



Andrew Vickers
@vickersbiostats.bsky.social
Biostatistician at Memorial Sloan Kettering Cancer Center. Special interest in prostate cancer, risk prediction, patient-reported outcomes, decision-making.
RCT n= ~1500. >90% of patients walking through the door with target indication were randomized. Zero funding. Clinical integration and rethinking informed consent transformational. journals.lww.com/anesthesiolo...
journals.lww.com
November 10, 2025 at 9:23 PM
RCT n= ~1500. >90% of patients walking through the door with target indication were randomized. Zero funding. Clinical integration and rethinking informed consent transformational. journals.lww.com/anesthesiolo...
Reposted by Andrew Vickers

Gosh, who could have predicted that the men who complained that they were being "censored!" during the pandemic phase of Covid (Prasad, Bhattacharya) are now leading the nation's health agencies & CENSORING others?
"staffers are terrified of pushing back on Prasad, lest they face retaliation"
"staffers are terrified of pushing back on Prasad, lest they face retaliation"

EXCLUSIVE: A slow-boiling feud between Vinay Prasad and his staff at the FDA is threatening the future of the center that regulates the nation’s vaccines, biological products, and blood supply. Read more here:
www.statnews.com/2025/10/31/v...
www.statnews.com/2025/10/31/v...

Under Vinay Prasad, employees at a key FDA center fear speaking out, look for the exits
Exclusive: Vinay Prasad has rattled FDA staff by expanding his power and pushing out senior leaders.
www.statnews.com
October 31, 2025 at 4:28 PM
Gosh, who could have predicted that the men who complained that they were being "censored!" during the pandemic phase of Covid (Prasad, Bhattacharya) are now leading the nation's health agencies & CENSORING others?
"staffers are terrified of pushing back on Prasad, lest they face retaliation"
"staffers are terrified of pushing back on Prasad, lest they face retaliation"
Recently been debating "cancer screening skeptics" about endpoints in screening RCTs. They insist on overall survival (OS); when I point out feasibility issues, they say infeasibility of RCT on OS proves screening doesn't work. Prejudice masquerading as methodologic rigor.
October 30, 2025 at 3:26 PM
Recently been debating "cancer screening skeptics" about endpoints in screening RCTs. They insist on overall survival (OS); when I point out feasibility issues, they say infeasibility of RCT on OS proves screening doesn't work. Prejudice masquerading as methodologic rigor.
Reposted by Andrew Vickers

Appreciated this editorial on the long term results from the prostate cancer screening trial. It's hard to believe we are doing the best we can be when it comes to this screening tool. Screening effectiveness needs to be re-evaluated over time as practices change.
www.nejm.org/doi/full/10....
www.nejm.org/doi/full/10....

Early Detection of Prostate Cancer — Time to Fish or Cut Bait | NEJM
Approaches to early detection of cancer often seem contentious, but the big-picture view is actually one of remarkable consensus. All major guideline groups recommend the Papanicolaou smear, mammog...
www.nejm.org
October 30, 2025 at 1:23 PM
Appreciated this editorial on the long term results from the prostate cancer screening trial. It's hard to believe we are doing the best we can be when it comes to this screening tool. Screening effectiveness needs to be re-evaluated over time as practices change.
www.nejm.org/doi/full/10....
www.nejm.org/doi/full/10....
After my son’s team lost in semi-finals of frisbee nationals 2024, he wrote to team “I love you all. This is how we do better next year …”. 2025: national champions. Something for science to learn from the sporting world: respect and motivate your team and good things will happen.

October 29, 2025 at 2:09 PM
After my son’s team lost in semi-finals of frisbee nationals 2024, he wrote to team “I love you all. This is how we do better next year …”. 2025: national champions. Something for science to learn from the sporting world: respect and motivate your team and good things will happen.
Folks (Prasad etc) who say “cancer screening must improve overall survival”, let's take a real example, ovarian cancer. ~0.7% mortality; salpingectomy reduces risk by ≥50%. Trial could be powered on cancer mortality (n~20,000) vs. overall (n~750,000). Which would you recommend?
October 28, 2025 at 3:03 AM
Folks (Prasad etc) who say “cancer screening must improve overall survival”, let's take a real example, ovarian cancer. ~0.7% mortality; salpingectomy reduces risk by ≥50%. Trial could be powered on cancer mortality (n~20,000) vs. overall (n~750,000). Which would you recommend?
Whether / how to do PSA screening complex topic highly dependent on detailed knowledge. Plenty of room for reasonable disagreement. But I’m getting pretty tired of self-proclaimed skeptics who, without specialist knowledge, smugly condescend anyone supporting PSA as naive.
October 16, 2025 at 2:29 PM
Whether / how to do PSA screening complex topic highly dependent on detailed knowledge. Plenty of room for reasonable disagreement. But I’m getting pretty tired of self-proclaimed skeptics who, without specialist knowledge, smugly condescend anyone supporting PSA as naive.
Very common to ask patients to rate pain from "no pain" (0) to "worst pain imaginable / possible" (10). Here is a randomized trial showing anchor for pain score of 10 should be "extreme pain" (TL;DR: we want to evaluate pain, not imagination) pmc.ncbi.nlm.nih.gov/articles/PMC...
Client Challenge
jpro.springeropen.com
October 13, 2025 at 3:08 PM
Very common to ask patients to rate pain from "no pain" (0) to "worst pain imaginable / possible" (10). Here is a randomized trial showing anchor for pain score of 10 should be "extreme pain" (TL;DR: we want to evaluate pain, not imagination) pmc.ncbi.nlm.nih.gov/articles/PMC...
Guidelines group argues against lymph node dissection in radical prostatectomy by cherry-picking outlying studies eg systematic review finds 5 studies on lymphedema only 1 with p<5%; authors cite that one study and ignore systematic review. www.europeanurology.com/article/S030...
Re: Matthew J. Roberts, Giorgio Gandaglia, Daniela E. Oprea-Lager, et al. Pelvic Lymph Node Dissection in Prostate Cancer: Evidence and Implications. Eur Urol 2025;87:619–21
There is an ongoing debate about whether the benefits of lymph node dissection (LND)
during radical prostatectomy outweigh the harms. We previously published a commentary
describing how opponents of L...
www.europeanurology.com
October 7, 2025 at 10:33 AM
Guidelines group argues against lymph node dissection in radical prostatectomy by cherry-picking outlying studies eg systematic review finds 5 studies on lymphedema only 1 with p<5%; authors cite that one study and ignore systematic review. www.europeanurology.com/article/S030...
All wrapped up in a neat little bow. Covid conspiracy theorist encourages her lymphoma afflicted daughter to refuse chemotherapy. The daughter dies. The mother blames paramedics for the death. www.theguardian.com/society/2025...

UK woman who refused cancer drugs was influenced by mother, inquest finds
Paloma Shemirani, 23, died after refusing chemotherapy for non-Hodgkin lymphoma despite doctors’ concerns
www.theguardian.com
October 2, 2025 at 3:31 PM
All wrapped up in a neat little bow. Covid conspiracy theorist encourages her lymphoma afflicted daughter to refuse chemotherapy. The daughter dies. The mother blames paramedics for the death. www.theguardian.com/society/2025...
Large multicenter study: "When grade group discordant between systematic & targeted biopsy, risk is intermediate. Current approach assigning highest grade should be abandoned ... consider de-escalating treatment when grade discordant." academic.oup.com/jnci/advance...

Assessing the oncologic risk when systematic and multiparametric magnetic resonance imaging-targeted prostate biopsy grade groups are discordant
AbstractBackground and Objective. In the systematic biopsy (SBx) era, prostate biopsy grading followed the rule that the ISUP grade group (GG) assigned was
academic.oup.com
September 29, 2025 at 3:57 PM
Large multicenter study: "When grade group discordant between systematic & targeted biopsy, risk is intermediate. Current approach assigning highest grade should be abandoned ... consider de-escalating treatment when grade discordant." academic.oup.com/jnci/advance...
Reposted by Andrew Vickers

My theory of medical evidence is simple: observational studies for me, RCTs for you.

September 23, 2025 at 11:21 AM
My theory of medical evidence is simple: observational studies for me, RCTs for you.
Remarkable study from the Malmo Preventive Project: ~1000 men with blood at 60 in 1981; no PSA screening, *lifetime* follow-up. >50% life years lost to prostate cancer in PSA>4.0; 85% for PSA >2.0. Focus screening for men in 60s in men with higher PSAs! academic.oup.com/jnci/advance...
Prostate-specific antigen levels at age 60 and lifetime risk of lethal prostate cancer
AbstractIntroduction. We investigated the natural history of the relationship between PSA at age 60 and lifetime risk of prostate cancer death in an unscre
academic.oup.com
September 22, 2025 at 11:50 AM
Remarkable study from the Malmo Preventive Project: ~1000 men with blood at 60 in 1981; no PSA screening, *lifetime* follow-up. >50% life years lost to prostate cancer in PSA>4.0; 85% for PSA >2.0. Focus screening for men in 60s in men with higher PSAs! academic.oup.com/jnci/advance...
Now seen two papers claiming PLND not needed in a subgroup with relatively low incidence of positive nodes at radical prostatectomy. Neither cite the RCT showing benefit of PLND. When RCT says “do X”, don’t eyeball a case-series to conclude “don’t do X”.
September 15, 2025 at 4:26 PM
Now seen two papers claiming PLND not needed in a subgroup with relatively low incidence of positive nodes at radical prostatectomy. Neither cite the RCT showing benefit of PLND. When RCT says “do X”, don’t eyeball a case-series to conclude “don’t do X”.
This is big! Worked with great statisticians on guidelines for meta-analysis & systematic review. We discuss rationales for systematic review, evaluation & interpretation of heterogeneity, & common errors in network meta-analysis, funnel plots etc. www.europeanurology.com/article/S030...

Guidelines for Meta-analyses and Systematic Reviews in Urology
Our guideline comprises points addressing the conduct and interpretation of systematic
reviews and meta-analyses in urology. Application of the guideline would lead to a
more considered interpretation...
www.europeanurology.com
September 5, 2025 at 2:30 PM
This is big! Worked with great statisticians on guidelines for meta-analysis & systematic review. We discuss rationales for systematic review, evaluation & interpretation of heterogeneity, & common errors in network meta-analysis, funnel plots etc. www.europeanurology.com/article/S030...
Urologists do well with probability estimates vs. clinical scenarios. Goes against 25 years of me hearing "clinicians are too dumb to understand numbers, just tell them what to do". doi.org/10.1097/UPJ....

How Do Urologists Interpret Risk? Differences in Appropriateness of Active Surveillance Based on Clinical-Based vs Probability-Based Risk Assessments | Urology Practice
doi.org
September 3, 2025 at 2:45 PM
Urologists do well with probability estimates vs. clinical scenarios. Goes against 25 years of me hearing "clinicians are too dumb to understand numbers, just tell them what to do". doi.org/10.1097/UPJ....
Reposted by Andrew Vickers

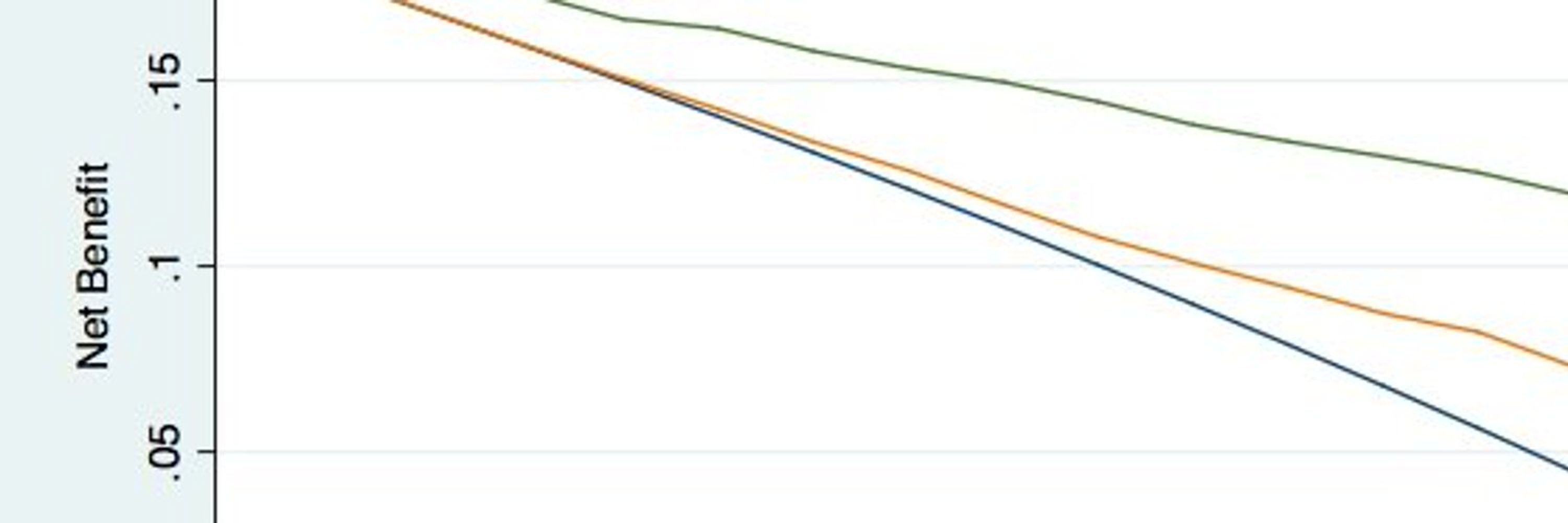
Thrilled to share our new @BJUIjournal study!
📊 Quantifying Gleason pattern 4 via MRI & targeted biopsy predicts prostate cancer metastasis better than standard Gleason grading & risk scores.
Precision matters in risk stratification.
🔗 doi.org/10.1111/bju.... @vickersbiostats.bsky.social
📊 Quantifying Gleason pattern 4 via MRI & targeted biopsy predicts prostate cancer metastasis better than standard Gleason grading & risk scores.
Precision matters in risk stratification.
🔗 doi.org/10.1111/bju.... @vickersbiostats.bsky.social

Quantification of prostate cancer Gleason pattern 4 to predict oncological outcome
Objectives To determine if quantifying Gleason pattern 4 (GP4) is superior to Grade Group (GG) in predicting any and distant metastatic recurrence after radical prostatectomy (RP) for prostate cance...
doi.org
August 27, 2025 at 8:49 PM
Thrilled to share our new @BJUIjournal study!
📊 Quantifying Gleason pattern 4 via MRI & targeted biopsy predicts prostate cancer metastasis better than standard Gleason grading & risk scores.
Precision matters in risk stratification.
🔗 doi.org/10.1111/bju.... @vickersbiostats.bsky.social
📊 Quantifying Gleason pattern 4 via MRI & targeted biopsy predicts prostate cancer metastasis better than standard Gleason grading & risk scores.
Precision matters in risk stratification.
🔗 doi.org/10.1111/bju.... @vickersbiostats.bsky.social
Reposted by Andrew Vickers

No.

5. You should use a precision-recall curve for a binary classifier, not an ROC curve
August 19, 2025 at 3:22 PM
No.
Folks discuss replication crisis as if something new. But remember Hans Eysenck (an OG scientific racist)? Both "Eysenck was the most frequently cited living psychologist" & "14 papers retracted, 60 statements of concern issued by journals"
en.wikipedia.org/wiki/Hans_Ey...
en.wikipedia.org/wiki/Hans_Ey...

Hans Eysenck - Wikipedia
en.wikipedia.org
August 12, 2025 at 7:33 PM
Folks discuss replication crisis as if something new. But remember Hans Eysenck (an OG scientific racist)? Both "Eysenck was the most frequently cited living psychologist" & "14 papers retracted, 60 statements of concern issued by journals"
en.wikipedia.org/wiki/Hans_Ey...
en.wikipedia.org/wiki/Hans_Ey...
No justification for arbitrary age cut-offs in clinical trials (e.g. excluding patients over 75) www.theguardian.com/society/2025...

Elderly people being excluded from medical research in UK, charities warn
The exclusion of older people from research due to arbitrary age cut-offs could stall the development of life-saving treatments
www.theguardian.com
August 10, 2025 at 12:56 PM
No justification for arbitrary age cut-offs in clinical trials (e.g. excluding patients over 75) www.theguardian.com/society/2025...
A comment on some invalid criticisms of the radical prostatectomy lymph node dissection trial www.sciencedirect.com/science/arti...

Reply to Matthew J. Roberts, Philip Cornford, Derya Tilki. Oncological Benefits of Extended Pelvic Lymph Node Dissection: More Fog or Clarity to the Debate? Eur Urol 2025;87:261–3
www.sciencedirect.com
July 28, 2025 at 12:14 PM
A comment on some invalid criticisms of the radical prostatectomy lymph node dissection trial www.sciencedirect.com/science/arti...
The Gleason score - the fundamental determinant of how we chose on treatments in localized prostate cancers - basically doesn't make any sense. grandroundsinurology.com/away-from-th...
Away from the Gleason Score and Towards Quantification of Pattern 4 for Treatment Decision Making in Localized Prostate Cancer
Andrew Vickers, PhD, discusses the need for reforming the Gleason score, the cornerstone of decision-making in prostate cancer management.
grandroundsinurology.com
July 23, 2025 at 8:54 PM
The Gleason score - the fundamental determinant of how we chose on treatments in localized prostate cancers - basically doesn't make any sense. grandroundsinurology.com/away-from-th...
I keep hearing "AI models have to be explainable otherwise doctors and patients won't trust them". But if I Google "does explainability improve trust in AI?", I get an AI summary (short answer "yes") created by an AI process that probably <1% of the population understands.
July 21, 2025 at 1:46 PM
I keep hearing "AI models have to be explainable otherwise doctors and patients won't trust them". But if I Google "does explainability improve trust in AI?", I get an AI summary (short answer "yes") created by an AI process that probably <1% of the population understands.
Results of observational study almost perfectly match those of our RCT. Hazard ratios of 1.07 / 0.72 for BCR / mets; RCT reported 1.05 / 0.82. Conclusions: do extended PLND during radical prostatectomy; effects of PLND occur after BCR. www.auajournals.org/doi/pdf/10.1...
July 14, 2025 at 6:39 PM
Results of observational study almost perfectly match those of our RCT. Hazard ratios of 1.07 / 0.72 for BCR / mets; RCT reported 1.05 / 0.82. Conclusions: do extended PLND during radical prostatectomy; effects of PLND occur after BCR. www.auajournals.org/doi/pdf/10.1...
Reposted by Andrew Vickers

You can have all the omni-omics data in the world and the bestest algorithms, but eventually a predicted probability is produced & it should be evaluated using well-established methods, and correctly implemented in the context of medical decision making.
statsepi.substack.com/i/140315566/...
statsepi.substack.com/i/140315566/...
July 14, 2025 at 9:49 AM
You can have all the omni-omics data in the world and the bestest algorithms, but eventually a predicted probability is produced & it should be evaluated using well-established methods, and correctly implemented in the context of medical decision making.
statsepi.substack.com/i/140315566/...
statsepi.substack.com/i/140315566/...