



Ken Koon Wong
@kenkoonwong.bsky.social
data science enthusiast #rstats. infectious disease provider. lazy gardener. tai chi practitioner. life long learner. views are my own. RT or like != endorsement. https://www.kenkoonwong.com/
Pinned
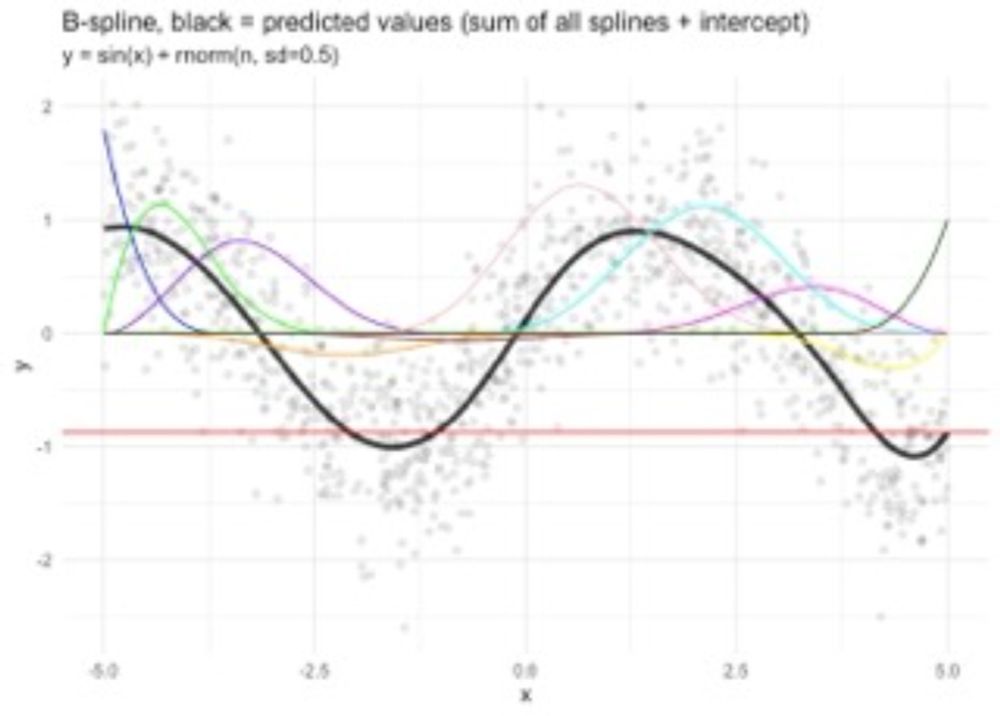
Understanding Basis Spline (B-spline) By Working Through Cox-deBoor Algorithm | Everyday Is A School Day
I finally understood B-splines by working through the Cox-deBoor algorithm step-by-step, discovering they're just weighted combinations of basis functions that make non-linear regression linear. What ...
www.kenkoonwong.com
I finally understood B-splines by working through the Cox-deBoor algorithm step-by-step, discovering they’re just weighted combo of basis functions that make non-linear regression linear. What surprised me is going through Bayesian statistics helped me understand the engine behind the model! #rstats
🧬 Explored molecular docking & MD simulations with penicillin binding to PBP2x — lots of stumbling through GROMACS but slowly piecing it together! 💊 Still much more to learn, but we’re getting there! 🔬 #gromacs

Exploring Molecular Docking & Molecular Dynamic Simulations - A Note To Myself | Everyday Is A School Day
🧬 Explored molecular docking & MD simulations with penicillin binding to PBP2x — lots of stumbling through GROMACS but slowly piecing it together! 💊 Still much more to learn, but we're getting there! ...
www.kenkoonwong.com
February 15, 2026 at 2:09 AM
🧬 Explored molecular docking & MD simulations with penicillin binding to PBP2x — lots of stumbling through GROMACS but slowly piecing it together! 💊 Still much more to learn, but we’re getting there! 🔬 #gromacs
Reposted by Ken Koon Wong

PROTECT trial (n=52) showed lower median DASC in ceftriaxone group (19.5 vs 53). No link found between DASC & new ARGs. DASC correlated with DOT, not AFD. 🧬💊##idsky
Effect of prophylactic antibiotics on days of antibiotic spectrum coverage in comatose post-cardiac arrest patients: a secondary analysis of PROTECT
Antibiotic resistance is a threat to public health driven in part by widespread antibiotic administration. Days of antibiotic spectrum coverage (DASC) is a novel metric to quantify both duration and breadth of antibiotic exposure that has not previously been used as an endpoint in a clinical trial. We calculated DASC using data from the Ceftriaxone to Prevent Pneumonia and Inflammation after Cardiac Arrest (PROTECT) trial to determine the association of ceftriaxone prophylaxis with DASC and with the acquisition of antibiotic resistance genes (ARGs).MethodsPROTECT randomized out-of-hospital cardiac arrest subjects to ceftriaxone or placebo for 3 days. ARGs were measured from rectal swabs collected at Days 0, 3 and 7 post randomization. DASC was calculated for each subject and compared using a two-sided Mann–Whitney U-test. Correlations between DASC and new ARGs, antibiotic-free days (AFD) and days of therapy (DOT) were tested using Kendall’s tau-alpha.ResultsPROTECT enrolled 52 subjects, 26 per treatment group, and treatment groups were similar at baseline. Median DASC scores were lower in the ceftriaxone group (19.5; IQR: 0, 43) compared with placebo (53; IQR: 16, 81). We found no correlation between DASC and new ARGs at either timepoint, or between DASC and AFD. DASC was correlated with DOT.ConclusionsDASC post intervention was lower in the ceftriaxone group, representing less antibiotic exposure following the intervention. There was no correlation between new ARGs and DASC. Further study is needed to understand the relationship between antibiotic prophylaxis, subsequent antibiotic exposure and resistome changes in the critically ill.
academic.oup.com
January 29, 2026 at 12:30 AM
PROTECT trial (n=52) showed lower median DASC in ceftriaxone group (19.5 vs 53). No link found between DASC & new ARGs. DASC correlated with DOT, not AFD. 🧬💊##idsky
Enjoyed learning the process of setting up a cluster of tiny PCs for parallel computing. A note to myself on installing Ubuntu, passwordless SSH, automating package installation across nodes, distributing #rstats simulations, and comparing CV5 vs CV10 performance. Fun project!

Setting Up A Cluster of Tiny PCs For Parallel Computing - A Note To Myself | Everyday Is A School Day
Enjoyed learning the process of setting up a cluster of tiny PCs for parallel computing. A note to myself on installing Ubuntu, passwordless SSH, automating package installation across nodes, distribu...
www.kenkoonwong.com
January 17, 2026 at 2:36 AM
Enjoyed learning the process of setting up a cluster of tiny PCs for parallel computing. A note to myself on installing Ubuntu, passwordless SSH, automating package installation across nodes, distributing #rstats simulations, and comparing CV5 vs CV10 performance. Fun project!
Reposted by Ken Koon Wong

If you don't want Claude to load all this great #RStats content for each session, try asking Claude Code to deconstruct this content into distinct skills. On first pass it did not add required YAML headers, so needed second pass with those instructions. Here are the skills I ended up with.

January 10, 2026 at 6:03 PM
If you don't want Claude to load all this great #RStats content for each session, try asking Claude Code to deconstruct this content into distinct skills. On first pass it did not add required YAML headers, so needed second pass with those instructions. Here are the skills I ended up with.
Testing Super Learner with TMLE showed some interesting patterns 🤔 XGBoost + random forest only hit ~54% coverage, but tuned xgboost + GLM reached ~90%. Seems like pairing flexible learners with stable (even misspecified) models helps? Need to explore this more with different setups 📊
#rstats
#rstats

Testing Super Learner's Coverage - A Note To Myself | Everyday Is A School Day
Testing Super Learner with TMLE showed some interesting patterns 🤔 XGBoost + random forest only hit ~54% coverage, but tuned xgboost + GLM reached ~90%. Seems like pairing flexible learners with stabl...
www.kenkoonwong.com
January 2, 2026 at 3:01 PM
Testing Super Learner with TMLE showed some interesting patterns 🤔 XGBoost + random forest only hit ~54% coverage, but tuned xgboost + GLM reached ~90%. Seems like pairing flexible learners with stable (even misspecified) models helps? Need to explore this more with different setups 📊
#rstats
#rstats
Reposted by Ken Koon Wong
In 827 enterococcal bacteremia cases, 21% had IE. DENOVi score (42% high risk) balanced safety (NLR 0.04) & echo use better than NOVA (76%) & DENOVA (26%).🔍💉##idsky
Prediction scores identifying patients at high risk of endocarditis in enterococcal bacteremia
Clinical prediction scores such as NOVA and DENOVA aim to identify patients with enterococcal bacteremia at low risk of infective endocarditis (IE) in whom imaging might be safely avoided. The aim was to evaluate the performance of NOVA and DENOVA scores and to introduce a modified tool, DENOVi.MethodsThis retrospective study included adult patients with enterococcal bacteremia at two Swiss tertiary centers (2015–2024). IE was adjudicated by multidisciplinary Endocarditis Teams according to 2023 Duke-ISCVID criteria. Patients were stratified as high risk for IE using the adapted NOVA score (cut-off: ≥4), the DENOVA score (≥3), and a newly developed DENOVi score (≥2), which excluded the subjective murmur criterion and broadened “valve disease” to include intracardiac electronic devices (new Vi component).ResultsAmong 827 bacteremia episodes, 172 (21%) were diagnosed with IE. The adapted NOVA, DENOVA, and DENOVi scores classified 76%, 26%, and 42% of patients as high risk, respectively. Corresponding NLRs were 0.04 (95% CI, 0.01–0.15), 0.10 (0.06–0.16), and 0.04 (0.02–0.10). The adapted NOVA substantially increased the proportion of echocardiograms needed to be performed from 58% based on clinical evaluation alone to 76%, whereas the DENOVA and DENOVi scores would have reduced this proportion to 26% and 42% of episodes, respectively.ConclusionsBoth adapted NOVA and DENOVi scores reliably ruled out IE, but DENOVi provided the most balanced approach between diagnostic safety and resource utilization. DENOVi therefore represents a pragmatic and objective tool for IE risk stratification in enterococcal bacteremia. Prospective validation is warranted.
academic.oup.com
December 23, 2025 at 11:30 PM
In 827 enterococcal bacteremia cases, 21% had IE. DENOVi score (42% high risk) balanced safety (NLR 0.04) & echo use better than NOVA (76%) & DENOVA (26%).🔍💉##idsky
📚 Tried building Super Learner from scratch to understand what’s happning under the hood. Walked thru the NNLS algorithm step-by-step—turns out ensembling models may beat solo models! Our homegrown vrsion? Srprisingly close to nnls package results ❤️ But, does it really work in real life? 🤷♂️
#rstats
#rstats

My Messy Notes on Building a Super Learner: Peeking Under The Hood of NNLS | Everyday Is A School Day
📚 Tried building Super Learner from scratch to understand what's happening under the hood. Walked through the NNLS algorithm step-by-step—turns out ensembling models may beat solo models! Our homegrow...
www.kenkoonwong.com
December 21, 2025 at 8:27 PM
📚 Tried building Super Learner from scratch to understand what’s happning under the hood. Walked thru the NNLS algorithm step-by-step—turns out ensembling models may beat solo models! Our homegrown vrsion? Srprisingly close to nnls package results ❤️ But, does it really work in real life? 🤷♂️
#rstats
#rstats
Reposted by Ken Koon Wong
N. farcinica DNA found in 51.4% of KFD vs 5.6% CD pts (P<0.001). N. positive KFD pts older, shorter onset, more leukopenia. Trauma/immunosuppression only in N. positive.🦠📊##idsky
Nocardia farcinica as a potential pathogen associated with a clinical subtype of Kikuchi-Fujimoto disease
Fever accompanied by disseminated lymphadenopathy presents a significant diagnostic challenge. Our prior clinical observations indicated a high detection rate of Nocardia farcinica (N. farcinica) DNA in patients with this presentation. Kikuchi-Fujimoto disease (KFD) is a common cause in young adults with fever and lymphadenopathy, yet its etiological drivers remain largely unknown.ObjectiveThis dual-center study aimed to investigate the prevalence of N. farcinica infection in a pathologically confirmed KFD cohort, to analyze its correlation with clinical phenotypes, particularly systemic involvement, in comparison to Castleman disease (CD).MethodsFormalin-fixed, paraffin-embedded tissue specimens from 35 KFD and 18 CD patients were tested by N. farcinica-specific qPCR. Clinical and imaging data were reviewed for comparison.ResultsN. farcinica DNA was significantly more prevalent in KFD (51.4%) than in CD (5.6%) (P<0.001). Within KFD, positive patients were older, had a shorter onset-to-presentation interval, and exhibited more pronounced leukopenia (all P<0.05). A history of recent trauma (11.1% vs. 0%) and immunosuppression (5.6% vs. 0%) was exclusively documented in the N. farcinica-positive group, albeit in small number. Furthermore, N. farcinica-positive patients showed a higher, though not statistically significant, prevalence of bilateral lymph node involvement (72.2% vs. 52.9%, P=0.34) and a trend towards involvement of more nodal regions compared to negative counterparts.ConclusionThis study demonstrated a potential association between N. farcinica and KFD, suggesting a clinical subtype characterized by older age, shorter onset-to-presentation interval, and significant leukopenia. These findings offer novel etiological insights and suggest potential targeted therapeutic approaches, warranting validation through larger prospective studies.
academic.oup.com
December 20, 2025 at 12:30 PM
N. farcinica DNA found in 51.4% of KFD vs 5.6% CD pts (P<0.001). N. positive KFD pts older, shorter onset, more leukopenia. Trauma/immunosuppression only in N. positive.🦠📊##idsky
Reposted by Ken Koon Wong
NTM infections rising 📈; M. avium causes lung disease. Sequential monotherapy = triple-drug combo in mice, cut lung bacteria, no resistance ↑. Promising safer tx! 🦠💊##idsky
Efficacies of sequenced monotherapies of Mycobacterium avium lung infection in mouse
The incidence of non-tuberculous mycobacterial (NTM) infections has been rising and now exceeds tuberculosis in several countries. Mycobacterium avium is the most common NTM cause of chronic lung disease. Current guidelines recommend simultaneous administration of three or more antibiotics, modeled after tuberculosis treatment, but these regimens are limited by toxicity, poor adherence, and low cure rates. Importantly, unlike M. tuberculosis, M. avium is acquired from the environment rather than transmitted between humans, weakening the rationale for multidrug therapy as necessary to suppress resistance.MethodsTo test an alternative treatment approach, we evaluated sequential monotherapy in a validated murine model of chronic M. avium lung infection. Mice were treated with either the standard triple-drug regimen of clarithromycin, ethambutol, and rifampicin or with sequential monotherapy: clarithromycin, bedaquiline, and clofazimine, with only one drug administered at a time for four-week intervals. Lung and spleen bacterial burdens were quantified, and minimum inhibitory concentrations (MICs) were determined for isolates recovered during treatment to assess resistance emergence.ResultsSequential monotherapy achieved reductions in lung bacterial burden equivalent to those of the standard multidrug regimen and prevented extrapulmonary dissemination. Notably, no increase in MICs was observed for clarithromycin, bedaquiline, or clofazimine across treatment phases, indicating that sequential monotherapy did not select for resistant clones.ConclusionsThese findings provide the first evidence that sequential monotherapy can deliver efficacy comparable to multidrug therapy for M. avium disease without promoting resistance. This proof-of-concept supports further investigation of sequencing strategies as a potentially more tolerable alternative to current triple-agent regimens.
academic.oup.com
December 20, 2025 at 12:30 AM
NTM infections rising 📈; M. avium causes lung disease. Sequential monotherapy = triple-drug combo in mice, cut lung bacteria, no resistance ↑. Promising safer tx! 🦠💊##idsky
Reposted by Ken Koon Wong
Nanopore sequencing ✅ bone samples (10/10) in diabetic foot osteomyelitis. Pathogen dominance linked to better outcomes (p=0.002). Matches culture results, predicts surgery success. 🦶🔬##idsky
Microbial Dominance in Diabetic Foot Osteomyelitis using Nanopore Sequencing Techniques Predicts Positive Response to Surgical Intervention
Existing tools to predict successful response to surgery for the treatment of diabetic foot osteomyelitis are lacking. Recent studies in non-bone infections have revealed that nanopore sequencing can provide real-time metagenomic identification of pathogens. In a cohort of patients with diabetic foot osteomyelitis, we tested the feasibility of generating interpretable metagenomic data from surgically-acquired osseous tissue, and compared bacterial community features (pathogen dominance) with clinical outcomes (resolution of infection). We hypothesized that nanopore-generated microbial data can be feasibly generated from surgically-acquired bone, aligns with conventional culture results, and is predictive of clinical response.MethodsWe performed a pilot feasibility study of ten consecutive patients hospitalized with diabetic foot osteomyelitis who underwent surgery for osteomyelitis. We performed metagenomic sequencing of surgical bone samples using the MinION (Oxford Nanopore). Our primary metagenomic index was community dominance (relative abundance of most abundant species). Our primary clinical endpoint was clinical response to surgery, adjudicated at one year.ResultsWe successfully generated interpretable metagenomic data from all (10/10) specimens, including two specimens with negative culture growth. Among culture-positive specimens, the culture-identified pathogen was either the first or second most abundant organism in all cases. Patients with favorable clinical response exhibited greater pathogen dominance than patients with unfavorable response (p=0.002).ConclusionsIn patients with surgically treated osteomyelitis, nanopore sequencing can generate interpretable metagenomic data from bone specimens that is culture-concordant and associated with clinical response. These findings support the feasibility and plausibility of using real-time metagenomic sequencing to improve the clinical management of osteomyelitis.
academic.oup.com
December 17, 2025 at 1:00 PM
Nanopore sequencing ✅ bone samples (10/10) in diabetic foot osteomyelitis. Pathogen dominance linked to better outcomes (p=0.002). Matches culture results, predicts surgery success. 🦶🔬##idsky
Reposted by Ken Koon Wong
DFO remission at 12m: bone biopsy 31.4%📉, ulcer bed biopsy 39.4%📈; no clear benefit of bone biopsy. Antibiotics matched bacteria in 85.9% cases. Bone biopsy not essential🦶.##idsky
“Bone biopsy not superior to ulcer bed biopsy guided antibacterial therapy on remission of diabetic foot osteomyelitis: A randomized controlled trial”
Percutaneous bone biopsy is the reference standard for guiding antibiotic therapy in diabetic foot osteomyelitis (DFO). However, ulcer bed biopsies are commonly used in practice. This study aimed to compare 12-month outcomes of conservatively treated DFO patients whose antibiotic regimens were based on cultures of either percutaneous bone or ulcer bed biopsy.MethodsWe conducted a multicenter, double-blind randomized clinical trial in 84 adult participants with DFO. All underwent a percutaneous bone biopsy and an ulcer bed biopsy. Participants were randomly allocated to antibiotic treatment based on either bone biopsy cultures or ulcer bed biopsy cultures. The primary outcome, DFO remission, was assessed at 12 months using both intention-to-treat (ITT) and per-protocol analyses (PP) with generalized linear models.ResultsThe remission rate in the bone biopsy group was 31.4% (95% CI 18.1-48.7%) and 39.4% (95% CI 24.2-57.0%) in the ulcer bed biopsy group. The RR of not achieving remission at 12 months in the bone biopsy group was 1.13; (95% CI 0.80-1.60) in the ITT analyses and ranged from 1.12 to 1.18 in the PP analyses. Antibiotics targeting bacteria identified in the unblinded sample were effective against all bacteria cultured from the blinded sample in 85.9% of cases (n=61).ConclusionsThis study found no evidence to recommend bone biopsies prior to the start of antibiotics in patients with DFO. In most cases, the antibiotics targeted bacteria in both samples, possibly contributing to the equivalence of the results in outcomes in both groups.Clinical trial registrationNetherlands Trial Register NL 7582.
academic.oup.com
December 17, 2025 at 2:00 PM
DFO remission at 12m: bone biopsy 31.4%📉, ulcer bed biopsy 39.4%📈; no clear benefit of bone biopsy. Antibiotics matched bacteria in 85.9% cases. Bone biopsy not essential🦶.##idsky
Reposted by Ken Koon Wong
ML predicts AMR from MALDI-TOF data with AUROC ~0.81-0.85 for E. coli, K. pneumoniae, S. aureus. Performance drops by 0.10-0.25 AUROC over 18 months 📉. Local, regular retraining needed.##idsky
Prediction of antimicrobial resistance from MALDI-TOF mass spectra using machine learning: a validation study
ABSTRACTMatrix-assisted laser desorption-ionization-time of flight (MALDI-TOF) mass spectra can be used to predict antimicrobial resistance (AMR) using machine learning (ML). This study aimed to validate the performance of ML models for AMR prediction using own and publicly available MALDI-TOF data and to test how these models perform over time. Mass spectra of Escherichia coli (n = 7,897), Klebsiella pneumoniae (n = 2,444), and Staphylococcus aureus (n = 4,664) from routine diagnostics (Germany) and the DRIAMS-A database (Switzerland) were used. Six classification models were benchmarked for AMR prediction using cross-validation (regularized logistic regressions [LR], multilayer perceptrons [MLP], support vector machines [SVM], random forests [RF], gradient boosting machines [LGBM, XGB]). Performance was prospectively observed for 18 months after training. The performance of AMR prediction evaluated by the mean area under the receiver operating characteristic curve (AUROC) was comparable between the DRIAMS-A data set and own data. The best predictive performance (classifier, AUROC) on own data was achieved for oxacillin resistance in S. aureus (RF, 0.85), ciprofloxacin resistance in E. coli (XGB, 0.83), and piperacillin-tazobactam resistance in K. pneumoniae (XGB, 0.81). ML performance was poor if training and test data were unrelated in terms of location and time. Performance (change in AUROC) decreased within 18 months after training for S. aureus (oxacillin resistance, RF: −0.10), E. coli (ciprofloxacin, XGB: −0.19), and K. pneumoniae (piperacillin-tazobactam, XGB: −0.25). The performance of ML for the prediction of AMR based on MALDI-TOF data is good (AUROC ≥ 0.8) but classifiers need to be trained on local data and retrained regularly to maintain the performance level.IMPORTANCEMALDI-TOF mass spectrometry can be used not only for bacterial species identification but also for the prediction of antimicrobial resistance (AMR) using machine learning (ML). Such an approach would provide antimicrobial susceptibility test results one day earlier than conventional routine diagnostics. This is essential for an early targeted treatment to reduce mortality of severe infections. We show that the performance of ML for the prediction of AMR based on MALDI-TOF data is good (AUROC ≥ 0.8). However, the ML models need to be trained on local data and retrained regularly to maintain a good performance.
journals.asm.org
December 7, 2025 at 11:30 PM
ML predicts AMR from MALDI-TOF data with AUROC ~0.81-0.85 for E. coli, K. pneumoniae, S. aureus. Performance drops by 0.10-0.25 AUROC over 18 months 📉. Local, regular retraining needed.##idsky
Reposted by Ken Koon Wong
Nanopore sequencing of 60 samples from 38 CAP pts showed sputum had 192K bacterial reads vs 14K in swabs, improving pathogen ID (e.g., S. pneumoniae, M. pneumoniae) & antibiotic targeting.🦠💨##idsky
P33 Metagenomic sequencing of sputum enables accurate, non-invasive diagnosis of community-acquired pneumonia
Community-acquired pneumonia (CAP) remains a major cause of hospital admission and mortality, yet the causative pathogen is rarely identified. Conventional diagnostics, including sputum culture, blood culture and multiplex PCR, lack sensitivity, breadth, or speed. Consequently, most patients receive empirical antibiotics, with implications for antimicrobial stewardship and patient outcomes. Invasive sampling (e.g. bronchoalveolar lavage) improves diagnostic yield but is often impractical in routine care. Nanopore metagenomic sequencing offers unbiased, real-time pathogen detection, but its utility using non-invasive specimens such as swabs and sputum remains underexplored.MethodsWe performed Nanopore-based metagenomic sequencing on 60 respiratory samples (46 nasopharyngeal swabs, 12 sputa, 2 pleural fluids) from 38 adults hospitalized with CAP and 8 matched controls. The higher number of swabs reflects the practical challenges of sputum collection in hospitalized CAP patients, where non-production is common. We also performed a paired analysis on patients who had both swab and sputum collected, enabling direct comparison of sample types. Protocols incorporated host DNA depletion, microbial and viral workflows, and rigorous bioinformatics (taxonomic classification, genome breadth and read dispersion metrics) to distinguish true pathogens from commensals. Sequencing results were compared with routine microbiological diagnostics and reviewed in a multidisciplinary clinical context.ResultsHost depletion reduced human DNA contamination and enriched microbial reads. Sputum consistently provided higher bacterial read counts (median 192 426 versus 14 025 per sample), deeper genome coverage and more uniform read distribution. Clinically relevant pathogens identified in sputum included Streptococcus pneumoniae, Streptococcus pyogenes, Moraxella catarrhalis and Mycoplasmoides pneumoniae. Two samples (one sputum and one swab) from a patient were confirmed as M. pneumoniae positive by qPCR but missed by routine diagnostic tests. Within patient comparison with paired swab-sputum samples showed that swabs were dominated by upper airway commensals (e.g. Dolosigranulum pigrum), whereas sputum reliably reflected lower respiratory tract infections. Metagenomics additionally identified polymicrobial infections and potential resistance determinants in sputum and pleural fluid samples.ConclusionsOur study demonstrates that sputum-based Nanopore metagenomic sequencing is a powerful, non-invasive alternative to invasive lower respiratory tract sampling in CAP. It improves pathogen identification and expands coverage beyond culture and PCR assays. By bridging laboratory workflows with clinical decision-making, this approach could improve CAP management—particularly for patients able to provide sputum —by supporting rapid targeted therapy, optimizing antibiotic use and reducing diagnostic uncertainty in one of the most common serious infections worldwide.ImpactThis work highlights the tangible clinical–laboratory connection: how metagenomic sequencing, applied to a readily available specimen, can shift pneumonia diagnostics from empiricism toward precision. The findings position sputum metagenomics as a scalable tool for hospitals, especially in settings where invasive sampling is not feasible, with direct relevance to antimicrobial stewardship programmes and patient outcomes.
academic.oup.com
December 6, 2025 at 4:00 PM
Nanopore sequencing of 60 samples from 38 CAP pts showed sputum had 192K bacterial reads vs 14K in swabs, improving pathogen ID (e.g., S. pneumoniae, M. pneumoniae) & antibiotic targeting.🦠💨##idsky
Reposted by Ken Koon Wong
Study on 42 adults found bictegravir (BIC) exposure ↓ by 79% with Al/Mg antacid, 33% Ca, 63% Fe supplements. Taking BIC 2h before or with food lessens effect.🥼💊##idsky
The effect of antacid and mineral supplements on bictegravir pharmacokinetics: results from a Phase 1, open-label, drug–drug interaction study
ABSTRACTThe mechanism of action of integrase strand transfer inhibitors involves binding to magnesium ions in the active site of the HIV integrase enzyme, making them susceptible to chelation-type drug–drug interactions with metal cation–containing medications. This study evaluated the potential of metal cation–containing antacids and mineral supplements to impact bictegravir (BIC) exposure and assessed alternative approaches for combined use. This was an open-label, single-dose, Phase 1 study in adult participants without HIV. The pharmacokinetics and safety of BIC (administered as part of a single-tablet combination with emtricitabine [F] and tenofovir alafenamide [TAF; B/F/TAF]) were assessed when co-administered with maximum-strength aluminum/magnesium-containing antacid (referred to as “aluminum/magnesium-containing antacid”), calcium carbonate, or ferrous fumarate under fasted and fed conditions, and administered 2 hours before or after the antacid. Pharmacokinetic parameters were compared using analysis of variance to calculate geometric least-squares mean ratios and 90% confidence intervals. Forty-two participants were enrolled. BIC exposure (area under the plasma concentration–time curve extrapolated to infinity) was reduced by 79%, 33%, and 63%, respectively, when co-administered with aluminum/magnesium-containing antacid, calcium carbonate, and ferrous fumarate under fasted conditions. Co-administration of B/F/TAF with calcium carbonate or ferrous fumarate with a meal and administration of B/F/TAF 2 hours before the antacid reduced the impact of the interactions. B/F/TAF was well tolerated alone or in combination with metal cation–containing medications. Co-administration of BIC and calcium/iron-containing supplements with a meal and administration of BIC 2 hours or more before aluminum/magnesium-containing antacids are some of the effective strategies to mitigate chelation effects on BIC exposure.This study was registered at NCT05502341/NCT06333808.
journals.asm.org
December 5, 2025 at 11:00 PM
Study on 42 adults found bictegravir (BIC) exposure ↓ by 79% with Al/Mg antacid, 33% Ca, 63% Fe supplements. Taking BIC 2h before or with food lessens effect.🥼💊##idsky
Reposted by Ken Koon Wong
Cefiderocol + taniborbactam restored susceptibility in 95.2% (20/21) of NDM+ P. aeruginosa from Vietnam/Nigeria; xeruborbactam had no effect. 💊🔬##idsky
Efficacy of cefiderocol in combination with xeruborbactam versus taniborbactam against cefiderocol-resistant NDM-producing Pseudomonas aeruginosa
ABSTRACTWe evaluated the in vitro activity of cefiderocol in combination with either taniborbactam or xeruborbactam against cefiderocol-resistant, blaNDM-positive Pseudomonas aeruginosa clinical isolates from Vietnam and Nigeria. Taniborbactam restored cefiderocol susceptibility in most isolates (20/21, 95.2%), while xeruborbactam had no effect. Resistance was reversed by dipicolinic acid, which confirmed New-Delhi Metallo-β-Lactamase (NDM-mediated) resistance. One isolate that was unresponsive to taniborbactam carried multiple copies of blaNDM-1. These findings highlight the species-specific limitations of xeruborbactam in P. aeruginosa.
journals.asm.org
December 3, 2025 at 1:00 AM
Cefiderocol + taniborbactam restored susceptibility in 95.2% (20/21) of NDM+ P. aeruginosa from Vietnam/Nigeria; xeruborbactam had no effect. 💊🔬##idsky
Reposted by Ken Koon Wong
FDA warns TMP-SMX ↑ risk of acute respiratory failure in 10-24y vs amoxicillin/cephalosporins: 0.03% vs 0.01% risk; RR ~2.8; careful risk-benefit needed.⚠️🏥##idsky
Trimethoprim-Sulfamethoxazole and Acute Respiratory Failure in Adolescents and Young Adults
Importance
The US Food and Drug Administration (FDA) has issued a warning and a label change regarding a potential association between trimethoprim-sulfamethoxazole (TMP-SMX) and acute respiratory failure in healthy adolescents and young adults.Objective
To examine the 30-day risk of a hospital visit (ie, hospitalization or emergency department visit) with acute respiratory failure in adolescents and young adults aged 10 to younger than 25 years old newly dispensed oral TMP-SMX compared with new users of amoxicillin or a cephalosporin.Design, Setting, and Participants
This retrospective, population-based, new-user cohort study in Ontario, Canada (2003-2023) used linked administrative health care data. The TMP-SMX vs amoxicillin and TMP-SMX vs cephalosporins cohorts both included adolescents and young adults aged 10 to younger than 25 years who were newly dispensed oral TMP-SMX, amoxicillin, or cephalosporins for 3 or more days from an outpatient pharmacy. Data were analyzed from January 1 to April 30, 2025.Exposure
TMP-SMX for 3 days or more.Main Outcomes and Measures
The primary outcome was a composite outcome of the 30-day risk of a hospital visit with acute respiratory failure (defined as a diagnosis of acute respiratory failure or receipt of mechanical ventilation, tracheotomy, or extracorporeal membrane oxygenation). Secondary outcomes were the individual components of the composite outcome, all-cause hospitalization, and all-cause mortality. Overlap weighting on the propensity score was used to balance comparison groups on 84 indicators of baseline health. Weighted risk ratios were obtained using log-binomial regression and weighted risk differences using binomial regression. Sensitivity analyses using a negative control outcome, and case-crossover analysis were also performed.Results
The TMP-SMX vs amoxicillin cohort included 575 218 individuals (44 801 TMP-SMX users and 530 417 amoxicillin users; median age after weighting, 19 years [IQR, 16-22 years]; 74.3% female). The TMP-SMX vs cephalosporins cohort included 248 236 individuals (51 197 TMP-SMX users and 197 039 cephalosporin users; median age after weighting, 19 years [IQR, 16-22 years]; 72.3% were female). The risk of the composite outcome occurred in 15 of 44 801 patients (0.03%) who started TMP-SMX and in 49 of 530 417 (0.01%) who started amoxicillin (number of weighted events, 7 of 21 579 [0.03%] for TMP-SMX and 2 of 21 579 [0.01%] for amoxicillin; weighted risk ratio, 2.79 [95% CI, 1.01-7.71]; weighted risk difference, 0.02% [95% CI, 0.001%-0.04%]). The risk of the composite outcome occurred in 17 of 51 197 patients (0.03%) who started TMP-SMX and in 21 of 197 039 (0.01%) who started cephalosporins (number of weighted events, 8 of 20 538 [0.04%] for TMP-SMX and 3 of 20 538 [0.01%] for cephalosporins; weighted risk ratio, 2.85 [95% CI, 1.11-7.31]; weighted risk difference, 0.02% [95% CI, 0.005%-0.05%]). Results were consistent in sensitivity analyses.Conclusions and Relevance
These findings suggest that the 30-day risk of a hospital visit with acute respiratory failure was higher among those receiving TMP-SMX compared with those receiving amoxicillin or cephalosporins. These findings supported the FDA warning, and if replicated, the risks should be carefully weighed against the benefits of TMP-SMX use. Regulatory agencies could reinforce the FDA warning, and product monographs and prescribing guidelines should be updated and revised accordingly.
jamanetwork.com
December 2, 2025 at 11:00 PM
FDA warns TMP-SMX ↑ risk of acute respiratory failure in 10-24y vs amoxicillin/cephalosporins: 0.03% vs 0.01% risk; RR ~2.8; careful risk-benefit needed.⚠️🏥##idsky
Reposted by Ken Koon Wong
Vancomycin & linezolid resistances in enterococci rise globally. pELF plasmids show 2 lineages, evolving via circular plasmid integration 🌍🔬 #AntibioticResistance##idsky
Ongoing independent evolution of linezolid and vancomycin-resistance pELF-type linear plasmids across the One Health spectrum
ABSTRACTVancomycin and linezolid are crucial for treating enterococcal infections. The global emergence of linezolid- and vancomycin-resistant enterococci is a growing concern. Enterococcal pELF-type linear plasmids, which confer both types of resistance, have been identified worldwide from clinical and environmental sources. Phylogenetic and structural analyses of pELF-type linear plasmids revealed that they diverged into two distinct lineages and evolved through the integration of circular plasmids. Our findings on this ongoing evolution advance the fundamental knowledge required for the future development of global and cross-sectoral surveillance.
journals.asm.org
November 30, 2025 at 6:30 PM
Vancomycin & linezolid resistances in enterococci rise globally. pELF plasmids show 2 lineages, evolving via circular plasmid integration 🌍🔬 #AntibioticResistance##idsky
Reposted by Ken Koon Wong
100 AI-in-IPC studies (2014-24) found: 75% ML use; 53% predictive analytics; 15% integrated tools. Barriers: data quality (45%), tech issues (16%). Risks: operational (35%), technical (33%). 🤖🦠📊##idsky
Advancing infection prevention and control through artificial intelligence: a scoping review of applications, barriers, and a decision-support checklist
View
abstract
Objective:To examine how artificial intelligence (AI) has been applied to infection prevention and control in healthcare, identify barriers and risks affecting implementation, and develop a structured checklist to support safe adoption.Design:Scoping review conducted in line with Joanna Briggs Institute methodology and reported according to PRISMA-ScR.Methods:PubMed, Scopus, and Web of Science were searched for primary studies (2014–2024) describing real-world AI applications for IPC. Studies reporting implementation experiences, outcomes, or risks were included. Data on study design, AI type, IPC function, integration level, barriers, and outcomes were extracted and synthesized thematically to derive a 41-item decision-support checklist.Results:Of 2,143 records screened, 100 studies met inclusion. Most were published since 2022, with the United States and China leading output. Machine learning dominated (75%), mainly for predictive analytics (53%), HAI detection (13%), and hand hygiene monitoring (13%). Only 15% of tools were integrated into existing digital infrastructures. Barriers centred on data quality (45%), technical and data related (16%), and economic/technical constraints (16%). Reported risks clustered around operational failures (35%), technical errors (33%), and data security (12%). Evidence was heavily skewed toward high-income countries, with limited prospective validation or implementation science.Conclusions:AI offers clear promise for IPC, particularly in early detection and compliance monitoring, but its translation into practice remains constrained by data fragmentation, limited integration, and uneven readiness across settings. Our evidence-informed checklist provides IPC teams with a structured tool to assess feasibility, governance, and resource needs before adoption, supporting safer and sustainable innovation.
www.cambridge.org
November 30, 2025 at 5:00 PM
100 AI-in-IPC studies (2014-24) found: 75% ML use; 53% predictive analytics; 15% integrated tools. Barriers: data quality (45%), tech issues (16%). Risks: operational (35%), technical (33%). 🤖🦠📊##idsky
Reposted by Ken Koon Wong
Reposted by Ken Koon Wong
Five subphenotypes of Staphylococcus aureus bacteremia (SAB) were identified in diverse cohorts: 40.2% had MRSA. 90-day mortality was highest in subphenotype A. 🦠💔##idsky
Reproducible identification of Staphylococcus aureus bacteremia clinical subphenotypes
Clinical heterogeneity in Staphylococcus aureus bacteremia (SAB) complicates clinical management and research. We have previously identified five clinically distinct subphenotypes of SAB associated with differences in outcomes and response to adjunctive rifampicin. Here, we aimed to identify these subphenotypes in geographically diverse observational cohorts, including a higher prevalence of methicillin-resistant S. aureus (MRSA) bacteremia and the USA300 clone.MethodsWe studied three cohorts of adults with SAB from observational studies: a UK retrospective study (Edinburgh cohort 2, n=463); a Dutch prospective study (IDISA, n=490); and a USA prospective study (SABG-PCS, n=755). Subphenotypes were identified from routinely available clinical data using latent class analysis.ResultsPatients from the SABG-PCS cohort had greater multimorbidity and more MRSA bacteremia (40.2%, 303/755), including infection with the USA300 clone (14.7%, 111/755). Five distinct subphenotypes were identified in each cohort: (A) older age and cardio-metabolic multimorbidity; (B) nosocomial acquisition and intravenous catheter portal of entry; (C) community acquisition and metastatic infection; (D) chronic kidney disease; and (E) younger age, injection drug use, and metastatic infection. Bacterial genotypes varied substantially between the Edinburgh 2 and SABG-PCS cohorts but did not differ between subphenotypes within each cohort. 90-day mortality was highest in subphenotype A, and persistent bacteremia in subphenotypes C and E.ConclusionsWe have reproducibly identified five clinical subphenotypes of SAB in observational cohorts including diverse bacterial genetic lineages and a cohort with a high prevalence of MRSA and USA300 bacteremia. These robustly reproducible clinical subphenotypes provide a framework to rationalize the heterogeneity intrinsic to SAB.
academic.oup.com
November 27, 2025 at 11:30 PM
Five subphenotypes of Staphylococcus aureus bacteremia (SAB) were identified in diverse cohorts: 40.2% had MRSA. 90-day mortality was highest in subphenotype A. 🦠💔##idsky
Reposted by Ken Koon Wong
Study on VGEI in 97 rats showed FDG-PET could differentiate untreated S. aureus infections but not monitor progression. SUVmax declined over time despite constant bacterial load. 📉🦠##idsky
[18F]Fluorodeoxyglucose Positron Emission Tomography for diagnosis and monitoring of acute Staphylococcus aureus vascular graft infection in a rat model
AbstractObjectivesVascular graft or endograft infections (VGEI) pose a detrimental complication when using vascular grafts and are challenging to diagnose and treat. This study examined the progression of infection and the antimicrobial response in VGEI using [18F]Fluorodeoxyglucose (FDG) Positron Emission Tomography (PET), ex vivo bacterial quantification, and histology in a VGEI rat model.MethodsIn this experimental study, 97 male Sprague-Dawley rats had a polytetrafluorethylene graft surgically implanted in the carotid artery. The graft was either pre-inoculated with Staphylococcus aureus, Staphylococcus epidermidis, or saline. Up to 31 days after surgery, rats were FDG-PET-scanned. Subsequently, they were euthanised, and the implants were retrieved for analysis. A subgroup of infected rats received daptomycin and rifampicin from days 20 to 29.ResultsTracer uptake around the implant, measured by maximum standardised uptake value (SUVmax), declined over time in all groups. Between groups, SUVmax was highest in untreated S. aureus-infected rats. When comparing antibiotic-treated and uninfected rats by day 31, there was no difference in SUVmax, although the treated rats were still infected.Histology revealed widespread inflammation by day 10 in S. aureus-infected rats, which decreased by days 20 and 31 with encapsulation of the infection, alongside increased plasma interleukin-10.ConclusionsFDG-PET differentiated untreated S. aureus-infected rats from uninfected ones but failed to monitor infection progression, as SUVmax declined over time despite a constant bacterial load.FDG-PET could not distinguish between uninfected rats and those with suppressed infection, likely due to reduced inflammation and encapsulation of the infection.
academic.oup.com
November 27, 2025 at 1:30 PM
Study on VGEI in 97 rats showed FDG-PET could differentiate untreated S. aureus infections but not monitor progression. SUVmax declined over time despite constant bacterial load. 📉🦠##idsky
Reposted by Ken Koon Wong
Study of 336 PABSI patients: 30.1% had 90-day mortality. No difference in outcomes based on gallbladder presence. Liver disease linked to higher mortality. Antimicrobial resistance similar in both groups.##idsky
Impact of Remote Cholecystectomy on Clinical Outcomes Following Pseudomonas aeruginosa Bloodstream Infection
Mortality associated with Pseudomonas aeruginosa bloodstream infection (PABSI) remains high despite advances in clinical care and therapeutics. In a recent study using a mouse model of PABSI, the gallbladder was identified as a reservoir for bacterial expansion. Furthermore, bile exposure has been linked to increased antimicrobial resistance. Therefore, we asked whether patients with retained gallbladders might experience more antimicrobial-resistant PABSIs, extended culture positivity, and worsened clinical outcomes.MethodsWe conducted a retrospective cohort study of adults hospitalized over a 5-year period with PABSI. PABSI cases were defined as patients with ≥1 positive P. aeruginosa bacterial culture from the blood. Patients were categorized as those retaining a gallbladder (no cholecystectomy) or not (cholecystectomy). Cholecystectomy was defined as a history of cholecystectomy ≥1 year prior to the index episode of PABSI. Inferential statistics were used to identify associations between remote cholecystectomy and antimicrobial resistance profile, length of blood culture positivity, and in-hospital and 90-day mortality.ResultsThe overall study population included 336 patients: 262 (78%) with a retained gallbladder and 74 (22%) without. Using the entire study population and a matched cohort, we observed no difference in length of culture positivity, 90-day mortality, or in-hospital mortality between groups based on the presence of a gallbladder. Overall, composite 90-day mortality was 30.1%, which was similar to a prior investigation of PABSI outcomes at our institution. While the presence of a gallbladder did not affect the outcome, patients with PABSI and liver disease had significantly higher 90-day mortality than those without liver disease. Furthermore, no robust differences were observed in the antimicrobial resistance profile of P. aeruginosa isolates from the group with or without a gallbladder.ConclusionsIn our study, neither PABSI antimicrobial resistance pattern nor clinical outcomes were affected by remote cholecystectomy. However, we do demonstrate that mortality for patients with PABSI in the modern era remains high despite advances in antipseudomonal therapeutics.
academic.oup.com
November 27, 2025 at 2:30 AM
Study of 336 PABSI patients: 30.1% had 90-day mortality. No difference in outcomes based on gallbladder presence. Liver disease linked to higher mortality. Antimicrobial resistance similar in both groups.##idsky
Reposted by Ken Koon Wong
Febrile neutropenia poses risks for patients with hematological malignancies. The 10th European Conference recommends personalized treatment based on local resistance patterns. Empirical monotherapy is advised in low-resistance settings.##idsky
[Review] Empirical and targeted antimicrobial therapy in patients with febrile neutropenia and haematological malignancy or after haematopoietic cell transplantation: recommendations from the 10th European Conference on Infections in Leukaemia
Febrile neutropenia can lead to life-threatening infections in patients with haematological malignancies or after hematopoietic cell transplantation. Infection management is challenged by rising antibiotic resistance and regional differences in bacterial epidemiology. The 10th European Conference on Infections in Leukaemia panel recommends a personalised approach guided by local resistance patterns and individual risk factors. For patients who are haemodynamically stable without colonisation or infection by resistant Gram-negative bacteria in low-resistance prevalence settings, empirical monotherapy sparing carbapenems or novel β-lactams with or without β-lactamase inhibitors (BLI) is recommended.
www.thelancet.com
November 26, 2025 at 12:00 PM
Febrile neutropenia poses risks for patients with hematological malignancies. The 10th European Conference recommends personalized treatment based on local resistance patterns. Empirical monotherapy is advised in low-resistance settings.##idsky
Reposted by Ken Koon Wong
Kleb4V, a tetravalent vaccine for antibiotic-resistant K. pneumoniae, was tested on 166 adults. It was well tolerated, showing strong immune responses for 3 of 4 serotypes. 💉✨##idsky
Safety and immunogenicity of a Klebsiella pneumoniae tetravalent bioconjugate vaccine (Kleb4V) administered to healthy adults: A first time in human phase I/II randomised and controlled study
Safe and effective vaccines are urgently needed to prevent infections caused by Klebsiella pneumoniae (K. pneumoniae), one of the most common antibiotic-resistant pathogens. We aimed to assess the safety and immunogenicity of a tetravalent bioconjugate vaccine Kleb4V, containing O antigen-polysaccharides of the most predominant K. pneumoniae serotypes (O1v1, O2a, O2afg and O3b).MethodsIn this observer-blind, randomised, placebo-controlled, phase I/II trial [ClinicalTrials.gov (number NCT04959344)], 166 healthy adults (18-40y n=16, 55-70y n=150) were enrolled and randomised to receive two intramuscular injections of Kleb4V (16μg or 64μg of total O-antigen +/- adjuvant AS03) or placebo on days 1 and 57. While the primary outcome was safety, the secondary outcomes included vaccine antigen immunogenicity.ResultsKleb4V was well tolerated, with most solicited and unsolicited AEs of mild to moderate intensity. Kleb4V was immunogenic for all four vaccine-serotypes at both antigen doses. O1v1, O2a and O2afg specific IgG increased two weeks after the 1st vaccination and the immune response persisted at six months after the second vaccination. For three of the four vaccine-serotypes, the AS03-adjuvanted formulations showed a superior immune response. O3b responses were reduced compared to the other vaccine antigens.DiscussionKleb4V is the first K. pneumoniae conjugate vaccine candidate to reach clinical assessment. The Kleb4V bioconjugate was immunogenic, well tolerated and with an acceptable safety profile in the target population of adults aged 55-70 years for all 4 vaccine-serotypes.
academic.oup.com
November 27, 2025 at 12:30 AM
Kleb4V, a tetravalent vaccine for antibiotic-resistant K. pneumoniae, was tested on 166 adults. It was well tolerated, showing strong immune responses for 3 of 4 serotypes. 💉✨##idsky
Reposted by Ken Koon Wong
In a phase 2a, randomized trial, oral treatment with high-dose mosnodenvir, a pan–DENV serotype antiviral drug, led to a significantly lower DENV-3 RNA load than placebo after challenge in a controlled human infection model. Full trial results: nej.md/48eUJwJ
#MedSky #IDSky
#MedSky #IDSky

November 26, 2025 at 10:10 PM
In a phase 2a, randomized trial, oral treatment with high-dose mosnodenvir, a pan–DENV serotype antiviral drug, led to a significantly lower DENV-3 RNA load than placebo after challenge in a controlled human infection model. Full trial results: nej.md/48eUJwJ
#MedSky #IDSky
#MedSky #IDSky