




Katie Wiskar
@katiewiskar.bsky.social
Academic General Internist 👩🏼⚕️ | GIM #POCUS fellowship lead www.ubcimpocus.com 🩺| SonoNerd 🤓| Obsessed with volume status 💦| #MedSky #POCUSky 🦋| Boy mom ❤️

March 27, 2025 at 3:45 PM
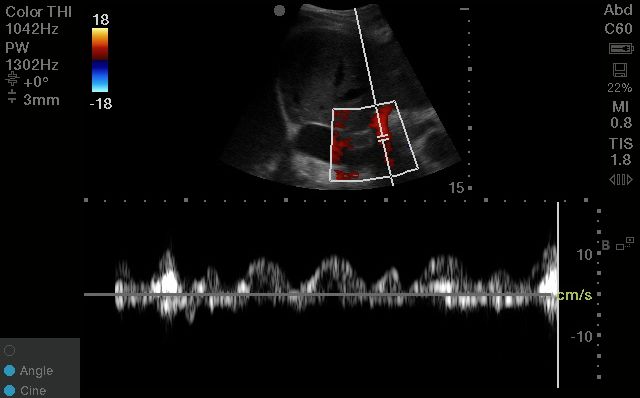
2. It's the easiest to interpret
Unlike the hepatic vein, which can be misleading in the absence of EKG gating, the portal vein is easily interpreted
You can use calipers to measure pulsatility fraction; but you can also use the eyeball method to assess mild vs moderate vs severe pulsatility.
Unlike the hepatic vein, which can be misleading in the absence of EKG gating, the portal vein is easily interpreted
You can use calipers to measure pulsatility fraction; but you can also use the eyeball method to assess mild vs moderate vs severe pulsatility.
February 25, 2025 at 6:30 PM
2. It's the easiest to interpret
Unlike the hepatic vein, which can be misleading in the absence of EKG gating, the portal vein is easily interpreted
You can use calipers to measure pulsatility fraction; but you can also use the eyeball method to assess mild vs moderate vs severe pulsatility.
Unlike the hepatic vein, which can be misleading in the absence of EKG gating, the portal vein is easily interpreted
You can use calipers to measure pulsatility fraction; but you can also use the eyeball method to assess mild vs moderate vs severe pulsatility.
You should see a nice vertically-aligned segment of the portal vein pop into view; easily recognized by its bright hyperechoic borders and hepatopetal blood flow (which will look RED on colour doppler).
February 25, 2025 at 6:30 PM
You should see a nice vertically-aligned segment of the portal vein pop into view; easily recognized by its bright hyperechoic borders and hepatopetal blood flow (which will look RED on colour doppler).
We've all been there: a Saturday on call in the hospital, with a list of 30 patients to round on 😵💫
Ward rounding can seem like an endless task - but it doesn't have to be! ⏰
Here are my top 10 tips for ward rounding efficiency 🧵-
#emimcc
Ward rounding can seem like an endless task - but it doesn't have to be! ⏰
Here are my top 10 tips for ward rounding efficiency 🧵-
#emimcc

February 14, 2025 at 4:32 PM
We've all been there: a Saturday on call in the hospital, with a list of 30 patients to round on 😵💫
Ward rounding can seem like an endless task - but it doesn't have to be! ⏰
Here are my top 10 tips for ward rounding efficiency 🧵-
#emimcc
Ward rounding can seem like an endless task - but it doesn't have to be! ⏰
Here are my top 10 tips for ward rounding efficiency 🧵-
#emimcc
11/
Of course - it goes without saying! - that all of these ultrasound findings should be incorporated with the rest of the clinical picture to help you reach a decision 🩺
Of course - it goes without saying! - that all of these ultrasound findings should be incorporated with the rest of the clinical picture to help you reach a decision 🩺

February 6, 2025 at 6:33 PM
11/
Of course - it goes without saying! - that all of these ultrasound findings should be incorporated with the rest of the clinical picture to help you reach a decision 🩺
Of course - it goes without saying! - that all of these ultrasound findings should be incorporated with the rest of the clinical picture to help you reach a decision 🩺
10/
Finally, we can look at other associated pathology.
In HF, we will often see other features such as bilateral simple pleural effusions; plus supportive cardiac findings.
In inflammatory/infectious causes, you may see unilateral consolidations, dynamic air bronchograms, shred signs, etc.
Finally, we can look at other associated pathology.
In HF, we will often see other features such as bilateral simple pleural effusions; plus supportive cardiac findings.
In inflammatory/infectious causes, you may see unilateral consolidations, dynamic air bronchograms, shred signs, etc.
February 6, 2025 at 6:33 PM
10/
Finally, we can look at other associated pathology.
In HF, we will often see other features such as bilateral simple pleural effusions; plus supportive cardiac findings.
In inflammatory/infectious causes, you may see unilateral consolidations, dynamic air bronchograms, shred signs, etc.
Finally, we can look at other associated pathology.
In HF, we will often see other features such as bilateral simple pleural effusions; plus supportive cardiac findings.
In inflammatory/infectious causes, you may see unilateral consolidations, dynamic air bronchograms, shred signs, etc.
9/
B lines arising from pulmonary edema should be bilateral, symmetrical, and in a dependent gradient (ie. most prominent at the bases).
B lines from infectious/inflammatory pathologies, on the other hand, are often asymmetrical, non-gravitational, and may display skipped or spared areas.
B lines arising from pulmonary edema should be bilateral, symmetrical, and in a dependent gradient (ie. most prominent at the bases).
B lines from infectious/inflammatory pathologies, on the other hand, are often asymmetrical, non-gravitational, and may display skipped or spared areas.
February 6, 2025 at 6:33 PM
9/
B lines arising from pulmonary edema should be bilateral, symmetrical, and in a dependent gradient (ie. most prominent at the bases).
B lines from infectious/inflammatory pathologies, on the other hand, are often asymmetrical, non-gravitational, and may display skipped or spared areas.
B lines arising from pulmonary edema should be bilateral, symmetrical, and in a dependent gradient (ie. most prominent at the bases).
B lines from infectious/inflammatory pathologies, on the other hand, are often asymmetrical, non-gravitational, and may display skipped or spared areas.
7/
In contrast, with infectious/inflammatory pathologies, you will see B lines which are NOT homogenous throughout the interspace.
You may see all the B lines arising from a single point on the pleura; or even A lines throughout part of the interspace.
In contrast, with infectious/inflammatory pathologies, you will see B lines which are NOT homogenous throughout the interspace.
You may see all the B lines arising from a single point on the pleura; or even A lines throughout part of the interspace.
February 6, 2025 at 6:33 PM
7/
In contrast, with infectious/inflammatory pathologies, you will see B lines which are NOT homogenous throughout the interspace.
You may see all the B lines arising from a single point on the pleura; or even A lines throughout part of the interspace.
In contrast, with infectious/inflammatory pathologies, you will see B lines which are NOT homogenous throughout the interspace.
You may see all the B lines arising from a single point on the pleura; or even A lines throughout part of the interspace.
6/
Next, we can look at the distribution of B lines across the interspace.
Pleural fluid fills interlobular septae in a predictable and regular way; which generates B lines that are evenly spaced throughout the whole interspace.
Next, we can look at the distribution of B lines across the interspace.
Pleural fluid fills interlobular septae in a predictable and regular way; which generates B lines that are evenly spaced throughout the whole interspace.
February 6, 2025 at 6:33 PM
6/
Next, we can look at the distribution of B lines across the interspace.
Pleural fluid fills interlobular septae in a predictable and regular way; which generates B lines that are evenly spaced throughout the whole interspace.
Next, we can look at the distribution of B lines across the interspace.
Pleural fluid fills interlobular septae in a predictable and regular way; which generates B lines that are evenly spaced throughout the whole interspace.
5/
In contrast, B lines arising from an irregular, ragged, interrupted pleural line are more likely to be from infectious/inflammatory pathologies.
(If you want to know WHY this happens - check out the video above!👆)
In contrast, B lines arising from an irregular, ragged, interrupted pleural line are more likely to be from infectious/inflammatory pathologies.
(If you want to know WHY this happens - check out the video above!👆)
February 6, 2025 at 6:33 PM
5/
In contrast, B lines arising from an irregular, ragged, interrupted pleural line are more likely to be from infectious/inflammatory pathologies.
(If you want to know WHY this happens - check out the video above!👆)
In contrast, B lines arising from an irregular, ragged, interrupted pleural line are more likely to be from infectious/inflammatory pathologies.
(If you want to know WHY this happens - check out the video above!👆)
4/
And there are several ultrasound features that we can use to tease apart these two types.
First: we can look at the pleural morphology.
B lines arising from a smooth, crisp, uniform pleural line are more likely to be from cardiogenic pulmonary edema.
And there are several ultrasound features that we can use to tease apart these two types.
First: we can look at the pleural morphology.
B lines arising from a smooth, crisp, uniform pleural line are more likely to be from cardiogenic pulmonary edema.
February 6, 2025 at 6:33 PM
4/
And there are several ultrasound features that we can use to tease apart these two types.
First: we can look at the pleural morphology.
B lines arising from a smooth, crisp, uniform pleural line are more likely to be from cardiogenic pulmonary edema.
And there are several ultrasound features that we can use to tease apart these two types.
First: we can look at the pleural morphology.
B lines arising from a smooth, crisp, uniform pleural line are more likely to be from cardiogenic pulmonary edema.
2/
Remember that B lines are generated because of something filling the interstitium & interlobular septae
Fluid can fill these spaces; but so can other things!
Pus, cells, fibrosis, blood - anything that can give you an interstitial pattern on a chest X ray can give you B lines on ultrasound.
Remember that B lines are generated because of something filling the interstitium & interlobular septae
Fluid can fill these spaces; but so can other things!
Pus, cells, fibrosis, blood - anything that can give you an interstitial pattern on a chest X ray can give you B lines on ultrasound.

February 6, 2025 at 6:33 PM
2/
Remember that B lines are generated because of something filling the interstitium & interlobular septae
Fluid can fill these spaces; but so can other things!
Pus, cells, fibrosis, blood - anything that can give you an interstitial pattern on a chest X ray can give you B lines on ultrasound.
Remember that B lines are generated because of something filling the interstitium & interlobular septae
Fluid can fill these spaces; but so can other things!
Pus, cells, fibrosis, blood - anything that can give you an interstitial pattern on a chest X ray can give you B lines on ultrasound.
The technique does require expertise in spectral doppler, and is not without pitfalls - it takes a certain level of #POCUS expertise
BUT I firmly believe that awareness of the concept is valuable for all levels of #POCUS users & clinicians; as it helps emphasize the importance of the venous side
BUT I firmly believe that awareness of the concept is valuable for all levels of #POCUS users & clinicians; as it helps emphasize the importance of the venous side

February 3, 2025 at 6:55 PM
Each of these has a characteristic doppler profile under normal physiologic conditions, which changes predictably with increasing congestion.
We can therefore scan multiple vessels and see if there is a pattern that supports diffuse venous congestion at the organ level.
We can therefore scan multiple vessels and see if there is a pattern that supports diffuse venous congestion at the organ level.

February 3, 2025 at 6:55 PM
Each of these has a characteristic doppler profile under normal physiologic conditions, which changes predictably with increasing congestion.
We can therefore scan multiple vessels and see if there is a pattern that supports diffuse venous congestion at the organ level.
We can therefore scan multiple vessels and see if there is a pattern that supports diffuse venous congestion at the organ level.
When assessing for clinically significant organ congestion with ultrasound, basic 2D ultrasound has its limits.
A plethoric IVC is a great start - it is highly sensitive, but not specific. A high CVP is a prerequisite to organ congestion; but by itself is not enough!
Enter: #VEXUS
A plethoric IVC is a great start - it is highly sensitive, but not specific. A high CVP is a prerequisite to organ congestion; but by itself is not enough!
Enter: #VEXUS

February 3, 2025 at 6:55 PM
When assessing for clinically significant organ congestion with ultrasound, basic 2D ultrasound has its limits.
A plethoric IVC is a great start - it is highly sensitive, but not specific. A high CVP is a prerequisite to organ congestion; but by itself is not enough!
Enter: #VEXUS
A plethoric IVC is a great start - it is highly sensitive, but not specific. A high CVP is a prerequisite to organ congestion; but by itself is not enough!
Enter: #VEXUS

The elusive volume status has got to be one of the most ubiquitous questions in medicine - and the most widely misunderstood 😕
It's my favourite soapbox 🎙️ - so much so, that I've made a 20-min video highlighting the 5 key rules of volume status
Video link ⬇️, but here's the TLDR: 🧵
#emimcc
It's my favourite soapbox 🎙️ - so much so, that I've made a 20-min video highlighting the 5 key rules of volume status
Video link ⬇️, but here's the TLDR: 🧵
#emimcc

January 29, 2025 at 2:53 PM
The elusive volume status has got to be one of the most ubiquitous questions in medicine - and the most widely misunderstood 😕
It's my favourite soapbox 🎙️ - so much so, that I've made a 20-min video highlighting the 5 key rules of volume status
Video link ⬇️, but here's the TLDR: 🧵
#emimcc
It's my favourite soapbox 🎙️ - so much so, that I've made a 20-min video highlighting the 5 key rules of volume status
Video link ⬇️, but here's the TLDR: 🧵
#emimcc
Confession: I LOVE hyponatremia 🤓
(I know, I know. What can I say, I'm a true internist!)
HypoNa is often feared, maligned, and misunderstood - but I promise it doesn't have to be scary!
Here are my top 10 hyponatremia tips and tricks - a 🧵
#emimcc
(I know, I know. What can I say, I'm a true internist!)
HypoNa is often feared, maligned, and misunderstood - but I promise it doesn't have to be scary!
Here are my top 10 hyponatremia tips and tricks - a 🧵
#emimcc

January 24, 2025 at 2:04 PM
Confession: I LOVE hyponatremia 🤓
(I know, I know. What can I say, I'm a true internist!)
HypoNa is often feared, maligned, and misunderstood - but I promise it doesn't have to be scary!
Here are my top 10 hyponatremia tips and tricks - a 🧵
#emimcc
(I know, I know. What can I say, I'm a true internist!)
HypoNa is often feared, maligned, and misunderstood - but I promise it doesn't have to be scary!
Here are my top 10 hyponatremia tips and tricks - a 🧵
#emimcc
Next to fluids, IV diuretics are some of the most commonly mis-prescribed medications in acute medicine 💉🩸
Let's unpack 5 common diuretic prescribing mistakes, and how to correct these 🧵
#emimcc
Let's unpack 5 common diuretic prescribing mistakes, and how to correct these 🧵
#emimcc

January 17, 2025 at 6:19 PM
Next to fluids, IV diuretics are some of the most commonly mis-prescribed medications in acute medicine 💉🩸
Let's unpack 5 common diuretic prescribing mistakes, and how to correct these 🧵
#emimcc
Let's unpack 5 common diuretic prescribing mistakes, and how to correct these 🧵
#emimcc
Suggested New Year's Resolution: more mindful prescribing of IV fluids 🫧
Far too often I see IV fluids thrown around with minimal consideration; meanwhile, we'll deliberate for hours about a dose of lasix 🤦♀️
Here are the 10 most common fluid prescription mistakes I see 🧵
#emimcc
Far too often I see IV fluids thrown around with minimal consideration; meanwhile, we'll deliberate for hours about a dose of lasix 🤦♀️
Here are the 10 most common fluid prescription mistakes I see 🧵
#emimcc
January 9, 2025 at 3:12 PM
Suggested New Year's Resolution: more mindful prescribing of IV fluids 🫧
Far too often I see IV fluids thrown around with minimal consideration; meanwhile, we'll deliberate for hours about a dose of lasix 🤦♀️
Here are the 10 most common fluid prescription mistakes I see 🧵
#emimcc
Far too often I see IV fluids thrown around with minimal consideration; meanwhile, we'll deliberate for hours about a dose of lasix 🤦♀️
Here are the 10 most common fluid prescription mistakes I see 🧵
#emimcc
9/
The transhepatic view - sometimes called the rescue view - is another great option for difficult cases ⛑️
This is found in the mid-axillary line in a coronal plane (for the long-axis). From your standard view of the kidney, fan or slide your probe anteriorly until the IVC pops into view.
The transhepatic view - sometimes called the rescue view - is another great option for difficult cases ⛑️
This is found in the mid-axillary line in a coronal plane (for the long-axis). From your standard view of the kidney, fan or slide your probe anteriorly until the IVC pops into view.
December 16, 2024 at 6:52 PM
9/
The transhepatic view - sometimes called the rescue view - is another great option for difficult cases ⛑️
This is found in the mid-axillary line in a coronal plane (for the long-axis). From your standard view of the kidney, fan or slide your probe anteriorly until the IVC pops into view.
The transhepatic view - sometimes called the rescue view - is another great option for difficult cases ⛑️
This is found in the mid-axillary line in a coronal plane (for the long-axis). From your standard view of the kidney, fan or slide your probe anteriorly until the IVC pops into view.
8/
Next: don't forget your troubleshooting arsenal 🏹
The IVC can be tough, so it's worth having a couple tricks up your sleeve for challenging cases 🃏
For example - the phased array probe (vs the curvilinear) often nestles better into the subxiphoid space, giving you a better view.
Next: don't forget your troubleshooting arsenal 🏹
The IVC can be tough, so it's worth having a couple tricks up your sleeve for challenging cases 🃏
For example - the phased array probe (vs the curvilinear) often nestles better into the subxiphoid space, giving you a better view.
December 16, 2024 at 6:52 PM
8/
Next: don't forget your troubleshooting arsenal 🏹
The IVC can be tough, so it's worth having a couple tricks up your sleeve for challenging cases 🃏
For example - the phased array probe (vs the curvilinear) often nestles better into the subxiphoid space, giving you a better view.
Next: don't forget your troubleshooting arsenal 🏹
The IVC can be tough, so it's worth having a couple tricks up your sleeve for challenging cases 🃏
For example - the phased array probe (vs the curvilinear) often nestles better into the subxiphoid space, giving you a better view.
6/
We also want to be wary of overcalling "IVC collapse" in the long-axis, especially if we're losing the clearly defined borders of the vessel with inspiration 📏
You may be seeing lateral translation of the IVC with respiration - it's moving out of your plane of view - rather than true collapse
We also want to be wary of overcalling "IVC collapse" in the long-axis, especially if we're losing the clearly defined borders of the vessel with inspiration 📏
You may be seeing lateral translation of the IVC with respiration - it's moving out of your plane of view - rather than true collapse
December 16, 2024 at 6:52 PM
6/
We also want to be wary of overcalling "IVC collapse" in the long-axis, especially if we're losing the clearly defined borders of the vessel with inspiration 📏
You may be seeing lateral translation of the IVC with respiration - it's moving out of your plane of view - rather than true collapse
We also want to be wary of overcalling "IVC collapse" in the long-axis, especially if we're losing the clearly defined borders of the vessel with inspiration 📏
You may be seeing lateral translation of the IVC with respiration - it's moving out of your plane of view - rather than true collapse
5/
Thirdly: avoid assessing the IVC right at the diaphragm ❌
The diaphragm can either stent the IVC open or "pinch it" during respiration, which is not the same as true collapse.
Train your eye (ideally) a couple cm distal to the hepatic vein
Thirdly: avoid assessing the IVC right at the diaphragm ❌
The diaphragm can either stent the IVC open or "pinch it" during respiration, which is not the same as true collapse.
Train your eye (ideally) a couple cm distal to the hepatic vein
December 16, 2024 at 6:52 PM
5/
Thirdly: avoid assessing the IVC right at the diaphragm ❌
The diaphragm can either stent the IVC open or "pinch it" during respiration, which is not the same as true collapse.
Train your eye (ideally) a couple cm distal to the hepatic vein
Thirdly: avoid assessing the IVC right at the diaphragm ❌
The diaphragm can either stent the IVC open or "pinch it" during respiration, which is not the same as true collapse.
Train your eye (ideally) a couple cm distal to the hepatic vein
4/
Next: beware the pitfalls of a single view!
This is an axiom that holds true for all of POCUS - always look in more than one view 👍
With the IVC, the short-axis provides a plethora of useful information; including shape/sphericity, which is arguably the most useful parameter of all
Next: beware the pitfalls of a single view!
This is an axiom that holds true for all of POCUS - always look in more than one view 👍
With the IVC, the short-axis provides a plethora of useful information; including shape/sphericity, which is arguably the most useful parameter of all
December 16, 2024 at 6:52 PM
4/
Next: beware the pitfalls of a single view!
This is an axiom that holds true for all of POCUS - always look in more than one view 👍
With the IVC, the short-axis provides a plethora of useful information; including shape/sphericity, which is arguably the most useful parameter of all
Next: beware the pitfalls of a single view!
This is an axiom that holds true for all of POCUS - always look in more than one view 👍
With the IVC, the short-axis provides a plethora of useful information; including shape/sphericity, which is arguably the most useful parameter of all