



DropNStretch
@dropnstretch.bsky.social
Resuscitationist | Open-Lung Enthusiast
Reposted by DropNStretch

Say No to Needle Cric Approach
-Open technique w/ Scalpel-Finger-Bougie superior
-Crics are rare + cric kit adds unneeded complexity
-Needle cric fails in a way that is unsalvageable
-Adrenaline impedes your fine motor skills needed for needle based approaches
youtube.com/shorts/WBagE...
#EMIMCC
-Open technique w/ Scalpel-Finger-Bougie superior
-Crics are rare + cric kit adds unneeded complexity
-Needle cric fails in a way that is unsalvageable
-Adrenaline impedes your fine motor skills needed for needle based approaches
youtube.com/shorts/WBagE...
#EMIMCC

Say No to Needle Cric #criticalcare #emergencymedicine #airway
YouTube video by EMSwami
youtube.com
December 29, 2025 at 2:51 PM
Say No to Needle Cric Approach
-Open technique w/ Scalpel-Finger-Bougie superior
-Crics are rare + cric kit adds unneeded complexity
-Needle cric fails in a way that is unsalvageable
-Adrenaline impedes your fine motor skills needed for needle based approaches
youtube.com/shorts/WBagE...
#EMIMCC
-Open technique w/ Scalpel-Finger-Bougie superior
-Crics are rare + cric kit adds unneeded complexity
-Needle cric fails in a way that is unsalvageable
-Adrenaline impedes your fine motor skills needed for needle based approaches
youtube.com/shorts/WBagE...
#EMIMCC
Reposted by DropNStretch

"consensus" guideline on the management of DKA & HHS
with ZERO input from:
- anyone in emergency medicine
- anyone in critical care
- anyone in hospital medicine
the guidelines (published in 2024) contain many antiquated practices and big errors... 🧵#1/3 #EMIMCC
pubmed.ncbi.nlm.nih.gov/39052901/
with ZERO input from:
- anyone in emergency medicine
- anyone in critical care
- anyone in hospital medicine
the guidelines (published in 2024) contain many antiquated practices and big errors... 🧵#1/3 #EMIMCC
pubmed.ncbi.nlm.nih.gov/39052901/

September 28, 2025 at 9:37 PM
"consensus" guideline on the management of DKA & HHS
with ZERO input from:
- anyone in emergency medicine
- anyone in critical care
- anyone in hospital medicine
the guidelines (published in 2024) contain many antiquated practices and big errors... 🧵#1/3 #EMIMCC
pubmed.ncbi.nlm.nih.gov/39052901/
with ZERO input from:
- anyone in emergency medicine
- anyone in critical care
- anyone in hospital medicine
the guidelines (published in 2024) contain many antiquated practices and big errors... 🧵#1/3 #EMIMCC
pubmed.ncbi.nlm.nih.gov/39052901/
Reposted by DropNStretch

ICU Snapshots:
60 yo pt, multiple medical problems (including morbid obesity; BMI 50), admitted to the ICU w ARDS in setting of sepsis. Intubated 08/14 (with 👇CXR), improved w VC-CMVs the next day but the same night became very hypoxic, had to be placed on FiO2 100% / PEEP 12
60 yo pt, multiple medical problems (including morbid obesity; BMI 50), admitted to the ICU w ARDS in setting of sepsis. Intubated 08/14 (with 👇CXR), improved w VC-CMVs the next day but the same night became very hypoxic, had to be placed on FiO2 100% / PEEP 12

August 27, 2025 at 4:15 AM
ICU Snapshots:
60 yo pt, multiple medical problems (including morbid obesity; BMI 50), admitted to the ICU w ARDS in setting of sepsis. Intubated 08/14 (with 👇CXR), improved w VC-CMVs the next day but the same night became very hypoxic, had to be placed on FiO2 100% / PEEP 12
60 yo pt, multiple medical problems (including morbid obesity; BMI 50), admitted to the ICU w ARDS in setting of sepsis. Intubated 08/14 (with 👇CXR), improved w VC-CMVs the next day but the same night became very hypoxic, had to be placed on FiO2 100% / PEEP 12
Reposted by DropNStretch
(Basic) ICU Hemodynamic “Secrets” - Part1:
I know you know them, but let’s remind ourselves of some basic hemodynamic "secrets":
I know you know them, but let’s remind ourselves of some basic hemodynamic "secrets":
August 16, 2025 at 6:23 PM
(Basic) ICU Hemodynamic “Secrets” - Part1:
I know you know them, but let’s remind ourselves of some basic hemodynamic "secrets":
I know you know them, but let’s remind ourselves of some basic hemodynamic "secrets":
Reposted by DropNStretch
ICU Snapshots:
Another nightshift and while checking the chart of a patient admitted during the am shift, I notice this 👇
1. Can anion gap (AGAP) be negative?
To complicate things more:
2. Can anion gap be negative -instead of "very" positive- with a lactate of 14 mmol/l?
Another nightshift and while checking the chart of a patient admitted during the am shift, I notice this 👇
1. Can anion gap (AGAP) be negative?
To complicate things more:
2. Can anion gap be negative -instead of "very" positive- with a lactate of 14 mmol/l?

August 10, 2025 at 6:53 AM
ICU Snapshots:
Another nightshift and while checking the chart of a patient admitted during the am shift, I notice this 👇
1. Can anion gap (AGAP) be negative?
To complicate things more:
2. Can anion gap be negative -instead of "very" positive- with a lactate of 14 mmol/l?
Another nightshift and while checking the chart of a patient admitted during the am shift, I notice this 👇
1. Can anion gap (AGAP) be negative?
To complicate things more:
2. Can anion gap be negative -instead of "very" positive- with a lactate of 14 mmol/l?

Gradual ventilator weaning (vs immediate) in comfort care...less airway issues and gasping, no increased PTSD for family, but nurses faced more stress. Food for thought 🤔
www.pulmccm.org/p/immediate-...
www.pulmccm.org/p/immediate-...

Immediate extubation vs. gradual ventilator weaning in comfort care
No good data exist to guide the process of withdrawal of invasive mechanical ventilation just prior to the end of life–variously known as “terminal extubation,” “compassionate withdrawal,” “extubation...
www.pulmccm.org
July 11, 2025 at 7:08 AM
Gradual ventilator weaning (vs immediate) in comfort care...less airway issues and gasping, no increased PTSD for family, but nurses faced more stress. Food for thought 🤔
www.pulmccm.org/p/immediate-...
www.pulmccm.org/p/immediate-...
Therapeutic heparin?
Hasn’t been in my practice, would love to learn more.
Hasn’t been in my practice, would love to learn more.
July 11, 2025 at 2:18 AM
Therapeutic heparin?
Hasn’t been in my practice, would love to learn more.
Hasn’t been in my practice, would love to learn more.
Insulin (w dextrose gtt), plus standard care. These folks usually do well. Trick is convincing nursing to titrate the dextrose rather than insulin.
July 11, 2025 at 2:16 AM
Insulin (w dextrose gtt), plus standard care. These folks usually do well. Trick is convincing nursing to titrate the dextrose rather than insulin.
Reposted by DropNStretch

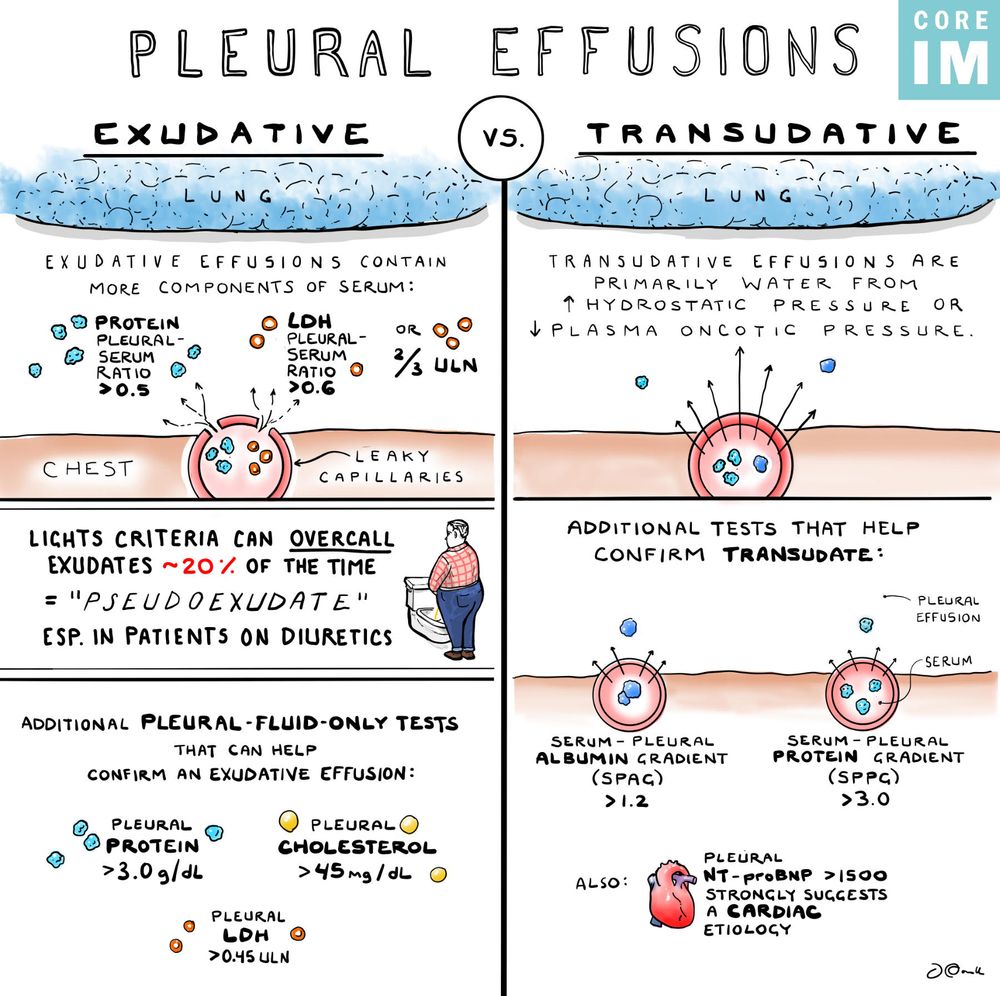
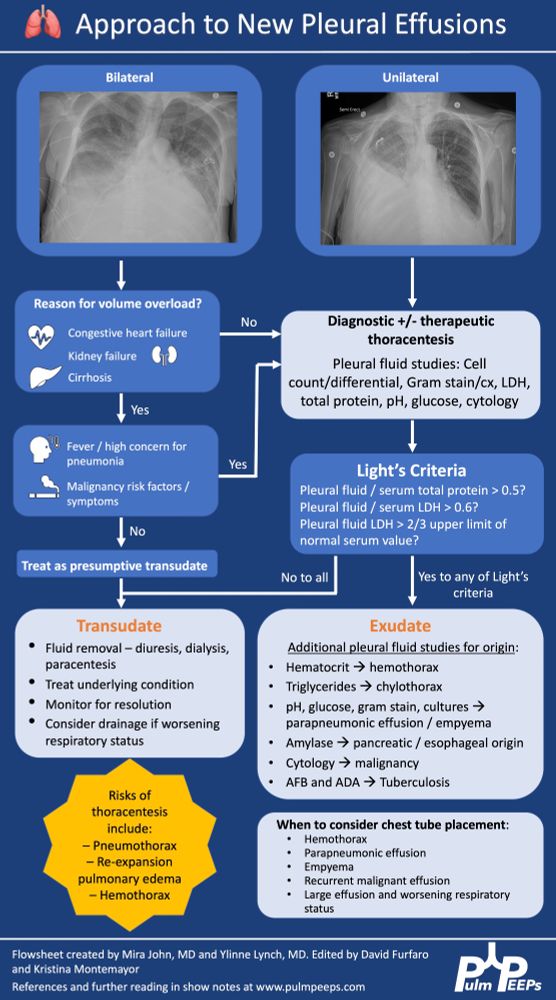
We can't get enough of pleural effusions!! We were so excited to go on @coreimpodcast.bsky.social
to discuss some pearls around pleural effusion diagnosis and management.
If you want more, check out our episodes on effusions, empyema, and malignant effusions!
www.pulmpeeps.com/2025/07/09/1...
to discuss some pearls around pleural effusion diagnosis and management.
If you want more, check out our episodes on effusions, empyema, and malignant effusions!
www.pulmpeeps.com/2025/07/09/1...
July 9, 2025 at 3:41 PM
We can't get enough of pleural effusions!! We were so excited to go on @coreimpodcast.bsky.social
to discuss some pearls around pleural effusion diagnosis and management.
If you want more, check out our episodes on effusions, empyema, and malignant effusions!
www.pulmpeeps.com/2025/07/09/1...
to discuss some pearls around pleural effusion diagnosis and management.
If you want more, check out our episodes on effusions, empyema, and malignant effusions!
www.pulmpeeps.com/2025/07/09/1...
Reposted by DropNStretch

IVC assessments were the "hot new thing" in POCUS when I was a fellow. Today, it's a minimal component of my practice. There are too many variables involved to help one make a volume status decision based solely on this. 🎩 tip to the authors.
eddyjoemd.com/foamed
eddyjoemd.com/foamed

July 7, 2025 at 9:56 AM
IVC assessments were the "hot new thing" in POCUS when I was a fellow. Today, it's a minimal component of my practice. There are too many variables involved to help one make a volume status decision based solely on this. 🎩 tip to the authors.
eddyjoemd.com/foamed
eddyjoemd.com/foamed
Excellent article, sharing w my residents this weekend (for sure).
I also like pulling TWDFNR from this repository from the J Hosp Med. shmpublications.onlinelibrary.wiley.com/journal/1553...
I also like pulling TWDFNR from this repository from the J Hosp Med. shmpublications.onlinelibrary.wiley.com/journal/1553...

Journal of Hospital Medicine
shmpublications.onlinelibrary.wiley.com
June 27, 2025 at 12:09 AM
Excellent article, sharing w my residents this weekend (for sure).
I also like pulling TWDFNR from this repository from the J Hosp Med. shmpublications.onlinelibrary.wiley.com/journal/1553...
I also like pulling TWDFNR from this repository from the J Hosp Med. shmpublications.onlinelibrary.wiley.com/journal/1553...
Reposted by DropNStretch

EMCrit Guest Post - In Defense of Dignity by Chris Hicks, MD [@HumanFact0rz]
emcrit.org/dignity
emcrit.org/dignity

EMCrit Guest Post - In Defense of Dignity by Chris Hicks, MD
Chris Hicks weighs in on dignity
emcrit.org
June 23, 2025 at 4:50 PM
EMCrit Guest Post - In Defense of Dignity by Chris Hicks, MD [@HumanFact0rz]
emcrit.org/dignity
emcrit.org/dignity
Reposted by DropNStretch
Driving Pressure to assess lung protective mech vent
Driving pressure = plateau pressure - PEEP
Target < 15 mm Hg
2015 study(PMID: 25693014): incr driving pressure of 7 mm Hg assoc w/ incr mortality
Drop driving pressure: Incr PEEP, change TV, incr sedation
youtube.com/shorts/YBs_o...
#EMIMCC
Driving pressure = plateau pressure - PEEP
Target < 15 mm Hg
2015 study(PMID: 25693014): incr driving pressure of 7 mm Hg assoc w/ incr mortality
Drop driving pressure: Incr PEEP, change TV, incr sedation
youtube.com/shorts/YBs_o...
#EMIMCC

Driving Pressure #criticalcare #emergencymedicine #ventilators
YouTube video by EMSwami
youtube.com
June 23, 2025 at 2:07 PM
Driving Pressure to assess lung protective mech vent
Driving pressure = plateau pressure - PEEP
Target < 15 mm Hg
2015 study(PMID: 25693014): incr driving pressure of 7 mm Hg assoc w/ incr mortality
Drop driving pressure: Incr PEEP, change TV, incr sedation
youtube.com/shorts/YBs_o...
#EMIMCC
Driving pressure = plateau pressure - PEEP
Target < 15 mm Hg
2015 study(PMID: 25693014): incr driving pressure of 7 mm Hg assoc w/ incr mortality
Drop driving pressure: Incr PEEP, change TV, incr sedation
youtube.com/shorts/YBs_o...
#EMIMCC
Reposted by DropNStretch
standard approaches to dosing hypertonic therapy are flawed
🧂for hyponatremia, reviews often recommend homeopathically low doses (eg 100cc of 3%)
🧂for elevated intracranial pressure, common practice is to use fixed doses (eg 30 cc 23.4% saline for everyone)
can we do better?... 🧵 #1/2
#EMIMCC
🧂for hyponatremia, reviews often recommend homeopathically low doses (eg 100cc of 3%)
🧂for elevated intracranial pressure, common practice is to use fixed doses (eg 30 cc 23.4% saline for everyone)
can we do better?... 🧵 #1/2
#EMIMCC
a man with a mustache and sunglasses is pouring salt on his face .
ALT: a man with a mustache and sunglasses is pouring salt on his face .
media.tenor.com
June 24, 2025 at 12:27 PM
standard approaches to dosing hypertonic therapy are flawed
🧂for hyponatremia, reviews often recommend homeopathically low doses (eg 100cc of 3%)
🧂for elevated intracranial pressure, common practice is to use fixed doses (eg 30 cc 23.4% saline for everyone)
can we do better?... 🧵 #1/2
#EMIMCC
🧂for hyponatremia, reviews often recommend homeopathically low doses (eg 100cc of 3%)
🧂for elevated intracranial pressure, common practice is to use fixed doses (eg 30 cc 23.4% saline for everyone)
can we do better?... 🧵 #1/2
#EMIMCC
Reposted by DropNStretch
The ideal cutoff for adequate time-to-antibiotic delivery in septic shock is being discussed again 🤦♂️
Should we be required to give antibiotics in 1 hr? 3 hr? 15 minutes? 3.14159 minutes?
This is worth a short thread on the background of this topic
Buckle up, it's a mess... #EMIMCC #IDsky #1/6
Should we be required to give antibiotics in 1 hr? 3 hr? 15 minutes? 3.14159 minutes?
This is worth a short thread on the background of this topic
Buckle up, it's a mess... #EMIMCC #IDsky #1/6
a man with a surprised look on his face and the words how did this happen below him
ALT: a man with a surprised look on his face and the words how did this happen below him
media.tenor.com
June 9, 2025 at 12:04 PM
Reposted by DropNStretch
did you think that labetalol is a single drug?
nope
it’s actually a mixture of FOUR different drugs
RS, RR, SS, and SR-labetalol
and this is clinically relevant!
lets discuss why…
🧵 #1/3 #EMIMCC
nope
it’s actually a mixture of FOUR different drugs
RS, RR, SS, and SR-labetalol
and this is clinically relevant!
lets discuss why…
🧵 #1/3 #EMIMCC
May 11, 2025 at 4:45 PM
did you think that labetalol is a single drug?
nope
it’s actually a mixture of FOUR different drugs
RS, RR, SS, and SR-labetalol
and this is clinically relevant!
lets discuss why…
🧵 #1/3 #EMIMCC
nope
it’s actually a mixture of FOUR different drugs
RS, RR, SS, and SR-labetalol
and this is clinically relevant!
lets discuss why…
🧵 #1/3 #EMIMCC
Reposted by DropNStretch
generalized convulsive status epilepticus update:
feels like it's time to add IV ketamine as a 2nd line agent before intubation 👇
thoughts/opinions?
rationale explained here: pubmed.ncbi.nlm.nih.gov/36609129/
evidence is accumulating eg, pubmed.ncbi.nlm.nih.gov/37610640/ #EMIMCC
feels like it's time to add IV ketamine as a 2nd line agent before intubation 👇
thoughts/opinions?
rationale explained here: pubmed.ncbi.nlm.nih.gov/36609129/
evidence is accumulating eg, pubmed.ncbi.nlm.nih.gov/37610640/ #EMIMCC

April 16, 2025 at 2:18 PM
generalized convulsive status epilepticus update:
feels like it's time to add IV ketamine as a 2nd line agent before intubation 👇
thoughts/opinions?
rationale explained here: pubmed.ncbi.nlm.nih.gov/36609129/
evidence is accumulating eg, pubmed.ncbi.nlm.nih.gov/37610640/ #EMIMCC
feels like it's time to add IV ketamine as a 2nd line agent before intubation 👇
thoughts/opinions?
rationale explained here: pubmed.ncbi.nlm.nih.gov/36609129/
evidence is accumulating eg, pubmed.ncbi.nlm.nih.gov/37610640/ #EMIMCC
Reposted by DropNStretch

The upside of defining contrast nephropathy in this way is it becomes very easy to measure the incidence of AKI. In 6 recent well done studies, the incidence runs from 1 to 11% among patients with CKD.
December 1, 2024 at 9:14 PM
The upside of defining contrast nephropathy in this way is it becomes very easy to measure the incidence of AKI. In 6 recent well done studies, the incidence runs from 1 to 11% among patients with CKD.
Used often in my trauma-SICU for multi modal analgesia, and with good effect. Reaching for this early if targeting MSK pain especially. Good drug IMO.
February 15, 2025 at 3:41 PM
Used often in my trauma-SICU for multi modal analgesia, and with good effect. Reaching for this early if targeting MSK pain especially. Good drug IMO.
Reposted by DropNStretch

We discussed this and it was so interesting how many different rounding strategies there are. I found out that there are attendings who want them to preround, then table round, then bedside round all together. ☠️
Clearly that’s too much rounding. I wonder though if we
Clearly that’s too much rounding. I wonder though if we
Our discussion article for Thursday conference and I can’t wait to hear what everyone thinks.

January 17, 2025 at 2:04 PM
We discussed this and it was so interesting how many different rounding strategies there are. I found out that there are attendings who want them to preround, then table round, then bedside round all together. ☠️
Clearly that’s too much rounding. I wonder though if we
Clearly that’s too much rounding. I wonder though if we
Challenging, yes. Learnable, yes. Awesome and amazing post, ABSOLUTELY!
Thx for sharing the knowledge!
Thx for sharing the knowledge!
January 4, 2025 at 4:59 AM
Challenging, yes. Learnable, yes. Awesome and amazing post, ABSOLUTELY!
Thx for sharing the knowledge!
Thx for sharing the knowledge!
Challenging, yes. Learnable, yes. Awesome and amazing post, ABSOLUTELY!
Thx for sharing the knowledge!
Thx for sharing the knowledge!
January 4, 2025 at 4:57 AM
Challenging, yes. Learnable, yes. Awesome and amazing post, ABSOLUTELY!
Thx for sharing the knowledge!
Thx for sharing the knowledge!
Reposted by DropNStretch
3 Changes to Practice 2024
1️⃣Vasopressin is back: use early in cirrhosis + massive PE
2️⃣O2 sat tracing as marker of perfusion. Poor waveform = poor perfusion. Augment w/ pressors, blood, fluids etc
3️⃣Paralytic 1st in RSI: Time drugs so simultaneous onset
#MedSky #EMIMCC
youtube.com/shorts/RwQwK...
1️⃣Vasopressin is back: use early in cirrhosis + massive PE
2️⃣O2 sat tracing as marker of perfusion. Poor waveform = poor perfusion. Augment w/ pressors, blood, fluids etc
3️⃣Paralytic 1st in RSI: Time drugs so simultaneous onset
#MedSky #EMIMCC
youtube.com/shorts/RwQwK...

3 Additions to Practice From 2024 #emergencymed #emergencymedicine #criticalcare #resuscitation
YouTube video by EMSwami
youtube.com
January 3, 2025 at 2:54 PM
3 Changes to Practice 2024
1️⃣Vasopressin is back: use early in cirrhosis + massive PE
2️⃣O2 sat tracing as marker of perfusion. Poor waveform = poor perfusion. Augment w/ pressors, blood, fluids etc
3️⃣Paralytic 1st in RSI: Time drugs so simultaneous onset
#MedSky #EMIMCC
youtube.com/shorts/RwQwK...
1️⃣Vasopressin is back: use early in cirrhosis + massive PE
2️⃣O2 sat tracing as marker of perfusion. Poor waveform = poor perfusion. Augment w/ pressors, blood, fluids etc
3️⃣Paralytic 1st in RSI: Time drugs so simultaneous onset
#MedSky #EMIMCC
youtube.com/shorts/RwQwK...