets🚫🟰CT/Bone scan mets
shorturl.at/n3JwU
Std of Care? Or just something we can do?
❓ADT+/-ARPI? How long?
❓PFS vs Eugonadal PFS?
❓how many mets? Where?
🔑❓what imaging 🩻❓
#PSMA mets🚫🟰CT/Bone scan mets
shorturl.at/n3JwU
Std of Care? Or just something we can do?
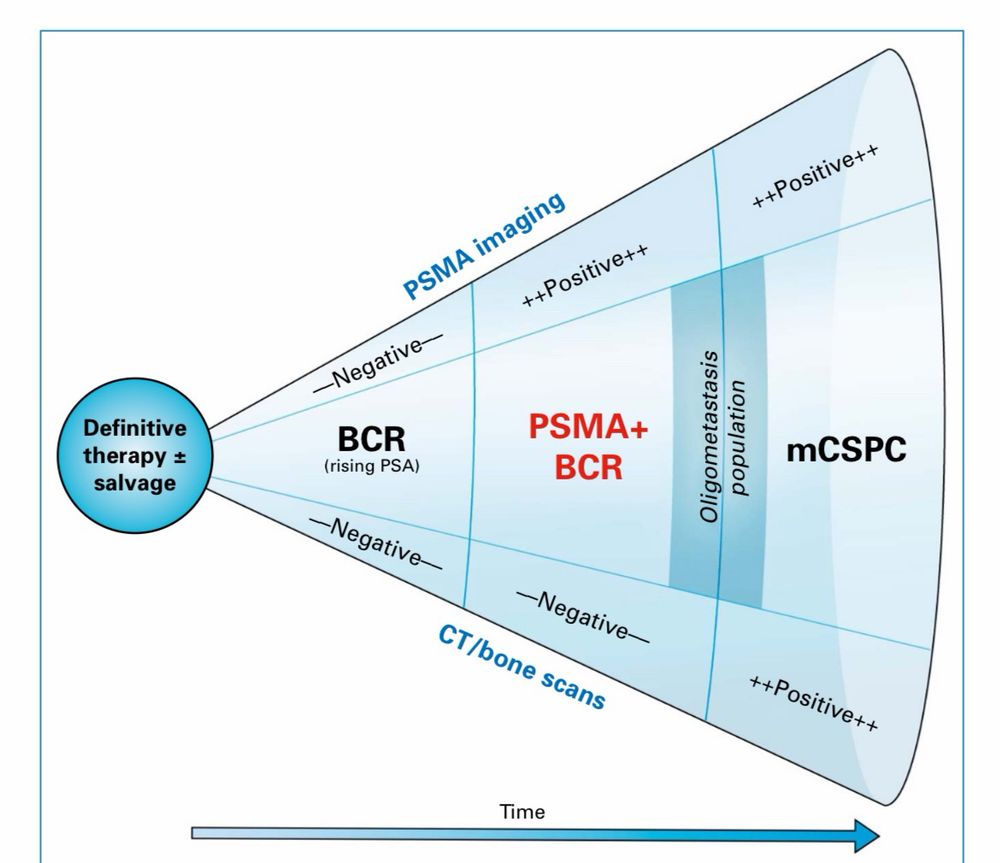
#PSMA+BCR
That is how @theNCI #BCR Working Group unanimously agreed to define pts w/PSMA findings & neg CT/bone scan after definitive tx
Retains all that is known about #BCR while drawing a distinction vs. mCSPC
More than semantics for #ProstateCancer pts & clinicians
@ascocancer.bsky.social
That is how @theNCI #BCR Working Group unanimously agreed to define pts w/PSMA findings & neg CT/bone scan after definitive tx
Retains all that is known about #BCR while drawing a distinction vs. mCSPC
More than semantics for #ProstateCancer pts & clinicians
@ascocancer.bsky.social


October 28, 2025 at 3:05 PM
#PSMA+BCR
That is how @theNCI #BCR Working Group unanimously agreed to define pts w/PSMA findings & neg CT/bone scan after definitive tx
Retains all that is known about #BCR while drawing a distinction vs. mCSPC
More than semantics for #ProstateCancer pts & clinicians
@ascocancer.bsky.social
That is how @theNCI #BCR Working Group unanimously agreed to define pts w/PSMA findings & neg CT/bone scan after definitive tx
Retains all that is known about #BCR while drawing a distinction vs. mCSPC
More than semantics for #ProstateCancer pts & clinicians
@ascocancer.bsky.social
#EMBARK #BCR📈 #ProstateCancer I have a forrest plot ?
2 subgroups w/LACK of clear benefit are⬆️CV risk(competing mortality-logical)
But why would pts under⬇️65 not🚫 have clear benefit?
This is a subgp where competing mortality shouldn’t be an issue & Tx should help ⁉️🧐
2 subgroups w/LACK of clear benefit are⬆️CV risk(competing mortality-logical)
But why would pts under⬇️65 not🚫 have clear benefit?
This is a subgp where competing mortality shouldn’t be an issue & Tx should help ⁉️🧐

October 23, 2025 at 12:27 PM
#EMBARK #BCR📈 #ProstateCancer I have a forrest plot ?
2 subgroups w/LACK of clear benefit are⬆️CV risk(competing mortality-logical)
But why would pts under⬇️65 not🚫 have clear benefit?
This is a subgp where competing mortality shouldn’t be an issue & Tx should help ⁉️🧐
2 subgroups w/LACK of clear benefit are⬆️CV risk(competing mortality-logical)
But why would pts under⬇️65 not🚫 have clear benefit?
This is a subgp where competing mortality shouldn’t be an issue & Tx should help ⁉️🧐
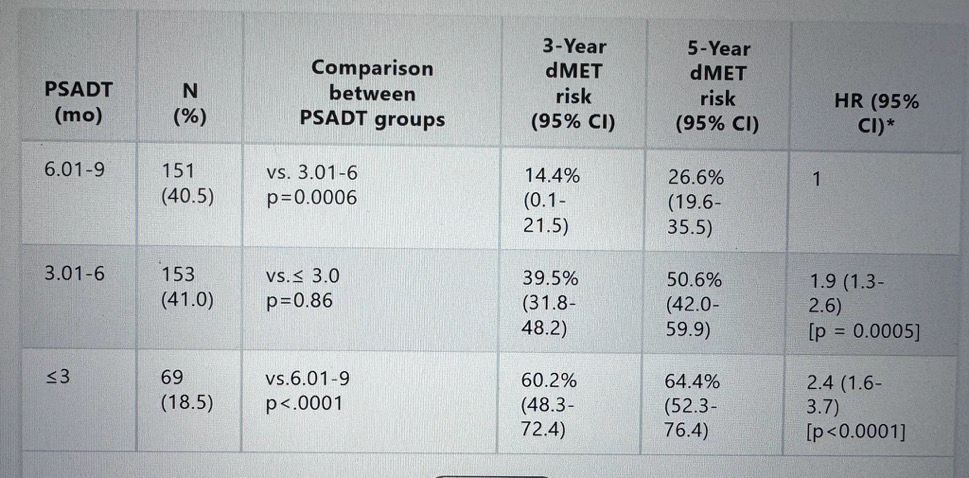
#EMBARK #ESMO25 creates the need to risk stratify pts
Here is data published last year which demonstrates that #ProstateCancer specific death is rare among unselected #BCR pts.
EMBARK Tx is for high risk pts (eg PSA DT<6mos)
tinyurl.com/y69hb5ue
Here is data published last year which demonstrates that #ProstateCancer specific death is rare among unselected #BCR pts.
EMBARK Tx is for high risk pts (eg PSA DT<6mos)
tinyurl.com/y69hb5ue

October 19, 2025 at 1:29 PM
#EMBARK #ESMO25 creates the need to risk stratify pts
Here is data published last year which demonstrates that #ProstateCancer specific death is rare among unselected #BCR pts.
EMBARK Tx is for high risk pts (eg PSA DT<6mos)
tinyurl.com/y69hb5ue
Here is data published last year which demonstrates that #ProstateCancer specific death is rare among unselected #BCR pts.
EMBARK Tx is for high risk pts (eg PSA DT<6mos)
tinyurl.com/y69hb5ue
Lots @ #ESMO25 re: #BCR #ProstateCancer but over-treatment of this indolent disease remains an important issue
How does #PSMA imaging factor in? See poster #2393P presented by @HelenMoonMD Saturday
+PSMA findings in BCR pts shouldn’t be the reason to treat as rPD is rare @1yr
How does #PSMA imaging factor in? See poster #2393P presented by @HelenMoonMD Saturday
+PSMA findings in BCR pts shouldn’t be the reason to treat as rPD is rare @1yr



October 18, 2025 at 9:43 AM
Lots @ #ESMO25 re: #BCR #ProstateCancer but over-treatment of this indolent disease remains an important issue
How does #PSMA imaging factor in? See poster #2393P presented by @HelenMoonMD Saturday
+PSMA findings in BCR pts shouldn’t be the reason to treat as rPD is rare @1yr
How does #PSMA imaging factor in? See poster #2393P presented by @HelenMoonMD Saturday
+PSMA findings in BCR pts shouldn’t be the reason to treat as rPD is rare @1yr
As #ESMO25 brings new data on #PSMA it may be time to consider what happens when you target a surface antigen in cancer. How will that impact diagnostic sensitivity of that target?
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe


October 14, 2025 at 2:11 PM
As #ESMO25 brings new data on #PSMA it may be time to consider what happens when you target a surface antigen in cancer. How will that impact diagnostic sensitivity of that target?
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
#PSMAdark
#ProstateCancer #theranostics
Dr Abel et al
@natrevurol.nature.com @ascocancer.bsky.social
rdcu.be/eKNQe
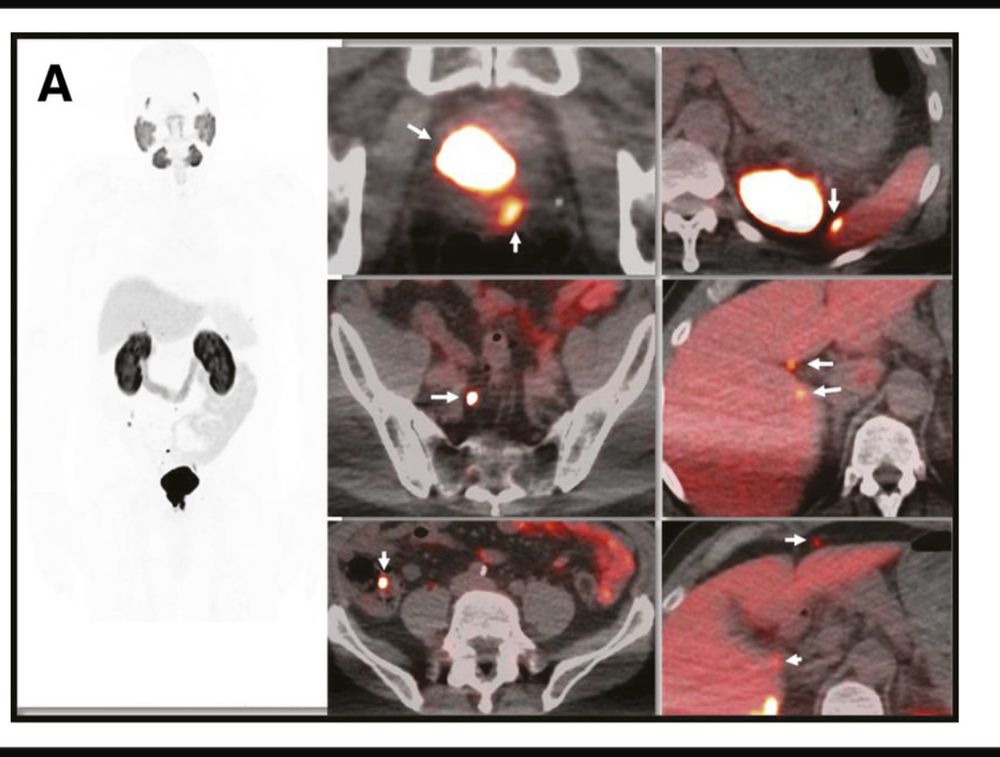
Not the first example of indolent serosal findings on #PSMA in #ProstateCancer
This pt with findings in 2018
tinyurl.com/29tpcddy
@ascocancer.bsky.social
This patient with serosal findings on the liver remains without parenchymal Mets in 2025. Went most of the 7 years without treatment.
This pt with findings in 2018
tinyurl.com/29tpcddy
@ascocancer.bsky.social
This patient with serosal findings on the liver remains without parenchymal Mets in 2025. Went most of the 7 years without treatment.
August 21, 2025 at 12:27 PM
Not the first example of indolent serosal findings on #PSMA in #ProstateCancer
This pt with findings in 2018
tinyurl.com/29tpcddy
@ascocancer.bsky.social
This patient with serosal findings on the liver remains without parenchymal Mets in 2025. Went most of the 7 years without treatment.
This pt with findings in 2018
tinyurl.com/29tpcddy
@ascocancer.bsky.social
This patient with serosal findings on the liver remains without parenchymal Mets in 2025. Went most of the 7 years without treatment.
Restaging w/ #PSMA Imaging in #mCRPC #ProstateCancer: When Seeing More Is Detrimental to Care
Sadly a year later this remains true & the frequency of this is 📈
@ascocancer.bsky.social @ascopost.bsky.social
ascopubs.org/doi/pdf/10.1...
Sadly a year later this remains true & the frequency of this is 📈
@ascocancer.bsky.social @ascopost.bsky.social
ascopubs.org/doi/pdf/10.1...
August 4, 2025 at 8:05 PM
Restaging w/ #PSMA Imaging in #mCRPC #ProstateCancer: When Seeing More Is Detrimental to Care
Sadly a year later this remains true & the frequency of this is 📈
@ascocancer.bsky.social @ascopost.bsky.social
ascopubs.org/doi/pdf/10.1...
Sadly a year later this remains true & the frequency of this is 📈
@ascocancer.bsky.social @ascopost.bsky.social
ascopubs.org/doi/pdf/10.1...
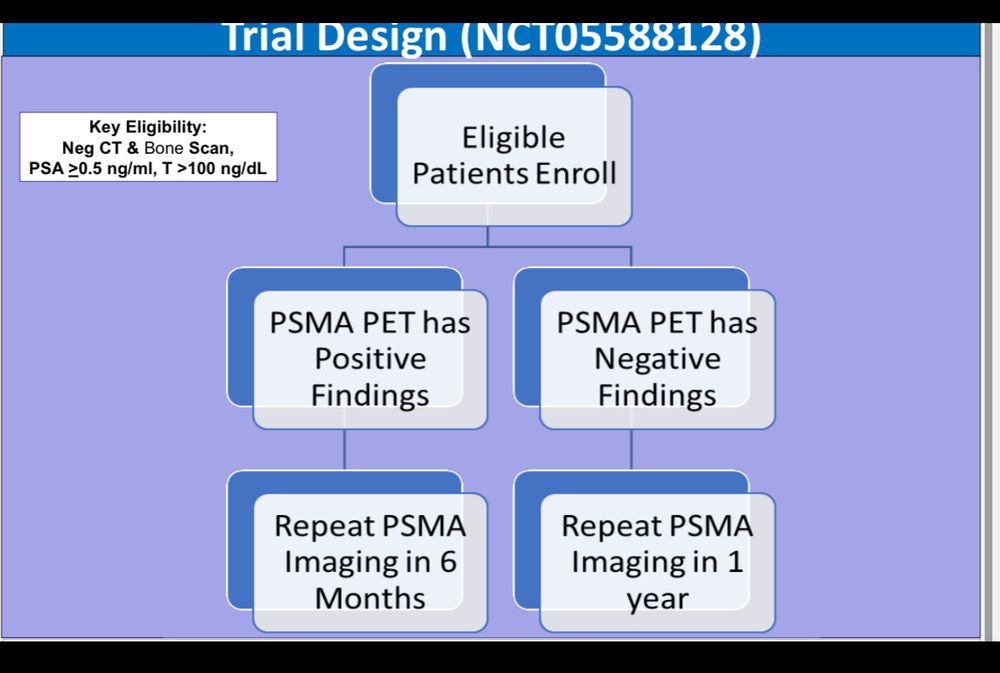
Great discussions #ProstateCancer posters #ASCO25 @ascocancer.bsky.social
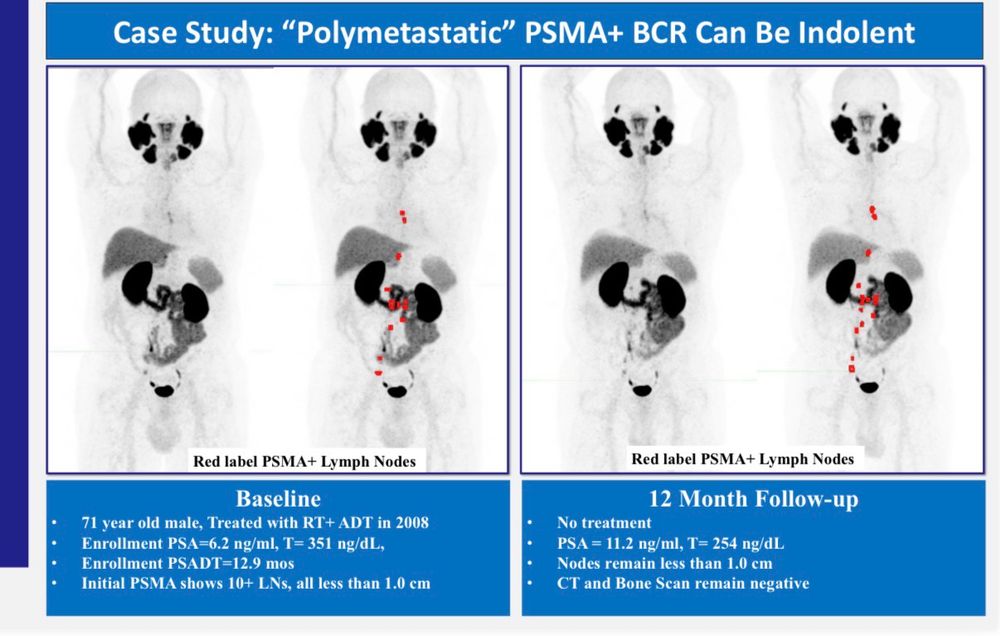
#PSMA+ #BCR is indolent & pts do NOT require urgent therapy in most cases
We should be ⚠️ cautious about over-treatment
🔗shorturl.at/NtxdF
Trial continues to accrue @theNCI
www.clinicaltrials.gov/study/NCT055...
#PSMA+ #BCR is indolent & pts do NOT require urgent therapy in most cases
We should be ⚠️ cautious about over-treatment
🔗shorturl.at/NtxdF
Trial continues to accrue @theNCI
www.clinicaltrials.gov/study/NCT055...



June 4, 2025 at 9:13 AM
Great discussions #ProstateCancer posters #ASCO25 @ascocancer.bsky.social
#PSMA+ #BCR is indolent & pts do NOT require urgent therapy in most cases
We should be ⚠️ cautious about over-treatment
🔗shorturl.at/NtxdF
Trial continues to accrue @theNCI
www.clinicaltrials.gov/study/NCT055...
#PSMA+ #BCR is indolent & pts do NOT require urgent therapy in most cases
We should be ⚠️ cautious about over-treatment
🔗shorturl.at/NtxdF
Trial continues to accrue @theNCI
www.clinicaltrials.gov/study/NCT055...
Most expected #Arches 5 yr follow up data to be pro-forma #ASCO25
@ascocancer.bsky.social
But then this data popped up 👀
Less clear benefit of Enza+ADT in low volume #mCSPC
Should this raise ?s for #mCSPC intensification w/#parp & #LU-psma
Implications for over treating PSMA+ recurrence?
@ascocancer.bsky.social
But then this data popped up 👀
Less clear benefit of Enza+ADT in low volume #mCSPC
Should this raise ?s for #mCSPC intensification w/#parp & #LU-psma
Implications for over treating PSMA+ recurrence?

June 4, 2025 at 2:59 AM
It remains disappointing that (unlike the Lu-PSMA trials) the #PARP inhibitor trials do not include cross over and thus continue to leave the key question of sequence unanswered. This limits understanding of clinical optimization
#AMPLITUDE #ASCO25 @ascocancer.bsky.social
#AMPLITUDE #ASCO25 @ascocancer.bsky.social

June 4, 2025 at 2:57 AM
It remains disappointing that (unlike the Lu-PSMA trials) the #PARP inhibitor trials do not include cross over and thus continue to leave the key question of sequence unanswered. This limits understanding of clinical optimization
#AMPLITUDE #ASCO25 @ascocancer.bsky.social
#AMPLITUDE #ASCO25 @ascocancer.bsky.social
Around this time of year we see the “How should #oncology #fellows navigate the ASCO mtg?” advice.
My take:
👉🏽Very Carefully 🤓
Distinguish science from showmanship and make sure the substance of a presentation aligns with the “take home message”
Happy ASCO ☺️
@ascocancer.bsky.social
#ASCO25
My take:
👉🏽Very Carefully 🤓
Distinguish science from showmanship and make sure the substance of a presentation aligns with the “take home message”
Happy ASCO ☺️
@ascocancer.bsky.social
#ASCO25

May 29, 2025 at 3:17 AM
Around this time of year we see the “How should #oncology #fellows navigate the ASCO mtg?” advice.
My take:
👉🏽Very Carefully 🤓
Distinguish science from showmanship and make sure the substance of a presentation aligns with the “take home message”
Happy ASCO ☺️
@ascocancer.bsky.social
#ASCO25
My take:
👉🏽Very Carefully 🤓
Distinguish science from showmanship and make sure the substance of a presentation aligns with the “take home message”
Happy ASCO ☺️
@ascocancer.bsky.social
#ASCO25
Rorschach Test for #ProstateCancer in 2025
Treat w/your favorite approach +/- your 2nd favorite approach?
Or acknowledge lack of data supporting long term benefits in this case & defer tx?
@theNCI continues to enroll #BCR pts on #PSMA monitoring trial
www.clinicaltrials.gov/study/NCT055...
Treat w/your favorite approach +/- your 2nd favorite approach?
Or acknowledge lack of data supporting long term benefits in this case & defer tx?
@theNCI continues to enroll #BCR pts on #PSMA monitoring trial
www.clinicaltrials.gov/study/NCT055...

May 22, 2025 at 2:20 PM
Rorschach Test for #ProstateCancer in 2025
Treat w/your favorite approach +/- your 2nd favorite approach?
Or acknowledge lack of data supporting long term benefits in this case & defer tx?
@theNCI continues to enroll #BCR pts on #PSMA monitoring trial
www.clinicaltrials.gov/study/NCT055...
Treat w/your favorite approach +/- your 2nd favorite approach?
Or acknowledge lack of data supporting long term benefits in this case & defer tx?
@theNCI continues to enroll #BCR pts on #PSMA monitoring trial
www.clinicaltrials.gov/study/NCT055...
Case from the #NCI #PSMA files
67 yo w/#BCR #ProstateCancer
4 yrs s/p RP (declined salvage)
PSA=1.0
PSA DT=11 mos(“high risk”per European criteria)
PSMA shows only 6 mm obturator node next to ureter (SUVmax=26)
—no treatment
18 months later PSA is 1.1
LN=8mm
No new findings on PSMA
67 yo w/#BCR #ProstateCancer
4 yrs s/p RP (declined salvage)
PSA=1.0
PSA DT=11 mos(“high risk”per European criteria)
PSMA shows only 6 mm obturator node next to ureter (SUVmax=26)
—no treatment
18 months later PSA is 1.1
LN=8mm
No new findings on PSMA
May 15, 2025 at 1:13 PM
Case from the #NCI #PSMA files
67 yo w/#BCR #ProstateCancer
4 yrs s/p RP (declined salvage)
PSA=1.0
PSA DT=11 mos(“high risk”per European criteria)
PSMA shows only 6 mm obturator node next to ureter (SUVmax=26)
—no treatment
18 months later PSA is 1.1
LN=8mm
No new findings on PSMA
67 yo w/#BCR #ProstateCancer
4 yrs s/p RP (declined salvage)
PSA=1.0
PSA DT=11 mos(“high risk”per European criteria)
PSMA shows only 6 mm obturator node next to ureter (SUVmax=26)
—no treatment
18 months later PSA is 1.1
LN=8mm
No new findings on PSMA
Certainly a worthy topic of discussion in #ProstateCancer #Trials and beyond.
Complex discussion with many considerations, but one whose time has come and should include disease experts, industry and regulatory.
@oncologynews.bsky.social
bit.ly/4kaza5K
Complex discussion with many considerations, but one whose time has come and should include disease experts, industry and regulatory.
@oncologynews.bsky.social
bit.ly/4kaza5K
February 21, 2025 at 2:16 AM
Certainly a worthy topic of discussion in #ProstateCancer #Trials and beyond.
Complex discussion with many considerations, but one whose time has come and should include disease experts, industry and regulatory.
@oncologynews.bsky.social
bit.ly/4kaza5K
Complex discussion with many considerations, but one whose time has come and should include disease experts, industry and regulatory.
@oncologynews.bsky.social
bit.ly/4kaza5K
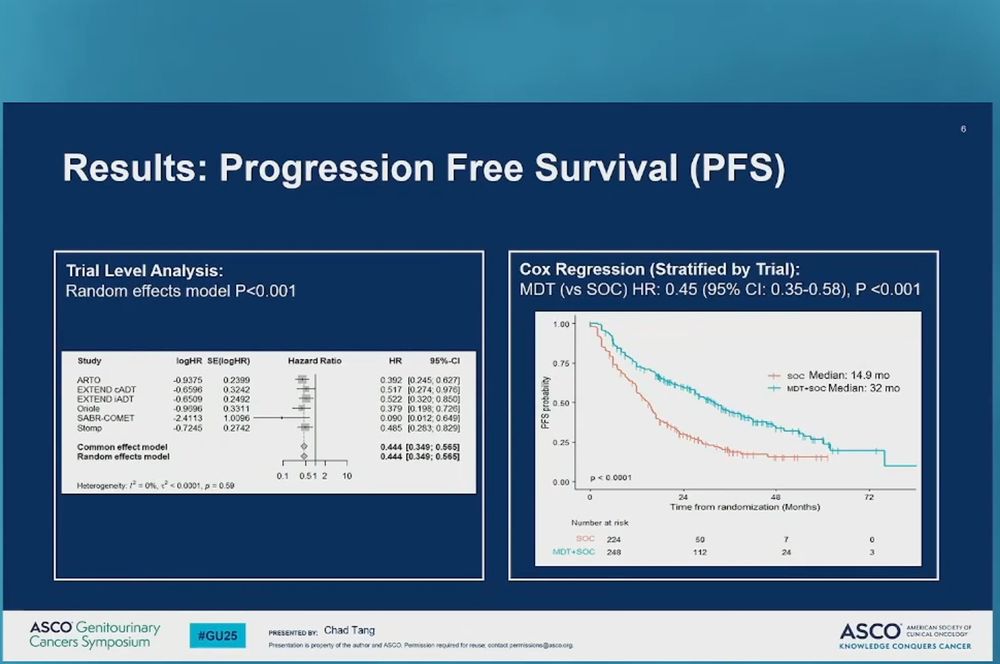
Good to see #wolverine & trend to OS in #MDT in #ProstateCancer @ascocancer.bsky.social #GU25
Many key❓remain
✴️ who gets benefit (we can tx all but do we need to?)
✴️ ADT or not?
✴️ ARPI or not?
✴️ need to distinguish between oligomet vs #PSMA+ #BCR - 2 very different populations & biologies
Many key❓remain
✴️ who gets benefit (we can tx all but do we need to?)
✴️ ADT or not?
✴️ ARPI or not?
✴️ need to distinguish between oligomet vs #PSMA+ #BCR - 2 very different populations & biologies


February 14, 2025 at 2:48 PM
Good to see #wolverine & trend to OS in #MDT in #ProstateCancer @ascocancer.bsky.social #GU25
Many key❓remain
✴️ who gets benefit (we can tx all but do we need to?)
✴️ ADT or not?
✴️ ARPI or not?
✴️ need to distinguish between oligomet vs #PSMA+ #BCR - 2 very different populations & biologies
Many key❓remain
✴️ who gets benefit (we can tx all but do we need to?)
✴️ ADT or not?
✴️ ARPI or not?
✴️ need to distinguish between oligomet vs #PSMA+ #BCR - 2 very different populations & biologies
Abs#45 #GU25 @ascocancer.bsky.social
Prelim data shows near term metastatic progression (conventional imaging) is rare in #PSMA+ #BCR #ProstateCancer
Are we overtreating pts w/median age of 70+ based on lack of understanding of #PSMA?
This study continues
meetings.asco.org/abstracts-pr...
Prelim data shows near term metastatic progression (conventional imaging) is rare in #PSMA+ #BCR #ProstateCancer
Are we overtreating pts w/median age of 70+ based on lack of understanding of #PSMA?
This study continues
meetings.asco.org/abstracts-pr...


February 13, 2025 at 10:49 PM
Abs#45 #GU25 @ascocancer.bsky.social
Prelim data shows near term metastatic progression (conventional imaging) is rare in #PSMA+ #BCR #ProstateCancer
Are we overtreating pts w/median age of 70+ based on lack of understanding of #PSMA?
This study continues
meetings.asco.org/abstracts-pr...
Prelim data shows near term metastatic progression (conventional imaging) is rare in #PSMA+ #BCR #ProstateCancer
Are we overtreating pts w/median age of 70+ based on lack of understanding of #PSMA?
This study continues
meetings.asco.org/abstracts-pr...
Watching #BCR session @asco #GU25 it is very clear there is a drive to treat #BCR asap esp w/+ #PSMA
But there is no data supporting a curative strategy & in that context deferring therapy max’ing #QOL is quite reasonable given JHU MFS data below
ascopubs.org/doi/10.1200/...
But there is no data supporting a curative strategy & in that context deferring therapy max’ing #QOL is quite reasonable given JHU MFS data below
ascopubs.org/doi/10.1200/...
February 13, 2025 at 10:46 PM
Appreciate Dr. Alicia Morgans acknowledging the fundamental disconnect we often observe between toxicity we observe in clinic and pt reported outcomes in #ProstateCancer
Also glad to hear her discuss options moving forward.
#GU25 @ascocancer.bsky.social
Also glad to hear her discuss options moving forward.
#GU25 @ascocancer.bsky.social


February 13, 2025 at 9:49 PM
Appreciate Dr. Alicia Morgans acknowledging the fundamental disconnect we often observe between toxicity we observe in clinic and pt reported outcomes in #ProstateCancer
Also glad to hear her discuss options moving forward.
#GU25 @ascocancer.bsky.social
Also glad to hear her discuss options moving forward.
#GU25 @ascocancer.bsky.social
Intriguing CT DNA presented by Dr. Johann DeBono suggesting the value in assessing treatment response #PSMAfore #Lu-psma #mCRPC #ProstateCancer
Especially appreciate comparison to PSA50 responses given it’s already in clinic
It does make me wonder - what if we looked at PSA80? #GU25
Especially appreciate comparison to PSA50 responses given it’s already in clinic
It does make me wonder - what if we looked at PSA80? #GU25



February 13, 2025 at 7:49 PM
Intriguing CT DNA presented by Dr. Johann DeBono suggesting the value in assessing treatment response #PSMAfore #Lu-psma #mCRPC #ProstateCancer
Especially appreciate comparison to PSA50 responses given it’s already in clinic
It does make me wonder - what if we looked at PSA80? #GU25
Especially appreciate comparison to PSA50 responses given it’s already in clinic
It does make me wonder - what if we looked at PSA80? #GU25
Dr. Louise Emmett presents OS data from #Enzalutamide +/- #Lu-psma in 1st line mCRPC #ProstateCancer
Intriguing data to be sure but would have appreciated a built in cross-over given equivalent OS seen in #PSMAfore in 2nd line mCRPC when ARPI before or after Lu-psma #GU25 @ascocancer.bsky.social
Intriguing data to be sure but would have appreciated a built in cross-over given equivalent OS seen in #PSMAfore in 2nd line mCRPC when ARPI before or after Lu-psma #GU25 @ascocancer.bsky.social




February 13, 2025 at 7:32 PM
Dr. Louise Emmett presents OS data from #Enzalutamide +/- #Lu-psma in 1st line mCRPC #ProstateCancer
Intriguing data to be sure but would have appreciated a built in cross-over given equivalent OS seen in #PSMAfore in 2nd line mCRPC when ARPI before or after Lu-psma #GU25 @ascocancer.bsky.social
Intriguing data to be sure but would have appreciated a built in cross-over given equivalent OS seen in #PSMAfore in 2nd line mCRPC when ARPI before or after Lu-psma #GU25 @ascocancer.bsky.social
Dr. Louise Emmett presents OS data from #Enzalutamide +/- #Lu-psma in 1st line mCRPC #ProstateCancer
I especially appreciate Dr. Emmett showing a slide that includes on limitations in her data.
It is required for papers. Probably should be for oral presentations @asco #GU25
I especially appreciate Dr. Emmett showing a slide that includes on limitations in her data.
It is required for papers. Probably should be for oral presentations @asco #GU25

February 13, 2025 at 7:31 PM
Dr. Louise Emmett presents OS data from #Enzalutamide +/- #Lu-psma in 1st line mCRPC #ProstateCancer
I especially appreciate Dr. Emmett showing a slide that includes on limitations in her data.
It is required for papers. Probably should be for oral presentations @asco #GU25
I especially appreciate Dr. Emmett showing a slide that includes on limitations in her data.
It is required for papers. Probably should be for oral presentations @asco #GU25
Dr. Kevin Kelly reviews emerging therapeutic targets in #ProstateCancer @asco #GU25


February 13, 2025 at 6:51 PM
Dr. Kevin Kelly reviews emerging therapeutic targets in #ProstateCancer @asco #GU25