



Carl Öberg MD PhD
@carloberg.bsky.social
Associate Professor | PI Dialysis & Renal Physiology Group | Lund University Sweden 🇸🇪
Giedre's excellent thesis is now available for download at Lund University: portal.research.lu.se/en/publicati...
Brings tears to the eyes of a true PD-nerd 🎓🎓🎓
Brings tears to the eyes of a true PD-nerd 🎓🎓🎓

Clinical, Experimental and Theoretical Studies of Solute and Water Removal in Peritoneal Dialysis
portal.research.lu.se
February 12, 2025 at 4:15 PM
Giedre's excellent thesis is now available for download at Lund University: portal.research.lu.se/en/publicati...
Brings tears to the eyes of a true PD-nerd 🎓🎓🎓
Brings tears to the eyes of a true PD-nerd 🎓🎓🎓
Both as I understand it. HyperK is the major safety concern + CKD4-5 pts were excluded in all major trials RALES, EPHESUS etc. = lack of solid evidence showing that the benefits outweigh potential risks in these patients.
February 9, 2025 at 9:52 AM
Both as I understand it. HyperK is the major safety concern + CKD4-5 pts were excluded in all major trials RALES, EPHESUS etc. = lack of solid evidence showing that the benefits outweigh potential risks in these patients.
👍 In Sweden, sodium bicarbonate pills are 1000 mg and contain ~12 mEq of bicarbonate.
February 5, 2025 at 8:32 AM
👍 In Sweden, sodium bicarbonate pills are 1000 mg and contain ~12 mEq of bicarbonate.
So, the answer is: Yes, theoretically, you could survive on Baltic Sea water—but only if you follow a strict, low-salt diet to avoid dehydration. Without careful control of dietary salt, the kidneys would quickly be overwhelmed, leading to fluid loss and dehydration. 🌊💧❗️
February 4, 2025 at 5:15 PM
So, the answer is: Yes, theoretically, you could survive on Baltic Sea water—but only if you follow a strict, low-salt diet to avoid dehydration. Without careful control of dietary salt, the kidneys would quickly be overwhelmed, leading to fluid loss and dehydration. 🌊💧❗️
Here’s the catch: drinking 2 liters of Baltic Sea water (14 g of salt) leaves little room for dietary salt. A typical diet adds another 10–12 g/day, pushing the total salt intake to 24–26 g, exceeding the kidneys' ability to excrete salt efficiently (~10–12 g/L in urine) and lead to dehydration. ⚠️💧
February 4, 2025 at 5:15 PM
Here’s the catch: drinking 2 liters of Baltic Sea water (14 g of salt) leaves little room for dietary salt. A typical diet adds another 10–12 g/day, pushing the total salt intake to 24–26 g, exceeding the kidneys' ability to excrete salt efficiently (~10–12 g/L in urine) and lead to dehydration. ⚠️💧
So, let’s revisit the Baltic Sea. Its water contains ~7 g/L of salt, much lower than regular seawater. If you drink 2 L per day, that would be a salt intake of 14 g/day. Surprisingly, not far off from the average Swedish daily salt consumption of 10–12 g/day. Could this be feasible for survival? 🤔💧
February 4, 2025 at 5:15 PM
So, let’s revisit the Baltic Sea. Its water contains ~7 g/L of salt, much lower than regular seawater. If you drink 2 L per day, that would be a salt intake of 14 g/day. Surprisingly, not far off from the average Swedish daily salt consumption of 10–12 g/day. Could this be feasible for survival? 🤔💧
First, regular seawater has a salt concentration of ~35 g/L. Consuming seawater leads to dehydration because the kidneys can only produce urine with a maximum salt concentration of 10-12 g/L. So for every liter of seawater consumed, 3-3.5 liters of urine is needed to excrete all the excess salt. 🚫💧
February 4, 2025 at 5:15 PM
First, regular seawater has a salt concentration of ~35 g/L. Consuming seawater leads to dehydration because the kidneys can only produce urine with a maximum salt concentration of 10-12 g/L. So for every liter of seawater consumed, 3-3.5 liters of urine is needed to excrete all the excess salt. 🚫💧
By shedding light on this mechanism, our study may help pave the way for optimized dialysis strategies in the future. For a complete overview of our study design and findings, read more here: doi.org/10.1177/0896...
Sage Journals: Discover world-class research
Subscription and open access journals from Sage, the world's leading independent academic publisher.
doi.org
February 3, 2025 at 10:58 AM
By shedding light on this mechanism, our study may help pave the way for optimized dialysis strategies in the future. For a complete overview of our study design and findings, read more here: doi.org/10.1177/0896...
The data we gathered supports the idea of a transcellular route for glucose movement—with evidence indicating that GLUT1 is central to this process. This builds on our previous observations and adds a new layer of understanding to how peritoneal dialysis works.
February 3, 2025 at 10:58 AM
The data we gathered supports the idea of a transcellular route for glucose movement—with evidence indicating that GLUT1 is central to this process. This builds on our previous observations and adds a new layer of understanding to how peritoneal dialysis works.
Additional studies with indinavir (GLUT4-blocker) had no effect on FDG diffusion, leading us to conclude that the observed effects were likely the result of GLUT1-inhibition.
![Forest plot showing 95% confidence intervals for UF rate, free water transport, diffusion capacity (MTAC) for 18F-deoxyglucose ([18-F]-DG), and MTACs for glucose, creatinine, urea and potassium.](https://cdn.bsky.app/img/feed_thumbnail/plain/did:plc:mlm2rmhobpzknkridc7qmz2b/bafkreib6v2su3adcdcudd47bwrabz6rr74zygxzx7ne6rpiztldwhirg5u@jpeg)
February 3, 2025 at 10:58 AM
Additional studies with indinavir (GLUT4-blocker) had no effect on FDG diffusion, leading us to conclude that the observed effects were likely the result of GLUT1-inhibition.
In our study, we not only found that phloretin reduced FDG transfer, supporting our hypothesis of transcellular transfer, but also a significant reduction using GLUT1:GLUT4-blocker ritonavir.

February 3, 2025 at 10:58 AM
In our study, we not only found that phloretin reduced FDG transfer, supporting our hypothesis of transcellular transfer, but also a significant reduction using GLUT1:GLUT4-blocker ritonavir.
We hypothesized that the observed reduction in glucose absorption due to pan-GLUT-blocker phloretin was either due to a reduction in 1. trans-cellular glucose transfer and little trapping 2. cellular absorption and trapping in peritoneal cells, 3. para-cellular glucose transfer.

February 3, 2025 at 10:58 AM
We hypothesized that the observed reduction in glucose absorption due to pan-GLUT-blocker phloretin was either due to a reduction in 1. trans-cellular glucose transfer and little trapping 2. cellular absorption and trapping in peritoneal cells, 3. para-cellular glucose transfer.
Here, we tracked the journey of glucose across the peritoneal membrane studying both conventional glucose and radiolabeled glucose (18-F-deoxyglucose) in the opposite direction (plasma→dialysate). Diffusive transport capacities for glucose were similar regardless of the direction of transport.

February 3, 2025 at 10:58 AM
Here, we tracked the journey of glucose across the peritoneal membrane studying both conventional glucose and radiolabeled glucose (18-F-deoxyglucose) in the opposite direction (plasma→dialysate). Diffusive transport capacities for glucose were similar regardless of the direction of transport.
We previously showed that the pan-GLUT inhibitor phloretin reduced glucose absorption and increased UF, implicating facilitative glucose transporters. However, it was unclear if transport occurred via absorption or transcellular pathways, or which GLUTs were involved. doi.org/10.1681/ASN.2022040474

Phloretin Improves Ultrafiltration and Reduces Glucose... : Journal of the American Society of Nephrology
ally contribute to mass transfer are not fully understood. Intraperitoneal administration of phloretin, a nonselective blocker of facilitative glucose transporters (GLUTs), reduced glucose absorption ...
doi.org
February 3, 2025 at 10:58 AM
We previously showed that the pan-GLUT inhibitor phloretin reduced glucose absorption and increased UF, implicating facilitative glucose transporters. However, it was unclear if transport occurred via absorption or transcellular pathways, or which GLUTs were involved. doi.org/10.1681/ASN.2022040474
Reposted by Carl Öberg MD PhD

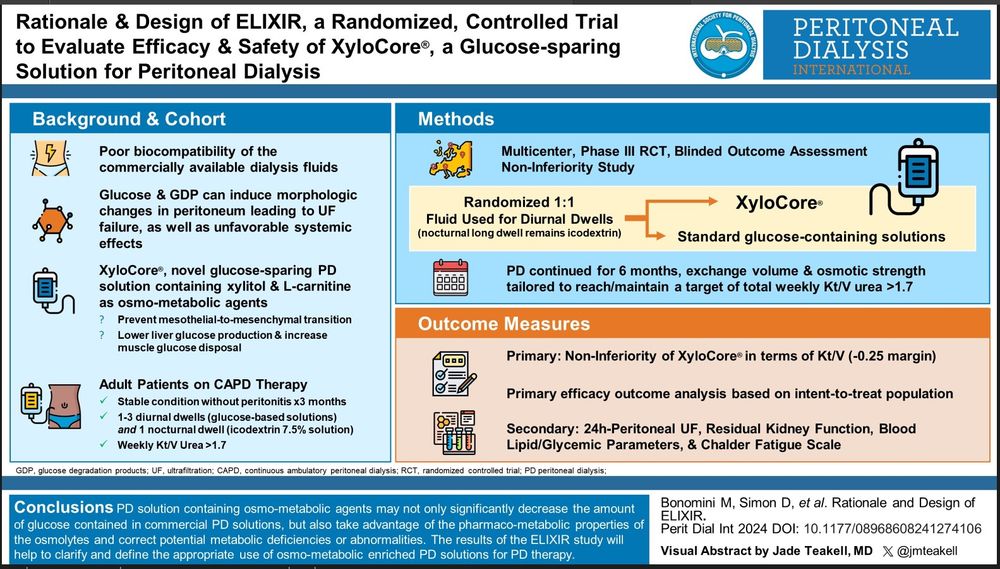
@pdi-journal.bsky.social @ispd.org @pd-perls.bsky.social
Original Article - journals.sagepub.com/doi/full/10....
Editorial - @johannmorelle.bsky.social @carloberg.bsky.social journals.sagepub.com/doi/full/10....
VA - @jmteakell.bsky.social
Original Article - journals.sagepub.com/doi/full/10....
Editorial - @johannmorelle.bsky.social @carloberg.bsky.social journals.sagepub.com/doi/full/10....
VA - @jmteakell.bsky.social
February 2, 2025 at 7:10 AM