



Aoxing Liu
@aoxing2.bsky.social
postdoc with Mark Daly at Broad Institute & MGH - curious about (large) chromosome alterations & (deep) human pedigrees + immunity, cancer & their interplay :)
A traditional "Comment" typically wouldn’t include such a "complicated" figure - we have to follow journal guidelines (=delete it from the paper).
However, we’re free to share the full version with you here!!
For those who think in pictures (myself included), I hope you find it clear & helpful! 🫶
However, we’re free to share the full version with you here!!
For those who think in pictures (myself included), I hope you find it clear & helpful! 🫶
October 17, 2025 at 2:43 AM
A traditional "Comment" typically wouldn’t include such a "complicated" figure - we have to follow journal guidelines (=delete it from the paper).
However, we’re free to share the full version with you here!!
For those who think in pictures (myself included), I hope you find it clear & helpful! 🫶
However, we’re free to share the full version with you here!!
For those who think in pictures (myself included), I hope you find it clear & helpful! 🫶
Thanks, Cristian!! 😄😄😄
August 21, 2025 at 4:39 PM
Thanks, Cristian!! 😄😄😄
And, the figure one you generated is so informative!!
June 11, 2025 at 9:46 PM
And, the figure one you generated is so informative!!
Thanks @struangrant.bsky.social and @agacita.bsky.social for seeing the uniqueness of our work and guiding others to understand it better!! Really appreciate your vision and insight!!
June 11, 2025 at 9:18 PM
Thanks @struangrant.bsky.social and @agacita.bsky.social for seeing the uniqueness of our work and guiding others to understand it better!! Really appreciate your vision and insight!!
8/n
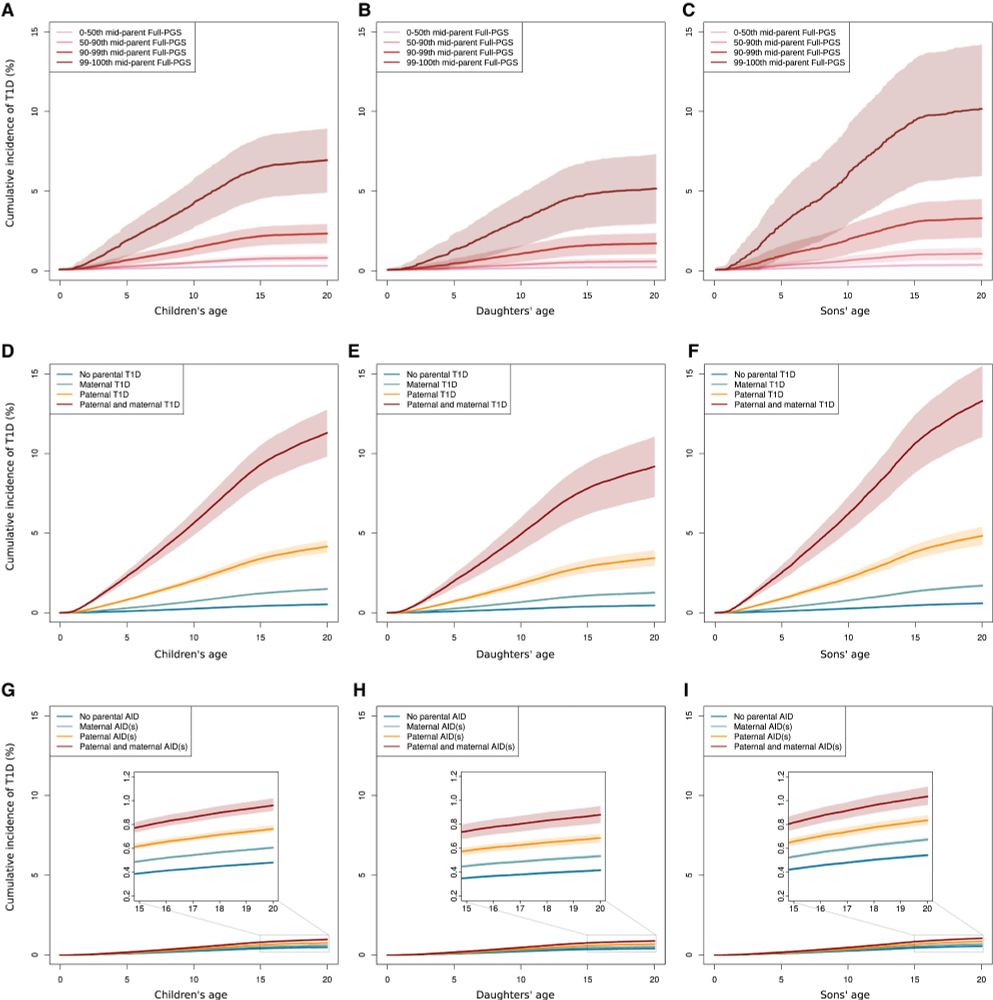
Parental T1D PGS is a strong predictor of T1D risk in children.
About parental PGSs of other AIDs - not adding too much to the prediction, given the high accuracy of T1D PGS.
PGS vs family history? High parental PGSs are usually more informative than a diagnosis of T1D in the mother or father.
Parental T1D PGS is a strong predictor of T1D risk in children.
About parental PGSs of other AIDs - not adding too much to the prediction, given the high accuracy of T1D PGS.
PGS vs family history? High parental PGSs are usually more informative than a diagnosis of T1D in the mother or father.
May 2, 2025 at 5:37 PM
8/n
Parental T1D PGS is a strong predictor of T1D risk in children.
About parental PGSs of other AIDs - not adding too much to the prediction, given the high accuracy of T1D PGS.
PGS vs family history? High parental PGSs are usually more informative than a diagnosis of T1D in the mother or father.
Parental T1D PGS is a strong predictor of T1D risk in children.
About parental PGSs of other AIDs - not adding too much to the prediction, given the high accuracy of T1D PGS.
PGS vs family history? High parental PGSs are usually more informative than a diagnosis of T1D in the mother or father.
7/n
People with AIDs are less likely to have children - for many reasons, including fear of transmitting diseases to offspring.
By estimating T1D risk for their children, couples can have informed family planning.
Also, children at high risk can benefit from targeted screening & early prevention.
People with AIDs are less likely to have children - for many reasons, including fear of transmitting diseases to offspring.
By estimating T1D risk for their children, couples can have informed family planning.
Also, children at high risk can benefit from targeted screening & early prevention.

May 2, 2025 at 5:07 PM
7/n
People with AIDs are less likely to have children - for many reasons, including fear of transmitting diseases to offspring.
By estimating T1D risk for their children, couples can have informed family planning.
Also, children at high risk can benefit from targeted screening & early prevention.
People with AIDs are less likely to have children - for many reasons, including fear of transmitting diseases to offspring.
By estimating T1D risk for their children, couples can have informed family planning.
Also, children at high risk can benefit from targeted screening & early prevention.
6/n
With pTDT, we see 2 main patterns for parent AID -> offspring T1D inheritance:
Pattern 1 – Overtransmission of both HLA & non-HLA PGSs for parental T1D, HYPO, RA, SLE.
Pattern 2 – Transmission occurs only for HLA: overtransmission for parental CD & psoriasis, undertransmission for IBD & MS.
With pTDT, we see 2 main patterns for parent AID -> offspring T1D inheritance:
Pattern 1 – Overtransmission of both HLA & non-HLA PGSs for parental T1D, HYPO, RA, SLE.
Pattern 2 – Transmission occurs only for HLA: overtransmission for parental CD & psoriasis, undertransmission for IBD & MS.

May 2, 2025 at 4:29 PM
6/n
With pTDT, we see 2 main patterns for parent AID -> offspring T1D inheritance:
Pattern 1 – Overtransmission of both HLA & non-HLA PGSs for parental T1D, HYPO, RA, SLE.
Pattern 2 – Transmission occurs only for HLA: overtransmission for parental CD & psoriasis, undertransmission for IBD & MS.
With pTDT, we see 2 main patterns for parent AID -> offspring T1D inheritance:
Pattern 1 – Overtransmission of both HLA & non-HLA PGSs for parental T1D, HYPO, RA, SLE.
Pattern 2 – Transmission occurs only for HLA: overtransmission for parental CD & psoriasis, undertransmission for IBD & MS.
5/n
But our original curiosity is about parents & children...
We can run polygenic transmission disequilibrium tests (pTDT) with AID HLA & non-HLA PGS in FinnGen trios!
A reminder - pTDT checks if AID risk variants are passed on more or less to children with T1D compared to what would be expected.
But our original curiosity is about parents & children...
We can run polygenic transmission disequilibrium tests (pTDT) with AID HLA & non-HLA PGS in FinnGen trios!
A reminder - pTDT checks if AID risk variants are passed on more or less to children with T1D compared to what would be expected.

May 2, 2025 at 3:55 PM
5/n
But our original curiosity is about parents & children...
We can run polygenic transmission disequilibrium tests (pTDT) with AID HLA & non-HLA PGS in FinnGen trios!
A reminder - pTDT checks if AID risk variants are passed on more or less to children with T1D compared to what would be expected.
But our original curiosity is about parents & children...
We can run polygenic transmission disequilibrium tests (pTDT) with AID HLA & non-HLA PGS in FinnGen trios!
A reminder - pTDT checks if AID risk variants are passed on more or less to children with T1D compared to what would be expected.
4/n
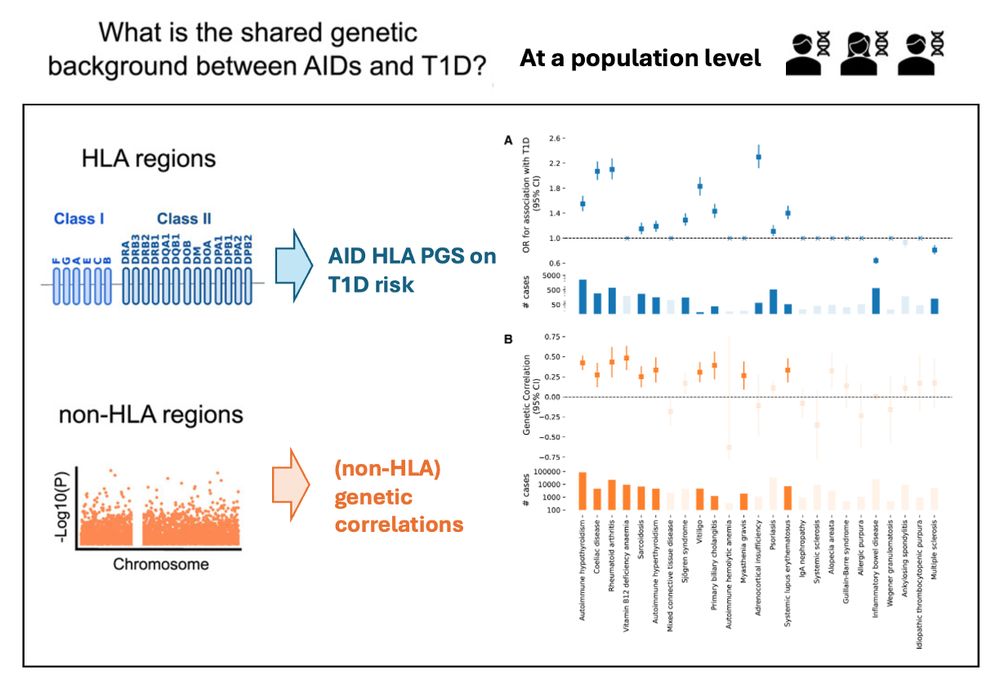
Now, let's revisit the question of the shared genetic background! 🧬🧬🧬
Overall, genetic analyses are consistent with epidemiological findings. For example, for HYPO, CD, RA, both HLA & non-HLA show positive effects.
However, for MS & IBD, non-HLA has no effect, while HLA has protective effects.
Now, let's revisit the question of the shared genetic background! 🧬🧬🧬
Overall, genetic analyses are consistent with epidemiological findings. For example, for HYPO, CD, RA, both HLA & non-HLA show positive effects.
However, for MS & IBD, non-HLA has no effect, while HLA has protective effects.
May 2, 2025 at 3:21 PM
4/n
Now, let's revisit the question of the shared genetic background! 🧬🧬🧬
Overall, genetic analyses are consistent with epidemiological findings. For example, for HYPO, CD, RA, both HLA & non-HLA show positive effects.
However, for MS & IBD, non-HLA has no effect, while HLA has protective effects.
Now, let's revisit the question of the shared genetic background! 🧬🧬🧬
Overall, genetic analyses are consistent with epidemiological findings. For example, for HYPO, CD, RA, both HLA & non-HLA show positive effects.
However, for MS & IBD, non-HLA has no effect, while HLA has protective effects.
3/n
Genetic correlation is straightforward but remember HLA - largely impacting T1D & other AIDs - is excluded by LDSC.
If genetic correlation is a genome-wide non-HLA measurement, how can we get HLA back into the game?
We built a within-sample HLA PGS with weighted ridge classifiers in FinnGen.
Genetic correlation is straightforward but remember HLA - largely impacting T1D & other AIDs - is excluded by LDSC.
If genetic correlation is a genome-wide non-HLA measurement, how can we get HLA back into the game?
We built a within-sample HLA PGS with weighted ridge classifiers in FinnGen.

April 28, 2025 at 3:15 AM
3/n
Genetic correlation is straightforward but remember HLA - largely impacting T1D & other AIDs - is excluded by LDSC.
If genetic correlation is a genome-wide non-HLA measurement, how can we get HLA back into the game?
We built a within-sample HLA PGS with weighted ridge classifiers in FinnGen.
Genetic correlation is straightforward but remember HLA - largely impacting T1D & other AIDs - is excluded by LDSC.
If genetic correlation is a genome-wide non-HLA measurement, how can we get HLA back into the game?
We built a within-sample HLA PGS with weighted ridge classifiers in FinnGen.
2/n
To what extent do the identified epidemiological associations result from genetics?🧬🧬🧬
Let’s download some summary stats and estimate some genetic correlations (quickly).
It looks not too bad - if we put the plot of epidemiological analysis aside for comparisons.
To what extent do the identified epidemiological associations result from genetics?🧬🧬🧬
Let’s download some summary stats and estimate some genetic correlations (quickly).
It looks not too bad - if we put the plot of epidemiological analysis aside for comparisons.

April 28, 2025 at 2:33 AM
2/n
To what extent do the identified epidemiological associations result from genetics?🧬🧬🧬
Let’s download some summary stats and estimate some genetic correlations (quickly).
It looks not too bad - if we put the plot of epidemiological analysis aside for comparisons.
To what extent do the identified epidemiological associations result from genetics?🧬🧬🧬
Let’s download some summary stats and estimate some genetic correlations (quickly).
It looks not too bad - if we put the plot of epidemiological analysis aside for comparisons.