



Madeleine Kline
@mckline98.bsky.social
MD/PhD student at HMS/HSPH infectious disease epidemiology, musician, climate advocate, runner, lover of baked goods and cute animals
Your point about higher starting prevalence settings is also excellent — and an area of ongoing work in the lab!
July 18, 2025 at 7:45 PM
Your point about higher starting prevalence settings is also excellent — and an area of ongoing work in the lab!
However, this would effectively mean there is a higher “resistance emergence” probability to those drugs, which we did test in our sensitivity analysis. Our framework could be easily adapted to more specifically look at bystander selection via something like an importation rate parameter.
July 18, 2025 at 7:45 PM
However, this would effectively mean there is a higher “resistance emergence” probability to those drugs, which we did test in our sensitivity analysis. Our framework could be easily adapted to more specifically look at bystander selection via something like an importation rate parameter.
Thanks so much! It’s true that bystander selection through antibiotic usage for non-gonorrhea infections could occur (especially for ceftriaxone and gepotidacin), and this is not explicitly modeled here.
July 18, 2025 at 7:45 PM
Thanks so much! It’s true that bystander selection through antibiotic usage for non-gonorrhea infections could occur (especially for ceftriaxone and gepotidacin), and this is not explicitly modeled here.
Our results indicate that distributing selective pressures across the population minimizes the emergence of drug resistance in gonorrhea in US MSM and underscore the importance of disease and context-specific decision-making. [10/10]
July 3, 2025 at 3:29 PM
Our results indicate that distributing selective pressures across the population minimizes the emergence of drug resistance in gonorrhea in US MSM and underscore the importance of disease and context-specific decision-making. [10/10]
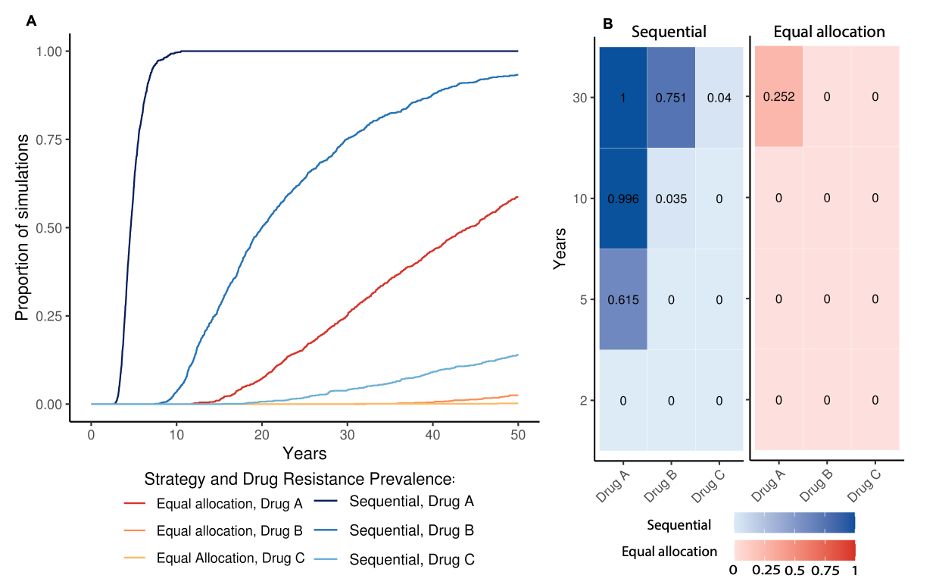
It was possible to find combinations of parameters where equal allocation was worse than sequential, but these were rare edge cases that required a combination of unlikely events. Even then, the difference between strategies was not large [9/10]
July 3, 2025 at 3:29 PM
It was possible to find combinations of parameters where equal allocation was worse than sequential, but these were rare edge cases that required a combination of unlikely events. Even then, the difference between strategies was not large [9/10]
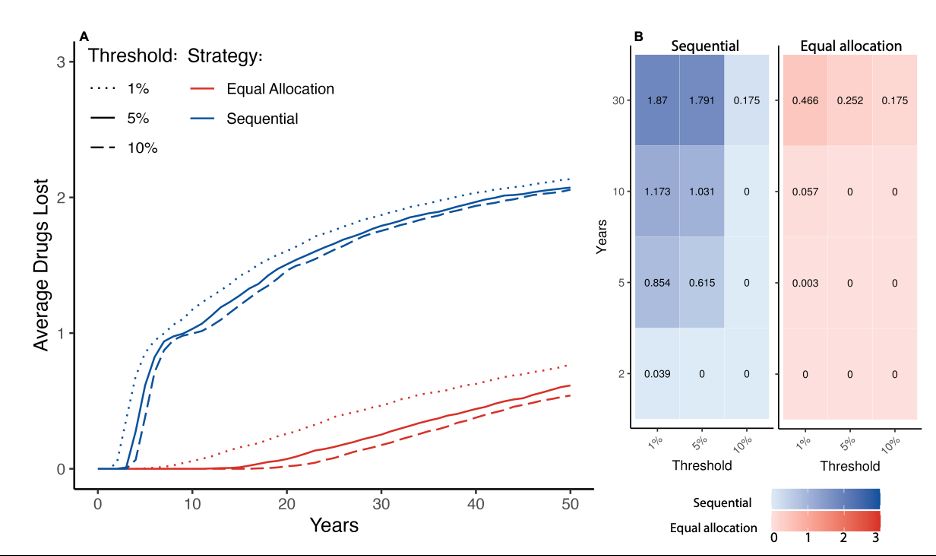
Equal allocation was still better when we changed the prevalence threshold from 5% to 1% or 10%, and across a wide range of parameter values for parameters that determine underlying model behavior [8/10]
July 3, 2025 at 3:29 PM
Equal allocation was still better when we changed the prevalence threshold from 5% to 1% or 10%, and across a wide range of parameter values for parameters that determine underlying model behavior [8/10]
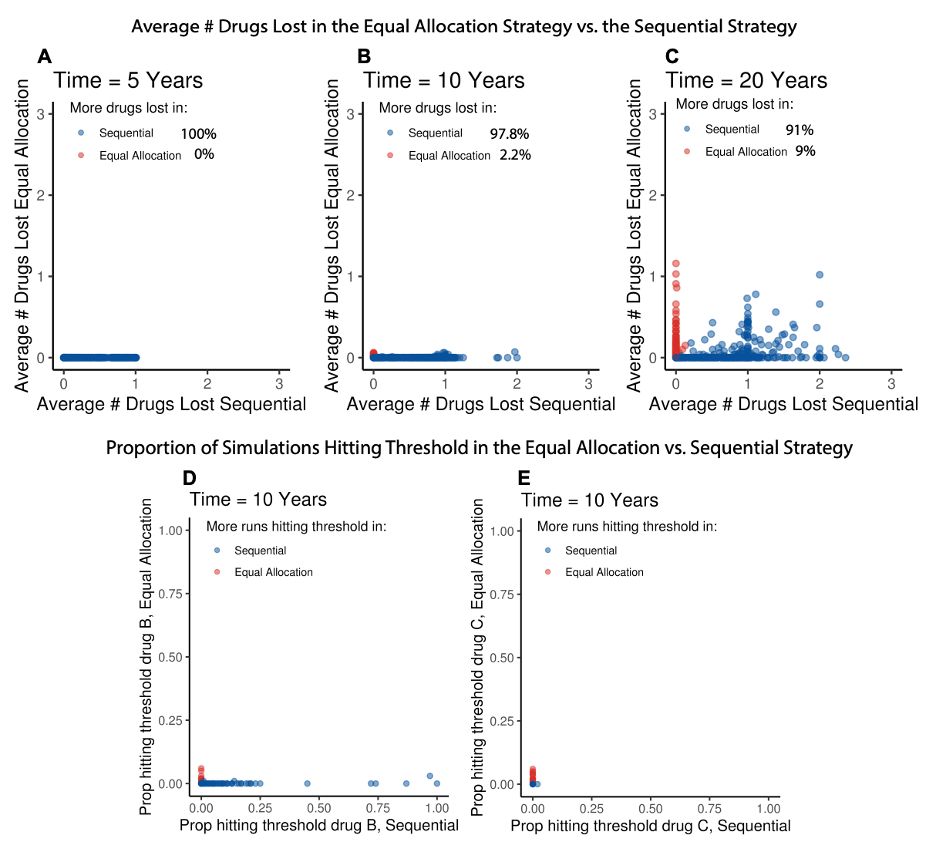
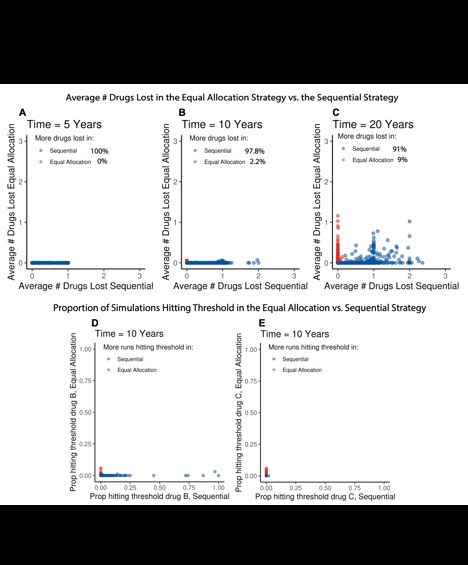
The sequential strategy had met the 5% resistance prevalence threshold i) for each drug individually and ii) for all 3 drugs in at least as many simulations and iii) for at least as many drugs on average compared to the equal allocation strategy [7/10]
July 3, 2025 at 3:29 PM
The sequential strategy had met the 5% resistance prevalence threshold i) for each drug individually and ii) for all 3 drugs in at least as many simulations and iii) for at least as many drugs on average compared to the equal allocation strategy [7/10]
We looked at the proportion of simulations had reached 5% prevalence of resistance for each drug and found that the equal allocation strategy 🔴 was better than the sequential strategy 🔵 because: [6/10]
July 3, 2025 at 3:29 PM
We looked at the proportion of simulations had reached 5% prevalence of resistance for each drug and found that the equal allocation strategy 🔴 was better than the sequential strategy 🔵 because: [6/10]
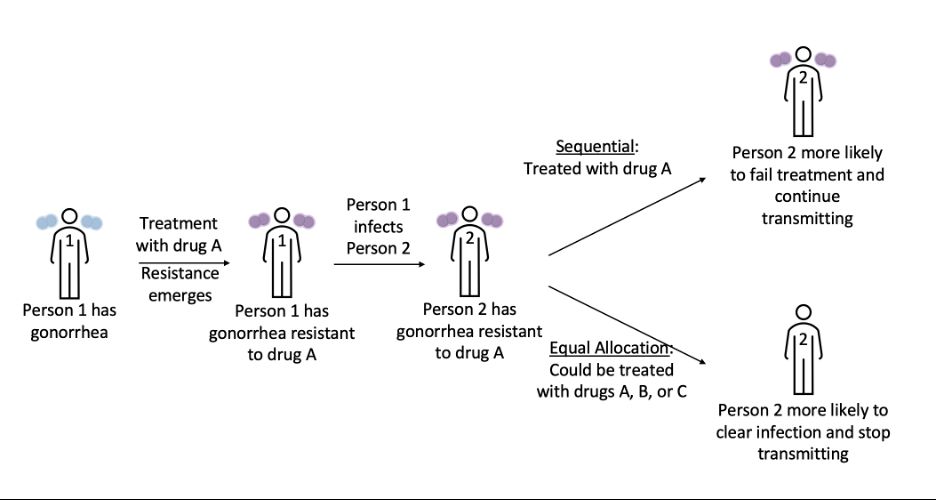
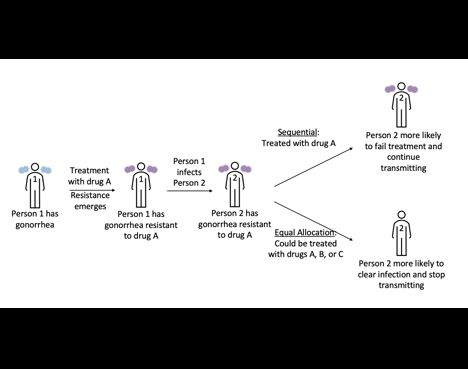
We compared two strategies: equal allocation 🔴, where all 3 drugs are used in random allocation but each individual gets treated with 1 drug, and sequential 🔵, where new drugs are only used once resistance prevalence for the previous drug has reached 5% [5/10]
July 3, 2025 at 3:29 PM
We compared two strategies: equal allocation 🔴, where all 3 drugs are used in random allocation but each individual gets treated with 1 drug, and sequential 🔵, where new drugs are only used once resistance prevalence for the previous drug has reached 5% [5/10]
Here, we used a stochastic compartmental gonorrhea transmission model of US MSM to test introduction strategies with two new available drugs and one currently used drug, aimed at capturing random emergence and extinction dynamics [4/10]
July 3, 2025 at 3:29 PM
Here, we used a stochastic compartmental gonorrhea transmission model of US MSM to test introduction strategies with two new available drugs and one currently used drug, aimed at capturing random emergence and extinction dynamics [4/10]
Antibiotic stewardship often urges us to reserve new antibiotics until they are absolutely needed, especially in hospital settings. Past research has shown that for gonorrhea treatment, distributing selective pressures by offering more treatment options at the same time reduces drug resistance[3/10]
July 3, 2025 at 3:29 PM
Antibiotic stewardship often urges us to reserve new antibiotics until they are absolutely needed, especially in hospital settings. Past research has shown that for gonorrhea treatment, distributing selective pressures by offering more treatment options at the same time reduces drug resistance[3/10]
There were > half a million notifications for gonorrhea in the US in 2023, and the bacteria that cause the infection have developed resistance to all antibiotics used to treat it. 2 new drugs, zoliflodacin and gepotidacin, had positive phase III trial results and will likely be approved soon [2/10]
July 3, 2025 at 3:29 PM
There were > half a million notifications for gonorrhea in the US in 2023, and the bacteria that cause the infection have developed resistance to all antibiotics used to treat it. 2 new drugs, zoliflodacin and gepotidacin, had positive phase III trial results and will likely be approved soon [2/10]
Our results indicate that distributing selective pressures across the population minimizes the emergence of drug resistance in gonorrhea in US MSM and underscore the importance of disease and context-specific decision-making. [10/10]
July 3, 2025 at 3:19 PM
Our results indicate that distributing selective pressures across the population minimizes the emergence of drug resistance in gonorrhea in US MSM and underscore the importance of disease and context-specific decision-making. [10/10]
It was possible to find combinations of parameters where equal allocation was worse than sequential, but these were rare edge cases that required a combination of unlikely events. Even then, the difference between strategies was not large [9/10]
July 3, 2025 at 3:19 PM
It was possible to find combinations of parameters where equal allocation was worse than sequential, but these were rare edge cases that required a combination of unlikely events. Even then, the difference between strategies was not large [9/10]
We looked at the proportion of simulations had reached 5% prevalence of resistance for each drug and found that the equal allocation strategy 🔴 was better than the sequential strategy 🔵 because: [6/10]
July 3, 2025 at 3:19 PM
We looked at the proportion of simulations had reached 5% prevalence of resistance for each drug and found that the equal allocation strategy 🔴 was better than the sequential strategy 🔵 because: [6/10]
We compared two strategies: equal allocation 🔴, where all 3 drugs are used in random allocation but each individual gets treated with 1 drug, and sequential 🔵, where new drugs are only used once resistance prevalence for the previous drug has reached 5% [5/10]
July 3, 2025 at 3:19 PM
We compared two strategies: equal allocation 🔴, where all 3 drugs are used in random allocation but each individual gets treated with 1 drug, and sequential 🔵, where new drugs are only used once resistance prevalence for the previous drug has reached 5% [5/10]
Here, we used a stochastic compartmental gonorrhea transmission model of US MSM to test introduction strategies with two new available drugs and one currently used drug, aimed at capturing random emergence and extinction dynamics [4/10]
July 3, 2025 at 3:19 PM
Here, we used a stochastic compartmental gonorrhea transmission model of US MSM to test introduction strategies with two new available drugs and one currently used drug, aimed at capturing random emergence and extinction dynamics [4/10]
Antibiotic stewardship often urges us to reserve new antibiotics until they are absolutely needed, especially in hospital settings. Past research has shown that for gonorrhea treatment, distributing selective pressures by offering more treatment options at the same time reduces drug resistance[3/10]
July 3, 2025 at 3:19 PM
Antibiotic stewardship often urges us to reserve new antibiotics until they are absolutely needed, especially in hospital settings. Past research has shown that for gonorrhea treatment, distributing selective pressures by offering more treatment options at the same time reduces drug resistance[3/10]
There were over 1/2 a million notifications for gonorrhea in the US in 2023, and the bacteria that cause the infection have developed resistance to all antibiotics used to treat it. 2 new drugs, zoliflodacin and gepotidacin, had positive phase III trial results and will likely be approved soon[2/10]
July 3, 2025 at 3:19 PM
There were over 1/2 a million notifications for gonorrhea in the US in 2023, and the bacteria that cause the infection have developed resistance to all antibiotics used to treat it. 2 new drugs, zoliflodacin and gepotidacin, had positive phase III trial results and will likely be approved soon[2/10]
Reposted by Madeleine Kline

I'm a current Harvard graduate student and I found out today that I had my NSF GRFP terminated without notification. I was awarded this individual research fellowship before even choosing Harvard as my graduate school
May 22, 2025 at 9:38 PM
I'm a current Harvard graduate student and I found out today that I had my NSF GRFP terminated without notification. I was awarded this individual research fellowship before even choosing Harvard as my graduate school