




Critical Care Notes
@criticalcarenotes.bsky.social
Critical Care Nurse Practitioner. FCCM. One half of the icuscenarios.com podcast and the icu101.com team. criticalcarenotes.com
Reposted by Critical Care Notes

Remembering the most likely mediator of reduced mortality in the original EGDT therapy was the presence of the CI in the intervention arm, the regular attendance of an interested and informed clinician (and skilled ICU nurse) likely has a bigger impact than any single drug or intervention.

"One intangible advantage of capillary refill time is that performing it brings the clinician back to the bedside to reassess the patient. This act may be itself the holy grail of early sepsis management."
great piece on #sepsis
great piece on #sepsis

💬 Editorial: While capillary refill time shows promise for early #SepticShock management, integrating it into broader, multimodal resuscitation strategies remains key to improving outcomes.
#LIVES2025 @esicm.bsky.social
ja.ma/4hAs5u7
#LIVES2025 @esicm.bsky.social
ja.ma/4hAs5u7
October 29, 2025 at 4:08 PM
Remembering the most likely mediator of reduced mortality in the original EGDT therapy was the presence of the CI in the intervention arm, the regular attendance of an interested and informed clinician (and skilled ICU nurse) likely has a bigger impact than any single drug or intervention.

Reposted by Critical Care Notes

Just updated the IBCC chapter on cholecystitis & cholangitis.
These patients are often initially triaged to the ICU.
Understanding these diseases can help us direct patients to interventions they need.
Let’s talk about four pearls 😁
chapter: emcrit.org/ibcc/biliary... #EMIMCC
These patients are often initially triaged to the ICU.
Understanding these diseases can help us direct patients to interventions they need.
Let’s talk about four pearls 😁
chapter: emcrit.org/ibcc/biliary... #EMIMCC
a woman in a pearl costume says pearls
ALT: a woman in a pearl costume says pearls
media.tenor.com
October 19, 2025 at 1:11 PM
Just updated the IBCC chapter on cholecystitis & cholangitis.
These patients are often initially triaged to the ICU.
Understanding these diseases can help us direct patients to interventions they need.
Let’s talk about four pearls 😁
chapter: emcrit.org/ibcc/biliary... #EMIMCC
These patients are often initially triaged to the ICU.
Understanding these diseases can help us direct patients to interventions they need.
Let’s talk about four pearls 😁
chapter: emcrit.org/ibcc/biliary... #EMIMCC
Reposted by Critical Care Notes
A man in his 50s seeks the ED for the umpteenth time since his abdo pain started a few years ago. He says that it’s his gallbladder, surgery has been denied because of diffuse pain and normal blood tests. Today CRP 9, Leukocytes 11. #POCUS He got his operation the next day. #EMIMCC
October 9, 2025 at 9:45 AM
Point-of-care ultrasound is being used by an increasing number of nurse practitioners, but its utility is not limited to the ICU, nor even to Acute Care.
journals.lww.com/jaanp/abstra...
journals.lww.com/jaanp/abstra...
Expanding the horizon: The case for point-of-care... : Journal of the American Association of Nurse Practitioners
enhanced diagnostic accuracy, faster decision-making, and improved patient satisfaction. With growing access to affordable handheld devices and expanding educational opportunities, POCUS is becoming i...
journals.lww.com
August 7, 2025 at 9:04 PM
Point-of-care ultrasound is being used by an increasing number of nurse practitioners, but its utility is not limited to the ICU, nor even to Acute Care.
journals.lww.com/jaanp/abstra...
journals.lww.com/jaanp/abstra...
Reposted by Critical Care Notes
rapidly pushing IV calcium may cause:
😦 vasodilation, bradycardia, hypotension
😦 nausea/vomiting, flushing
if patients are conscious, this can make them feel horrible
if the patient is obtunded & not intubated, emesis can be a big problem
whenever possible, give IV Ca slowly #EMIMCC
😦 vasodilation, bradycardia, hypotension
😦 nausea/vomiting, flushing
if patients are conscious, this can make them feel horrible
if the patient is obtunded & not intubated, emesis can be a big problem
whenever possible, give IV Ca slowly #EMIMCC

a man wearing sunglasses and a green shirt with breaking bobby bones on the bottom
ALT: a man wearing sunglasses and a green shirt with breaking bobby bones on the bottom
media.tenor.com
August 1, 2025 at 6:08 PM
rapidly pushing IV calcium may cause:
😦 vasodilation, bradycardia, hypotension
😦 nausea/vomiting, flushing
if patients are conscious, this can make them feel horrible
if the patient is obtunded & not intubated, emesis can be a big problem
whenever possible, give IV Ca slowly #EMIMCC
😦 vasodilation, bradycardia, hypotension
😦 nausea/vomiting, flushing
if patients are conscious, this can make them feel horrible
if the patient is obtunded & not intubated, emesis can be a big problem
whenever possible, give IV Ca slowly #EMIMCC
The other thing to remember is that patients in HFNC typically benefit more from “flow” than FiO2. So wean the FiO2 before the flow.

Another thing I hear often in the ICU is this:
The patient is on high-flow nasal cannula (HFNC) (or high-flow oxymask)
When I specifically ask "how many liters?", often the answer is: 6 or 7 l/min
HFNC is a respiratory support system delivering heated-humidified O2 @
The patient is on high-flow nasal cannula (HFNC) (or high-flow oxymask)
When I specifically ask "how many liters?", often the answer is: 6 or 7 l/min
HFNC is a respiratory support system delivering heated-humidified O2 @

August 1, 2025 at 10:25 PM
The other thing to remember is that patients in HFNC typically benefit more from “flow” than FiO2. So wean the FiO2 before the flow.
And remember, ST is often compensatory. Don’t slow it down blindly.

🫀 Sinus tachycardia = a sign, not a diagnosis.
Don’t just treat the rate—find the cause.
Use this 8-point checklist & skip reflexive beta blockers.
🎧 REBEL Core Cast 137: https://wp.me/pdrP8b-5nI
#EMIMCC #FOAMed #MedEd #MedSky
Don’t just treat the rate—find the cause.
Use this 8-point checklist & skip reflexive beta blockers.
🎧 REBEL Core Cast 137: https://wp.me/pdrP8b-5nI
#EMIMCC #FOAMed #MedEd #MedSky



July 22, 2025 at 9:34 AM
And remember, ST is often compensatory. Don’t slow it down blindly.
“But WHY did they fail?” All too often I get, “they failed SBT” from someone who also wasn’t there, and that’s that. Do it again and see for yourself. Often you can get them off the vent after all.
great thread on SBTs
💨 if someone “failed” for unclear reasons before your shift, repeat the SBT with direct observation
💨 look for treatable causes of SBT failure
-but-
💨 for most patients, repeating multiple SBTs daily doesn’t help
more: emcrit.org/ibcc/extubat... #EMIMCC
💨 if someone “failed” for unclear reasons before your shift, repeat the SBT with direct observation
💨 look for treatable causes of SBT failure
-but-
💨 for most patients, repeating multiple SBTs daily doesn’t help
more: emcrit.org/ibcc/extubat... #EMIMCC
ICU Practice:
The conventional teaching is to perform spontaneous breathing trials (SBT) only once daily when we try to wean a patient from mechanical ventilation. The rationale is to prevent precipitating respiratory muscle fatigue. It has been shown that SBT failures are often
The conventional teaching is to perform spontaneous breathing trials (SBT) only once daily when we try to wean a patient from mechanical ventilation. The rationale is to prevent precipitating respiratory muscle fatigue. It has been shown that SBT failures are often
July 22, 2025 at 9:33 AM
“But WHY did they fail?” All too often I get, “they failed SBT” from someone who also wasn’t there, and that’s that. Do it again and see for yourself. Often you can get them off the vent after all.
Big news for lung ultrasound #POCUS
This is the summary of the recommendations:
1. Lung ultrasound versus chest x-ray to diagnose CAP
For adults with suspected CAP, we suggest lung US is an acceptable diagnostic alternative to CXR in medical centers where appropriate clinical expertise exists
1. Lung ultrasound versus chest x-ray to diagnose CAP
For adults with suspected CAP, we suggest lung US is an acceptable diagnostic alternative to CXR in medical centers where appropriate clinical expertise exists
July 21, 2025 at 12:14 PM
Big news for lung ultrasound #POCUS
I sadly see this not rarely. Especially with overworked interns. They run out of time and rather than admit this, and risk being perceived as failing, they lie. And they ALWAYS get caught.
Advice for New Trainees #5: Never Lie. It’s not worth to tell what may seem like a small lie to cover up for something you forgot to check or do.
Better to simply say, “I don’t know or I didn’t check. Let me find out and I’ll get back to you.”
youtube.com/shorts/x6L6G...
#EMIMCC
Better to simply say, “I don’t know or I didn’t check. Let me find out and I’ll get back to you.”
youtube.com/shorts/x6L6G...
#EMIMCC

Advice for New Trainees 5: Never Lie #emergencymedicine #residents #internship
YouTube video by EMSwami
youtube.com
July 4, 2025 at 11:40 PM
I sadly see this not rarely. Especially with overworked interns. They run out of time and rather than admit this, and risk being perceived as failing, they lie. And they ALWAYS get caught.
I’ll add to this, communicate when you want to be called. Don’t just start NE with a MAP goal>65, add, “call me if you get to X.” This prevents you getting busy and checking back to find that they’re almost maxed.
Advice for New Trainees #3: Communicate
If you want something done, not enough to just order it
Best approach: put orders in, find nurse + discuss
Gives nurse opportunity to share observations, clarify orders, catch errors + creates a shared mental model
youtube.com/shorts/nLh20...
#EMIMCC
If you want something done, not enough to just order it
Best approach: put orders in, find nurse + discuss
Gives nurse opportunity to share observations, clarify orders, catch errors + creates a shared mental model
youtube.com/shorts/nLh20...
#EMIMCC

Advice for New Trainees 3: Communicate #emergencymedicine #residents #internship
YouTube video by EMSwami
youtube.com
July 2, 2025 at 8:51 PM
I’ll add to this, communicate when you want to be called. Don’t just start NE with a MAP goal>65, add, “call me if you get to X.” This prevents you getting busy and checking back to find that they’re almost maxed.
Reposted by Critical Care Notes

Occult VF in Cardiac Arrest: 5.3% of patients with cardiac arrest showed VF on echo but ECG w/ PEA/asystole
Study does not show improved outcomes but not powered to do so
Strong argument for intra-arrest echo as it can dramatically change management
#EMIMCC
Study does not show improved outcomes but not powered to do so
Strong argument for intra-arrest echo as it can dramatically change management
#EMIMCC
July 1, 2025 at 5:44 PM
Occult VF in Cardiac Arrest: 5.3% of patients with cardiac arrest showed VF on echo but ECG w/ PEA/asystole
Study does not show improved outcomes but not powered to do so
Strong argument for intra-arrest echo as it can dramatically change management
#EMIMCC
Study does not show improved outcomes but not powered to do so
Strong argument for intra-arrest echo as it can dramatically change management
#EMIMCC
Reposted by Critical Care Notes
Advice for New Trainees #2: Listen to your nurses
Don’t mistake your short time as a doctor as equivalent clinically to their years and decades of experience
If a nurse asks you to reevaluate a patient, GO TO THE BEDSIDE AND RE-EVALUTE THE PATIENT, EVERY TIME.
youtube.com/shorts/c0o5F...
#EMIMCC
Don’t mistake your short time as a doctor as equivalent clinically to their years and decades of experience
If a nurse asks you to reevaluate a patient, GO TO THE BEDSIDE AND RE-EVALUTE THE PATIENT, EVERY TIME.
youtube.com/shorts/c0o5F...
#EMIMCC
Advice for Interns 2: Listen to The Nurses #emergencymedicine #internship #residents
YouTube video by EMSwami
youtube.com
July 1, 2025 at 2:02 PM
Advice for New Trainees #2: Listen to your nurses
Don’t mistake your short time as a doctor as equivalent clinically to their years and decades of experience
If a nurse asks you to reevaluate a patient, GO TO THE BEDSIDE AND RE-EVALUTE THE PATIENT, EVERY TIME.
youtube.com/shorts/c0o5F...
#EMIMCC
Don’t mistake your short time as a doctor as equivalent clinically to their years and decades of experience
If a nurse asks you to reevaluate a patient, GO TO THE BEDSIDE AND RE-EVALUTE THE PATIENT, EVERY TIME.
youtube.com/shorts/c0o5F...
#EMIMCC
Reposted by Critical Care Notes

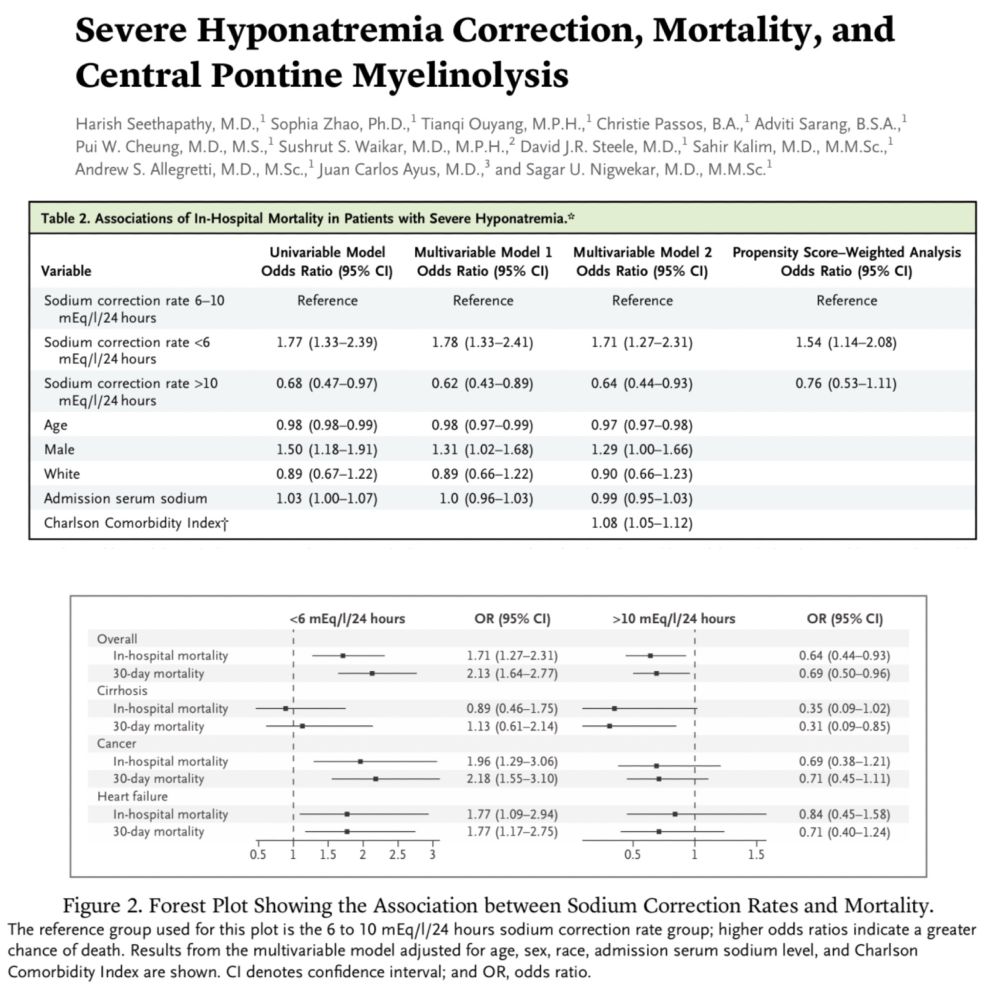
Might we be correcting hyponatremia too slowly? May our patients be suffering because we're too fearful of the risk of central pontine myelinolysis? Here's data that may challenge our regular approach. Hat tip to the authors.
eddyjoemd.com/foamed
eddyjoemd.com/foamed
June 26, 2025 at 10:51 AM
Might we be correcting hyponatremia too slowly? May our patients be suffering because we're too fearful of the risk of central pontine myelinolysis? Here's data that may challenge our regular approach. Hat tip to the authors.
eddyjoemd.com/foamed
eddyjoemd.com/foamed
Interesting. Had never thought of this before. How many other things in medicine to we get wrong because if assumptions?

The Bernoulli equation (simplified to 4 * V squared) is used in every echo to estimate pressure gradients from velocities. One source of error is widely ignored I belive. #echofirst #pocus #emimcc
June 27, 2025 at 11:45 AM
Interesting. Had never thought of this before. How many other things in medicine to we get wrong because if assumptions?
Reposted by Critical Care Notes

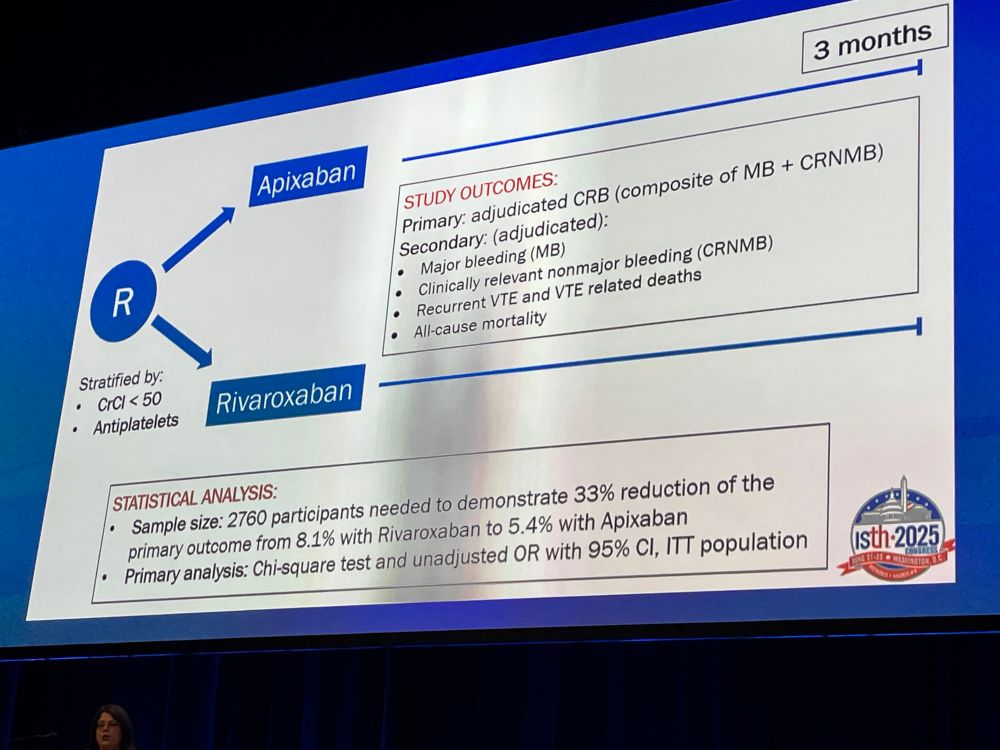
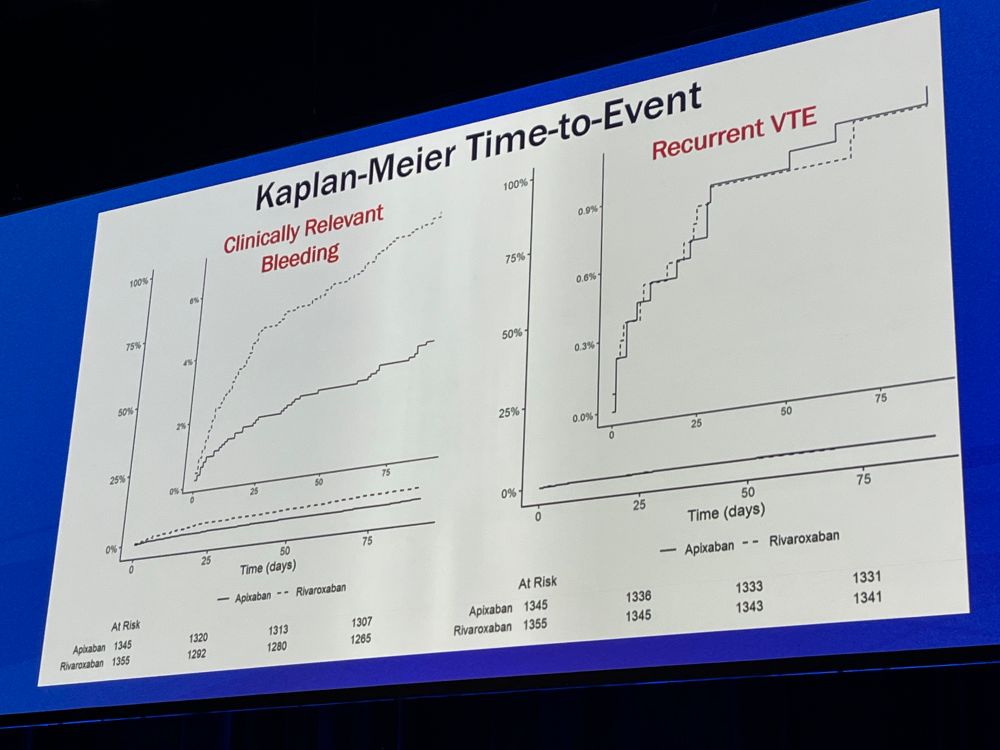
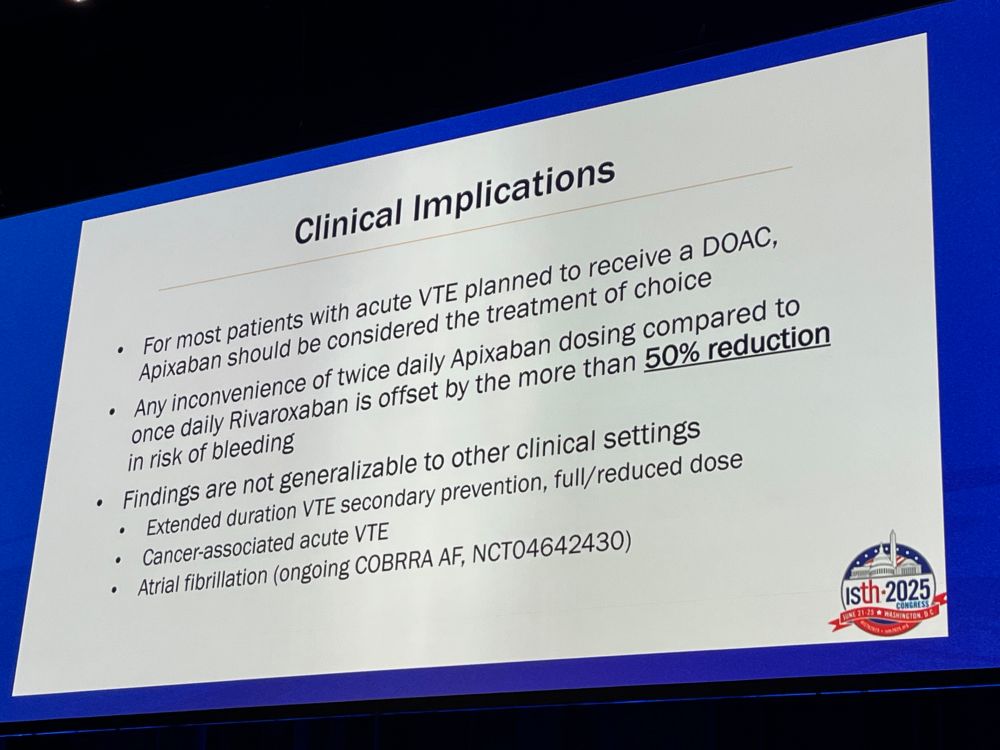
This is what we were waiting for. A direct comparison between apixaban and rivaroxaban for the treatment of acute VTE. Apixaban reduces bleeding risk in the first 3 months by >50%!
Practice changing investigator-initiated RCT.
#ISTH2025
Practice changing investigator-initiated RCT.
#ISTH2025

June 22, 2025 at 1:49 PM
This is what we were waiting for. A direct comparison between apixaban and rivaroxaban for the treatment of acute VTE. Apixaban reduces bleeding risk in the first 3 months by >50%!
Practice changing investigator-initiated RCT.
#ISTH2025
Practice changing investigator-initiated RCT.
#ISTH2025
Reposted by Critical Care Notes
June 17, 2025 at 7:21 PM
Mottling is one of this signs that gets me real worried.
When a patient presents with mottling among their constellation of signs, symptoms, and labs, there is a look that team members give each other that we've all seen. It's not a positive look. Here is some data reinforcing our intuition. 🎩 tip to the authors.
eddyjoemd.com/foamed
eddyjoemd.com/foamed

June 16, 2025 at 12:24 PM
Mottling is one of this signs that gets me real worried.
Reposted by Critical Care Notes
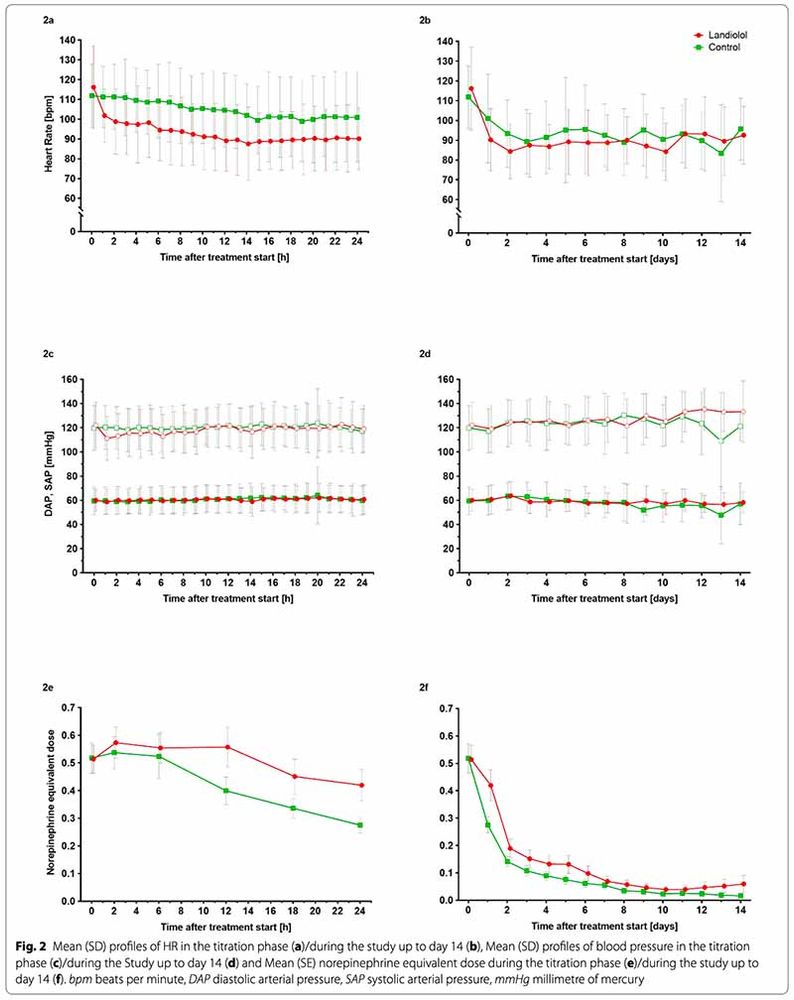
beta-blocker in sepsis trials continue to mystify me
you have patients on reasonable doses of pressor (0.5 mcg/kg/min norepi equivalent) with an average MAP ~80 (mean diastolic BP ~60!)
you're worried about catecholamine toxicity
instead of reducing the pressors you add a beta-blocker😳 #EMIMCC
you have patients on reasonable doses of pressor (0.5 mcg/kg/min norepi equivalent) with an average MAP ~80 (mean diastolic BP ~60!)
you're worried about catecholamine toxicity
instead of reducing the pressors you add a beta-blocker😳 #EMIMCC

June 14, 2025 at 12:21 PM
beta-blocker in sepsis trials continue to mystify me
you have patients on reasonable doses of pressor (0.5 mcg/kg/min norepi equivalent) with an average MAP ~80 (mean diastolic BP ~60!)
you're worried about catecholamine toxicity
instead of reducing the pressors you add a beta-blocker😳 #EMIMCC
you have patients on reasonable doses of pressor (0.5 mcg/kg/min norepi equivalent) with an average MAP ~80 (mean diastolic BP ~60!)
you're worried about catecholamine toxicity
instead of reducing the pressors you add a beta-blocker😳 #EMIMCC
Don’t be distracted by the obvious pleural yuck…
ICU Snapshots:
If you have a sharp eye, what is the worse finding here 👇?
If you have a sharp eye, what is the worse finding here 👇?
June 16, 2025 at 12:17 PM
Don’t be distracted by the obvious pleural yuck…
My students know well of my disdain for the d-diner…

No, no. Wells is the scientist’s name, you’re referring to Wells’ monster. #emimcc
![From MD calc: “The model should be applied only after a history and physical suggests that venous thromboembolism is a diagnostic possibility. it should not be applied to all patients with chest pain or dyspnea or to all patients with leg pain or swelling. This is the most common mistake made. Also, never never do the D-dimer first [before history and physical exam]. The monster in the box is that the D-dimer is done first and is positive (as it is for many patients with non-VTE conditions)”](https://cdn.bsky.app/img/feed_thumbnail/plain/did:plc:amklqog4avjkgvhzaqalqwhy/bafkreigzqtiwelw4ypqnvqcvs2v5rjsuqmvrtj27hllxwoci3i2x4bxxv4@jpeg)
June 16, 2025 at 12:16 PM
My students know well of my disdain for the d-diner…
Anyone ever done peer review for Optum InterQual? I was approached about doing some reviews but not sure what to make of it. Sounds good, they send you material in your area of expertise and you review it for accuracy. I’ve done similar work before but never heard of this particular company.
April 23, 2025 at 10:20 PM
Anyone ever done peer review for Optum InterQual? I was approached about doing some reviews but not sure what to make of it. Sounds good, they send you material in your area of expertise and you review it for accuracy. I’ve done similar work before but never heard of this particular company.
Reposted by Critical Care Notes
Episode 86: EEGs in the ICU with Carolina Maciel – Critical Care Scenarios
icuscenarios.com
April 16, 2025 at 3:05 PM