



Ece Kartal
@ecekartal.bsky.social
🎓 previously @borklab.bsky.social @EMBL.org & @saezlab.bsky.social @uniHeidelberg.bsky.social
📍Heidelberg
🦠Human microbiome | Host-microbiome interactions | Multiomics integration
📍Heidelberg
🦠Human microbiome | Host-microbiome interactions | Multiomics integration
Reposted by Ece Kartal

The team's first preprint is out!
Led by
@vishnuprasoodanan.bsky.social & @omaistrenko.bsky.social , we asked a question (almost) as old as microbiology: how many prokaryotic species exist on Earth? More specifically, how much diversity is "hiding" in existing metagenomic data?
A 🧵.
Led by
@vishnuprasoodanan.bsky.social & @omaistrenko.bsky.social , we asked a question (almost) as old as microbiology: how many prokaryotic species exist on Earth? More specifically, how much diversity is "hiding" in existing metagenomic data?
A 🧵.

A census of hidden and discoverable microbial diversity beyond genome-centric approaches https://www.biorxiv.org/content/10.1101/2025.06.26.661807v1
June 27, 2025 at 8:10 PM
The team's first preprint is out!
Led by
@vishnuprasoodanan.bsky.social & @omaistrenko.bsky.social , we asked a question (almost) as old as microbiology: how many prokaryotic species exist on Earth? More specifically, how much diversity is "hiding" in existing metagenomic data?
A 🧵.
Led by
@vishnuprasoodanan.bsky.social & @omaistrenko.bsky.social , we asked a question (almost) as old as microbiology: how many prokaryotic species exist on Earth? More specifically, how much diversity is "hiding" in existing metagenomic data?
A 🧵.
Reposted by Ece Kartal

Pre-registration is now open for our second (free) course on phylogenomic data analysis and visualization using ETE, funded by @cziscience.bsky.social
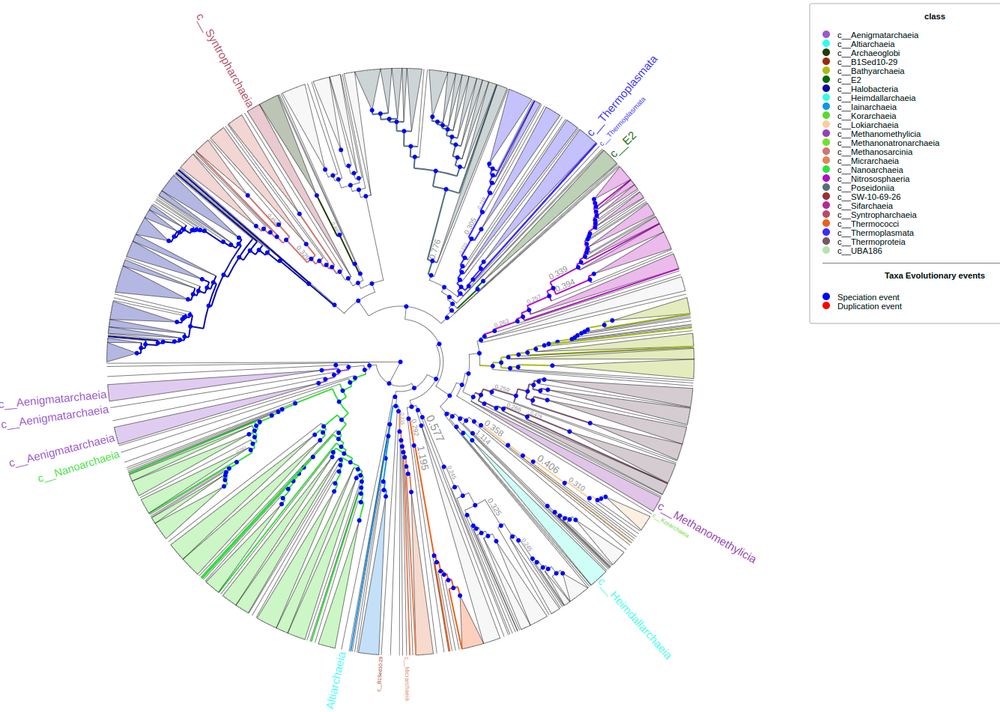
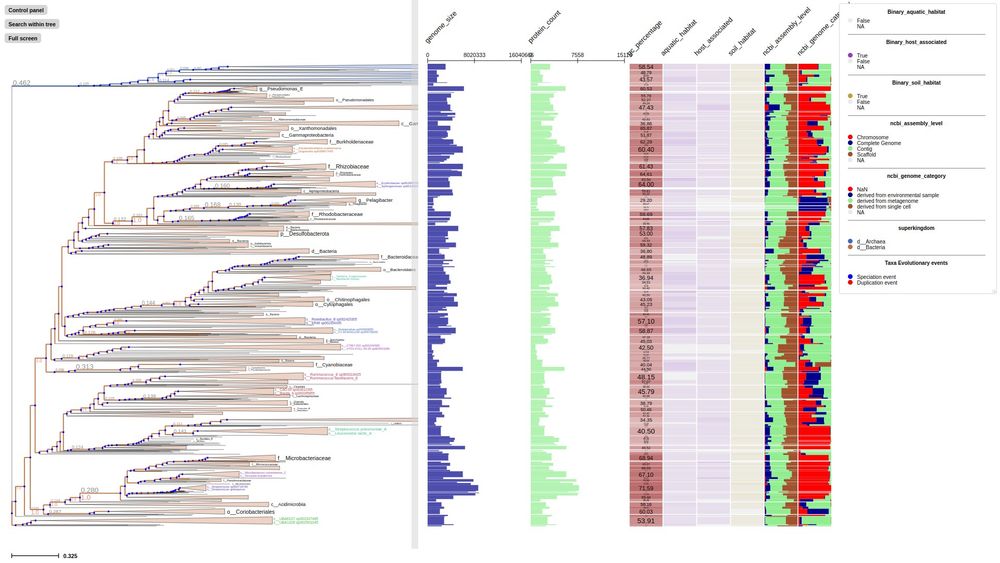
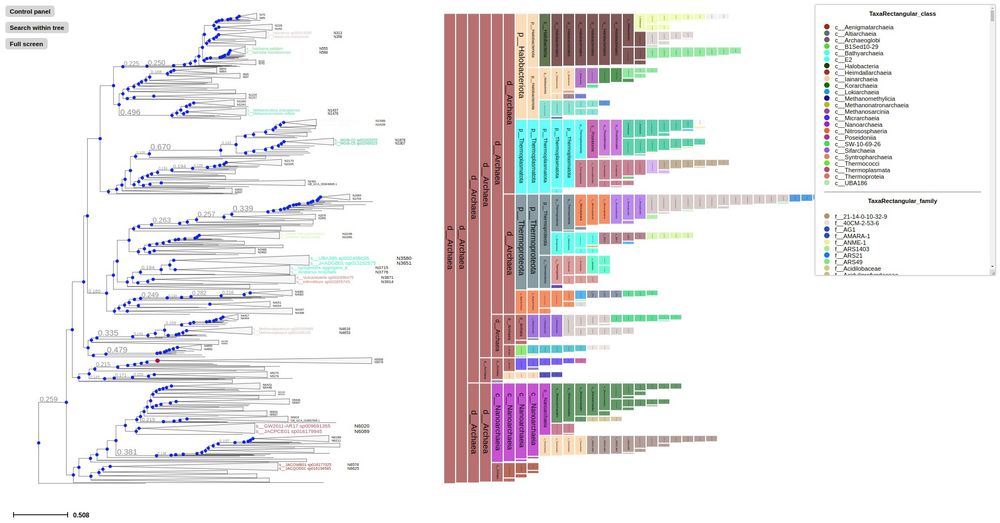
First time to cover new ETE4 features: Interactive viz of huge tree, profiling...
In Madrid, April 21-25. Travel fellowships available!
First time to cover new ETE4 features: Interactive viz of huge tree, profiling...
In Madrid, April 21-25. Travel fellowships available!
March 6, 2025 at 3:32 PM
Pre-registration is now open for our second (free) course on phylogenomic data analysis and visualization using ETE, funded by @cziscience.bsky.social
First time to cover new ETE4 features: Interactive viz of huge tree, profiling...
In Madrid, April 21-25. Travel fellowships available!
First time to cover new ETE4 features: Interactive viz of huge tree, profiling...
In Madrid, April 21-25. Travel fellowships available!
Reposted by Ece Kartal

"A faecal microbiota signature with high specificity for pancreatic cancer" by @ecekartal.bsky.social is an important step towards the early detection of PDAC, finding a panel of 27 microbial species with consistent accuracy across early and late disease stages (2022)
gut.bmj.com/content/...
gut.bmj.com/content/...

A faecal microbiota signature with high specificity for pancreatic cancer
Background Recent evidence suggests a role for the microbiome in pancreatic ductal adenocarcinoma (PDAC) aetiology and progression.
Objective To explore the faecal and salivary microbiota as potential diagnostic biomarkers.
Methods We applied shotgun metagenomic and 16S rRNA amplicon sequencing to samples from a Spanish case–control study (n=136), including 57 cases, 50 controls, and 29 patients with chronic pancreatitis in the discovery phase, and from a German case–control study (n=76), in the validation phase.
Results Faecal metagenomic classifiers performed much better than saliva-based classifiers and identified patients with PDAC with an accuracy of up to 0.84 area under the receiver operating characteristic curve (AUROC) based on a set of 27 microbial species, with consistent accuracy across early and late disease stages. Performance further improved to up to 0.94 AUROC when we combined our microbiome-based predictions with serum levels of carbohydrate antigen (CA) 19–9, the only current non-invasive, Food and Drug Administration approved, low specificity PDAC diagnostic biomarker. Furthermore, a microbiota-based classification model confined to PDAC-enriched species was highly disease-specific when validated against 25 publicly available metagenomic study populations for various health conditions (n=5792). Both microbiome-based models had a high prediction accuracy on a German validation population (n=76). Several faecal PDAC marker species were detectable in pancreatic tumour and non-tumour tissue using 16S rRNA sequencing and fluorescence in situ hybridisation.
Conclusion Taken together, our results indicate that non-invasive, robust and specific faecal microbiota-based screening for the early detection of PDAC is feasible.
Data are available in a public, open access repository. All data relevant to the study are included in the article or uploaded as supplementary information. The raw sequencing data for the samples are made available in the European Nucleotide Archive (ENA) under the study identifiers PRJEB38625 and PRJEB42013. Metadata for these samples are available as Supplementary Tables S1 and S2. Filtered taxonomic and functional profiles used as input for the statistical modelling pipeline are available in Supplementary Data S1 and S2. Analysis code and results available under [https://github.com/psecekartal/PDAC.git][1].
[1]: https://github.com/psecekartal/PDAC
gut.bmj.com
December 12, 2024 at 2:00 PM
"A faecal microbiota signature with high specificity for pancreatic cancer" by @ecekartal.bsky.social is an important step towards the early detection of PDAC, finding a panel of 27 microbial species with consistent accuracy across early and late disease stages (2022)
gut.bmj.com/content/...
gut.bmj.com/content/...