


Sean Ong
@seanong.bsky.social
ID doc and joint PhD candidate at University of Toronto + University of Melbourne. Talk to me about clinical trial design and methodology, bloodstream infections, S. aureus, and Gram negatives 🦠
🇸🇬🇨🇦🇦🇺
🇸🇬🇨🇦🇦🇺
High-income countries fund a large majority of clinical trials in ID, with the NIH in particular funding 20% of trials in our review. Current changes in funding (especially the de-prioritisation of global health amongst some funders) has major implications on ID clinical trials worldwide.

September 29, 2025 at 8:57 AM
High-income countries fund a large majority of clinical trials in ID, with the NIH in particular funding 20% of trials in our review. Current changes in funding (especially the de-prioritisation of global health amongst some funders) has major implications on ID clinical trials worldwide.
Our new paper in @cmijournal.bsky.social led by the brilliant Hadrien Moffroid, a junior colleague in Melbourne. We examined international funding flows in ID RCTs published in selected high-impact journals over a 10-year period.
doi.org/10.1016/j.cm...
@steventong.bsky.social #IDSky
doi.org/10.1016/j.cm...
@steventong.bsky.social #IDSky

September 29, 2025 at 8:57 AM
Our new paper in @cmijournal.bsky.social led by the brilliant Hadrien Moffroid, a junior colleague in Melbourne. We examined international funding flows in ID RCTs published in selected high-impact journals over a 10-year period.
doi.org/10.1016/j.cm...
@steventong.bsky.social #IDSky
doi.org/10.1016/j.cm...
@steventong.bsky.social #IDSky
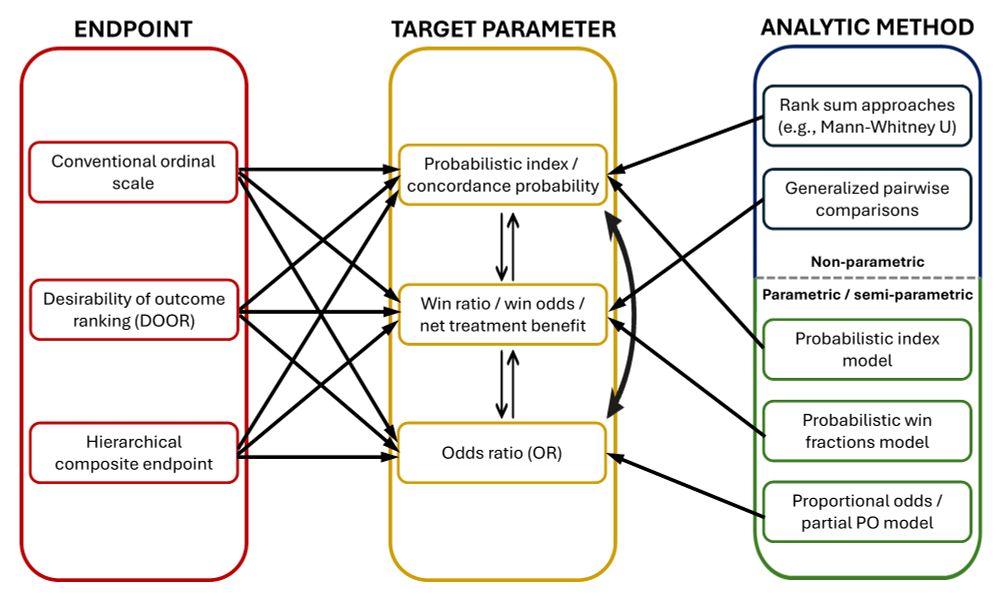
7/ The nomenclature in the literature is inconsistent, and often mixes up outcomes, target parameters, and analytic methods. Confusingly, outcomes can be summarized using multiple different target parameters, which can be analyzed using multiple different methods. More than one way to skin a cat :)
June 16, 2025 at 1:55 AM
7/ The nomenclature in the literature is inconsistent, and often mixes up outcomes, target parameters, and analytic methods. Confusingly, outcomes can be summarized using multiple different target parameters, which can be analyzed using multiple different methods. More than one way to skin a cat :)
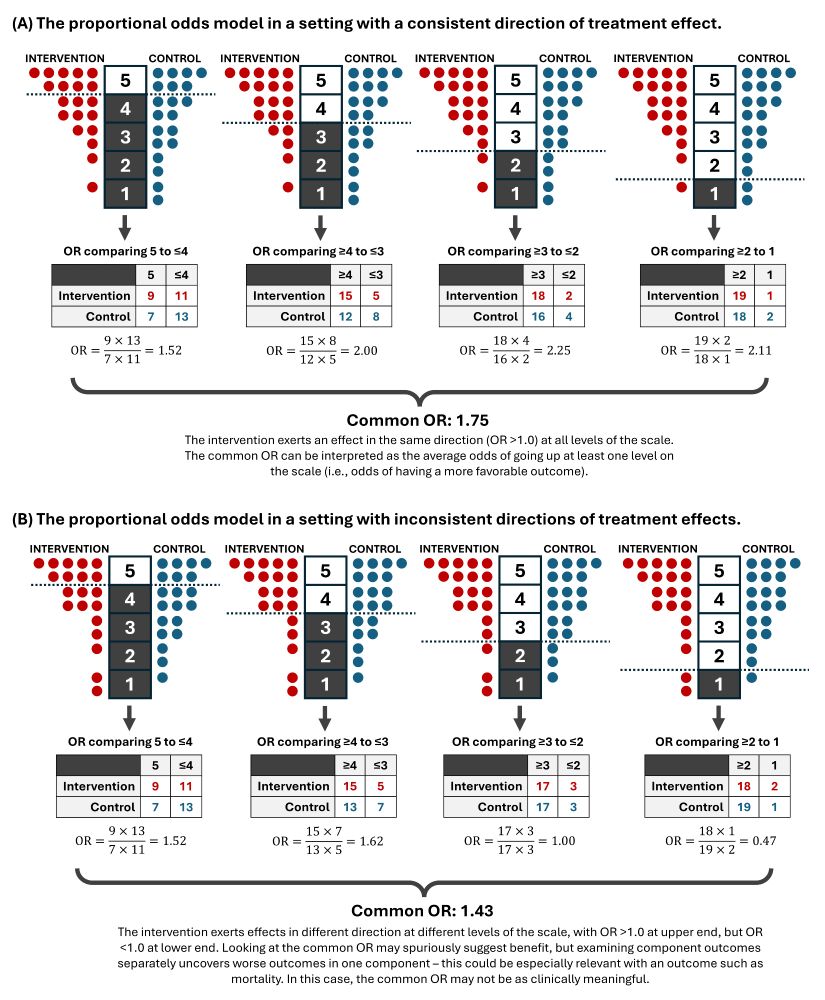
6/ Importantly, we should look at whether odds are proportional (known as the PO assumption), or minimally that the direction of effect is consistent across all levels of the ordinal scale. As long as the effect is consistent (as opposed to discordant), the common OR is clinically interpretable.
June 16, 2025 at 1:55 AM
6/ Importantly, we should look at whether odds are proportional (known as the PO assumption), or minimally that the direction of effect is consistent across all levels of the ordinal scale. As long as the effect is consistent (as opposed to discordant), the common OR is clinically interpretable.
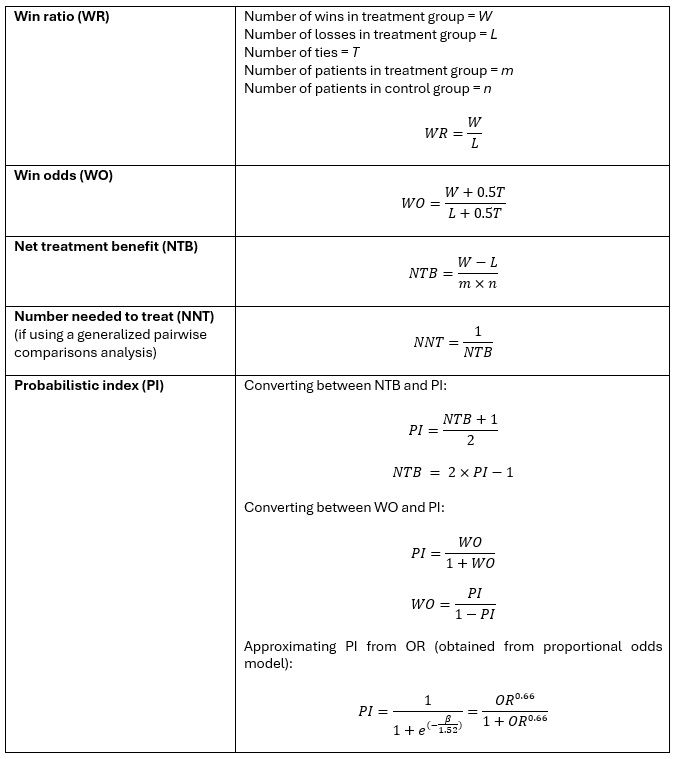
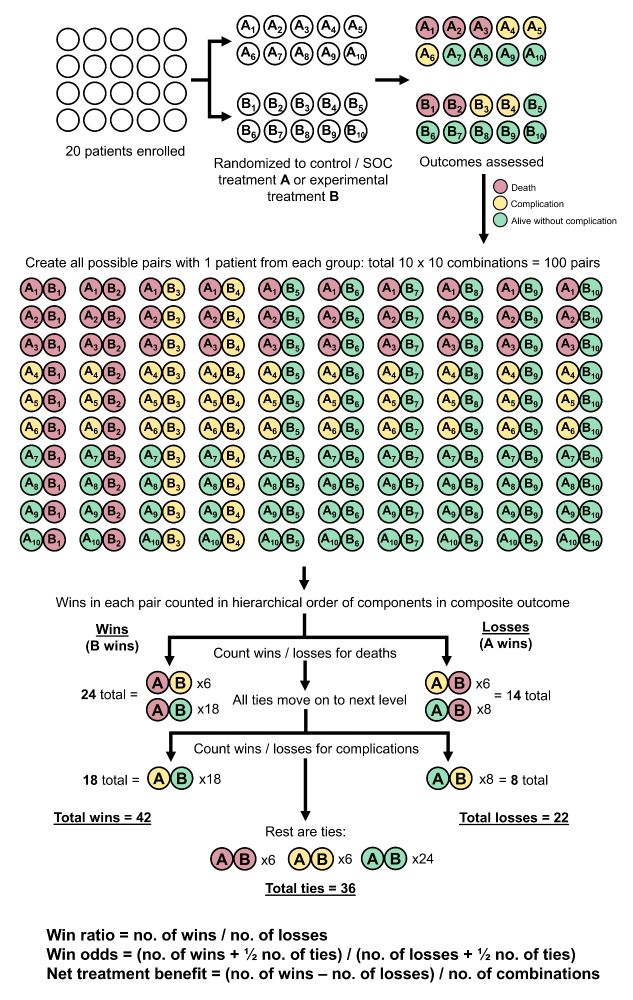
4/ This results in three summary numbers: total number of wins, losses, and ties. These numbers can be used to calculate different treatment effect estimates: win ratio, win odds, net treatment benefit, NNT, and probabilistic index. (Don't let the math scare you, it's simpler than it looks!)
June 16, 2025 at 1:55 AM
4/ This results in three summary numbers: total number of wins, losses, and ties. These numbers can be used to calculate different treatment effect estimates: win ratio, win odds, net treatment benefit, NNT, and probabilistic index. (Don't let the math scare you, it's simpler than it looks!)
3/ HCEs can also be analyzed using the generalized pairwise comparisons (GPC) method, where every patient in group 1 is compared to every patient in group 2 in all possible patient-pair combinations. A win is determined for each pair based on the hierarchical ordering of outcome components.
June 16, 2025 at 1:55 AM
3/ HCEs can also be analyzed using the generalized pairwise comparisons (GPC) method, where every patient in group 1 is compared to every patient in group 2 in all possible patient-pair combinations. A win is determined for each pair based on the hierarchical ordering of outcome components.
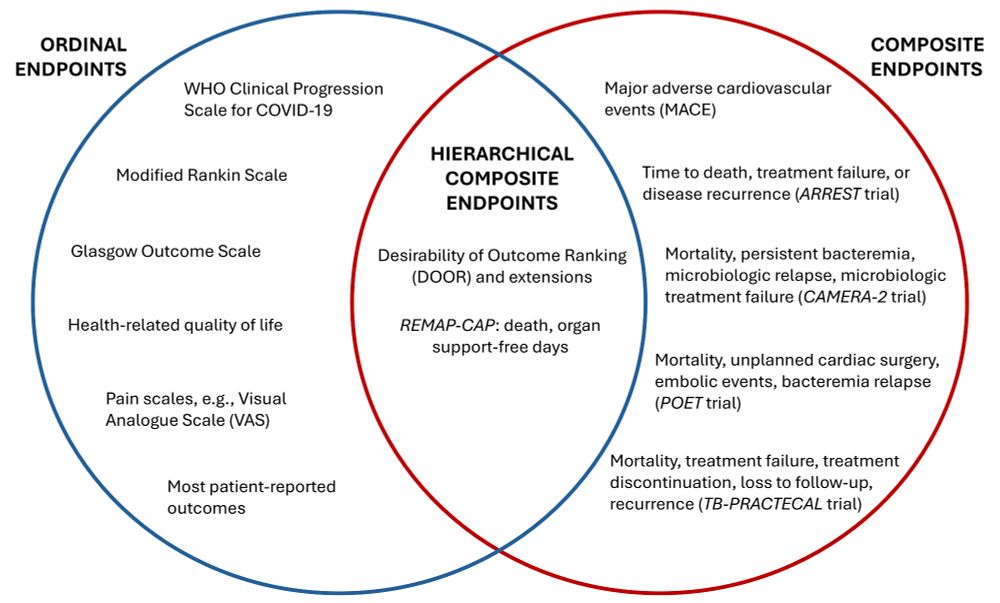
1/ HCEs combine features of composite and ordinal outcomes: they combine multiple clinical events (composite), but are also hierarchical as they establish a rank order of clinical importance across the different component events. A common example in ID is the DOOR outcome, a specific type of HCE.
June 16, 2025 at 1:55 AM
1/ HCEs combine features of composite and ordinal outcomes: they combine multiple clinical events (composite), but are also hierarchical as they establish a rank order of clinical importance across the different component events. A common example in ID is the DOOR outcome, a specific type of HCE.
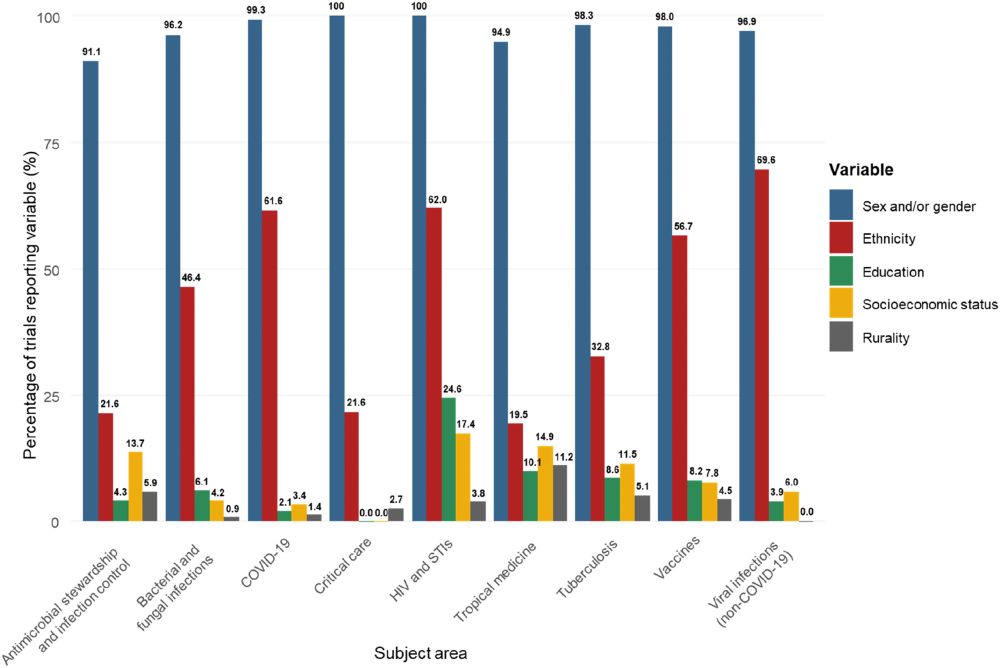
6/ Reporting of these variables also differed widely depending on subject area. E.g., RCTs studying viral infections, HIV/STIs, and COVID-19 had the highest reporting of ethnicity, while those studying tropical medicine, critical care, and antimicrobial stewardship/infection control had the lowest.
May 7, 2025 at 12:55 AM
6/ Reporting of these variables also differed widely depending on subject area. E.g., RCTs studying viral infections, HIV/STIs, and COVID-19 had the highest reporting of ethnicity, while those studying tropical medicine, critical care, and antimicrobial stewardship/infection control had the lowest.
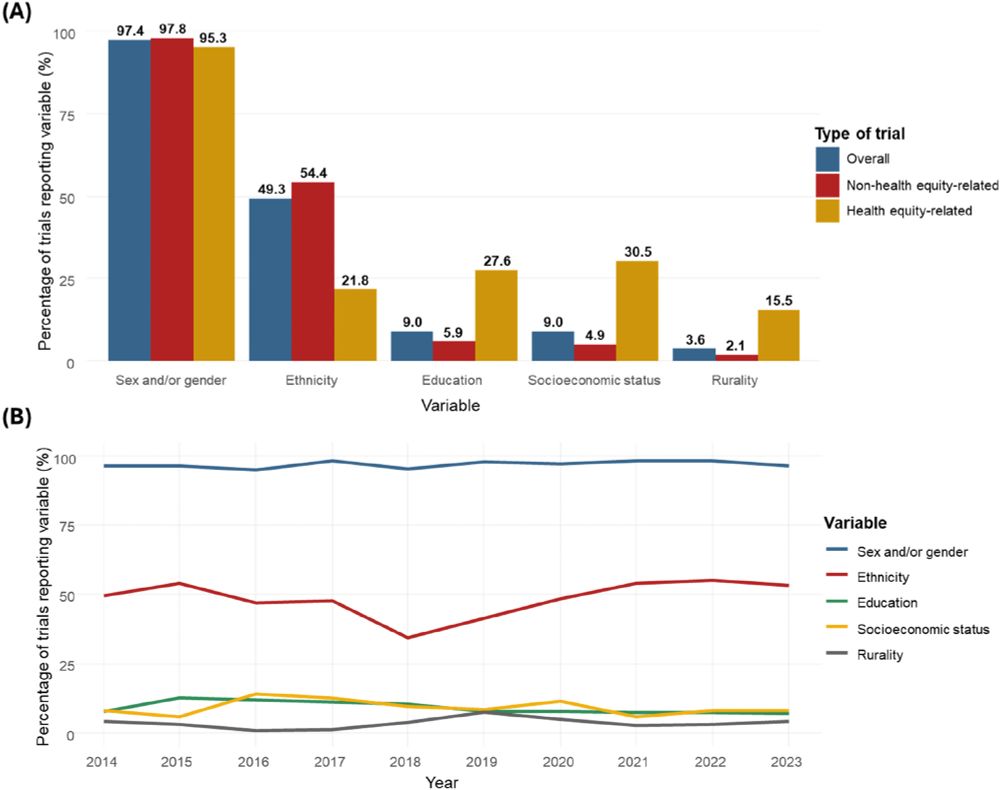
5/ Almost all trials reported sex and/or gender. However, less than half (49.3%) reported ethnicity, and only a minority reported education level (9.0%), socioeconomic status (9.0%), and rurality (3.9%). Reporting of all these variables did not improve throughout the 10-year study period.
May 7, 2025 at 12:55 AM
5/ Almost all trials reported sex and/or gender. However, less than half (49.3%) reported ethnicity, and only a minority reported education level (9.0%), socioeconomic status (9.0%), and rurality (3.9%). Reporting of all these variables did not improve throughout the 10-year study period.
Looking forward to another packed day at #ESCMIDGlobal. Come say hi at 12:00 at Poster 0737 (Sector A/6/5) where I will be presenting our experience with the vanguard phase of the BALANCE+ Platform, our new platform trial for Gram-negative BSI. Open to new collaborators and sites to join!

April 13, 2025 at 6:14 AM
Looking forward to another packed day at #ESCMIDGlobal. Come say hi at 12:00 at Poster 0737 (Sector A/6/5) where I will be presenting our experience with the vanguard phase of the BALANCE+ Platform, our new platform trial for Gram-negative BSI. Open to new collaborators and sites to join!
@steventong.bsky.social and @gurujosh.bsky.social presenting an overview of the SNAP trial and results of the PSSA & MSSA antibiotic backbone domains, at #ESCMIDGlobal. Exciting stuff!!

April 12, 2025 at 2:31 PM
@steventong.bsky.social and @gurujosh.bsky.social presenting an overview of the SNAP trial and results of the PSSA & MSSA antibiotic backbone domains, at #ESCMIDGlobal. Exciting stuff!!
9/ However, there was no significant heterogeneity of treatment effect identified using any of the three risk scores, i.e., there was no difference between 7-day vs 14-day treatment, even amongst the higher risk groups.

April 10, 2025 at 9:36 AM
9/ However, there was no significant heterogeneity of treatment effect identified using any of the three risk scores, i.e., there was no difference between 7-day vs 14-day treatment, even amongst the higher risk groups.
8/ In the BALANCE cohort, all three decision rules could predict the outcome of 90-day mortality well, i.e., the combination of variables used in each risk score could reliably classify patients into different risk groups with different risks of experiencing the primary outcome.

April 10, 2025 at 9:36 AM
8/ In the BALANCE cohort, all three decision rules could predict the outcome of 90-day mortality well, i.e., the combination of variables used in each risk score could reliably classify patients into different risk groups with different risks of experiencing the primary outcome.
6/ We formulated two rules based on results of a survey of BALANCE investigators querying them on variables they consider important in deciding antibiotic duration. We constructed these as a static decision rule (to be applied on day 4), and a dynamic stopping rule (to be assessed daily).

April 10, 2025 at 9:36 AM
6/ We formulated two rules based on results of a survey of BALANCE investigators querying them on variables they consider important in deciding antibiotic duration. We constructed these as a static decision rule (to be applied on day 4), and a dynamic stopping rule (to be assessed daily).
5/ In this paper, we applied the risk-modelling approach to identify HTE. In this approach, we develop or identify risk scores that are predictive of the outcome, classify the trial population to different risk groups using these scores, then determine if there is a treatment effect difference.

April 10, 2025 at 9:36 AM
5/ In this paper, we applied the risk-modelling approach to identify HTE. In this approach, we develop or identify risk scores that are predictive of the outcome, classify the trial population to different risk groups using these scores, then determine if there is a treatment effect difference.
4/ Even if subgroup analyses find no effect in single variables such as severity, comorbidity, and pathogen characteristics — what does this mean for my patient who may have multiple high-risk features? Clinicians must consider a combination of clinical variables when making treatment decisions.

April 10, 2025 at 9:36 AM
4/ Even if subgroup analyses find no effect in single variables such as severity, comorbidity, and pathogen characteristics — what does this mean for my patient who may have multiple high-risk features? Clinicians must consider a combination of clinical variables when making treatment decisions.
3/ The conventional approach to identifying HTE is single variable subgroup analysis — and none of these identified a significant subgroup interaction effect in the primary BALANCE analysis. However, single variable subgroup analyses translate poorly to clinical decision making at the bedside.

April 10, 2025 at 9:36 AM
3/ The conventional approach to identifying HTE is single variable subgroup analysis — and none of these identified a significant subgroup interaction effect in the primary BALANCE analysis. However, single variable subgroup analyses translate poorly to clinical decision making at the bedside.
2/ Clinical trials estimate average treatment effects across the entire trial population. However, there may be heterogeneity of treatment effect — a finding of no difference could be seen when there are subgroups who benefit and are harmed from treatment, but whose effects cancel each other out.

April 10, 2025 at 9:36 AM
2/ Clinical trials estimate average treatment effects across the entire trial population. However, there may be heterogeneity of treatment effect — a finding of no difference could be seen when there are subgroups who benefit and are harmed from treatment, but whose effects cancel each other out.
9/ However, there was no significant heterogeneity of treatment effect identified using any of the three risk scores, i.e., there was no difference between 7-day vs 14-day treatment, even amongst the higher risk groups.

April 10, 2025 at 9:25 AM
9/ However, there was no significant heterogeneity of treatment effect identified using any of the three risk scores, i.e., there was no difference between 7-day vs 14-day treatment, even amongst the higher risk groups.
8/ In the BALANCE cohort, all three decision rules could predict the outcome of 90-day mortality well, i.e., the combination of variables used in each risk score could reliably classify patients into different risk groups with different risks of experiencing the primary outcome.

April 10, 2025 at 9:25 AM
8/ In the BALANCE cohort, all three decision rules could predict the outcome of 90-day mortality well, i.e., the combination of variables used in each risk score could reliably classify patients into different risk groups with different risks of experiencing the primary outcome.
6/ We formulated two rules based on results of a survey of BALANCE investigators querying them on variables they consider important in deciding antibiotic duration. We constructed these as a static decision rule (to be applied on day 4), and a dynamic stopping rule (to be assessed daily).

April 10, 2025 at 9:25 AM
6/ We formulated two rules based on results of a survey of BALANCE investigators querying them on variables they consider important in deciding antibiotic duration. We constructed these as a static decision rule (to be applied on day 4), and a dynamic stopping rule (to be assessed daily).
5/ In this paper, we applied the risk-modelling approach to identify HTE. In this approach, we develop or identify risk scores that are predictive of the outcome, classify the trial population to different risk groups using these scores, then determine if there is a treatment effect difference.

April 10, 2025 at 9:25 AM
5/ In this paper, we applied the risk-modelling approach to identify HTE. In this approach, we develop or identify risk scores that are predictive of the outcome, classify the trial population to different risk groups using these scores, then determine if there is a treatment effect difference.
4/ Even if subgroup analyses find no effect in single variables such as severity, comorbidity, and pathogen characteristics — what does this mean for my patient who may have multiple high-risk features? Clinicians must consider a combination of clinical variables when making treatment decisions.

April 10, 2025 at 9:25 AM
4/ Even if subgroup analyses find no effect in single variables such as severity, comorbidity, and pathogen characteristics — what does this mean for my patient who may have multiple high-risk features? Clinicians must consider a combination of clinical variables when making treatment decisions.
3/ The conventional approach to identifying HTE is single variable subgroup analysis — and none of these identified a significant subgroup interaction effect in the primary BALANCE analysis. However, single variable subgroup analyses translate poorly to clinical decision making at the bedside.
April 10, 2025 at 9:25 AM
3/ The conventional approach to identifying HTE is single variable subgroup analysis — and none of these identified a significant subgroup interaction effect in the primary BALANCE analysis. However, single variable subgroup analyses translate poorly to clinical decision making at the bedside.
2/ Clinical trials estimate average treatment effects across the entire trial population. However, there may be heterogeneity of treatment effect — a finding of no difference could be seen when there are subgroups who benefit and are harmed from treatment, but whose effects cancel each other out.

April 10, 2025 at 9:25 AM
2/ Clinical trials estimate average treatment effects across the entire trial population. However, there may be heterogeneity of treatment effect — a finding of no difference could be seen when there are subgroups who benefit and are harmed from treatment, but whose effects cancel each other out.