




Willy Frick
@willyhfrick.bsky.social
Heart rhythm fellow. Medical educator. ECG enthusiast.
Associate Editor of Dr. Smith's ECG Blog: https://drsmithsecgblog.com
Associate Editor of Dr. Smith's ECG Blog: https://drsmithsecgblog.com
Do #EPeeps believe in AVNRT upper common pathway (block)?
This patient had:
1. AH jump
2. Septal VA < 80 ms
3. Concentric A during SVT
4. During RVP: (Stim-A)-(V-A) > 85 ms
5. During RVP: PPI-TCL > 115 ms
6. SVT terminated by RV burst pacing
7. Ablation in TOK rendered non-inducible
This patient had:
1. AH jump
2. Septal VA < 80 ms
3. Concentric A during SVT
4. During RVP: (Stim-A)-(V-A) > 85 ms
5. During RVP: PPI-TCL > 115 ms
6. SVT terminated by RV burst pacing
7. Ablation in TOK rendered non-inducible

October 21, 2025 at 1:43 AM
Do #EPeeps believe in AVNRT upper common pathway (block)?
This patient had:
1. AH jump
2. Septal VA < 80 ms
3. Concentric A during SVT
4. During RVP: (Stim-A)-(V-A) > 85 ms
5. During RVP: PPI-TCL > 115 ms
6. SVT terminated by RV burst pacing
7. Ablation in TOK rendered non-inducible
This patient had:
1. AH jump
2. Septal VA < 80 ms
3. Concentric A during SVT
4. During RVP: (Stim-A)-(V-A) > 85 ms
5. During RVP: PPI-TCL > 115 ms
6. SVT terminated by RV burst pacing
7. Ablation in TOK rendered non-inducible
Arrhythmogenic cardiomyopathy, epicardial access. Pacing from ablator.
@narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @danacjohnson.medsky.social
#EPeeps
@narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @danacjohnson.medsky.social
#EPeeps

October 17, 2025 at 5:09 PM
Arrhythmogenic cardiomyopathy, epicardial access. Pacing from ablator.
@narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @danacjohnson.medsky.social
#EPeeps
@narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @danacjohnson.medsky.social
#EPeeps

June 20, 2025 at 9:55 PM

June 17, 2025 at 4:47 PM
Does the constancy of the PVC coupling interval suggest triggered mechanism?
#ECGSky #MedSky #CardioSky
@jeffreyvinocur.bsky.social @narrowqrs.bsky.social @shah.md @danacjohnson.medsky.social @daverichley.bsky.social @alexturinmd.bsky.social
#ECGSky #MedSky #CardioSky
@jeffreyvinocur.bsky.social @narrowqrs.bsky.social @shah.md @danacjohnson.medsky.social @daverichley.bsky.social @alexturinmd.bsky.social

June 11, 2025 at 3:42 AM
Does the constancy of the PVC coupling interval suggest triggered mechanism?
#ECGSky #MedSky #CardioSky
@jeffreyvinocur.bsky.social @narrowqrs.bsky.social @shah.md @danacjohnson.medsky.social @daverichley.bsky.social @alexturinmd.bsky.social
#ECGSky #MedSky #CardioSky
@jeffreyvinocur.bsky.social @narrowqrs.bsky.social @shah.md @danacjohnson.medsky.social @daverichley.bsky.social @alexturinmd.bsky.social
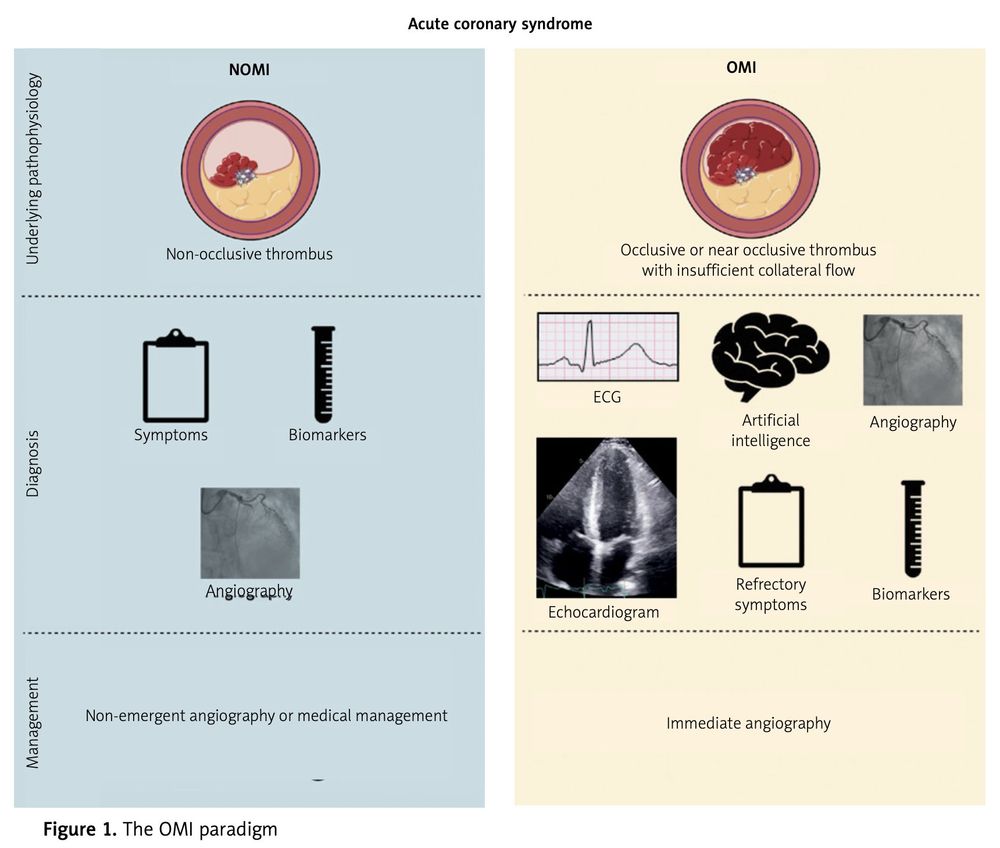
Read our editorial at the link below!
www.termedia.pl/Occlusion-my...
#ECGSky #Medsky #cardiosky
@ecgcases.bsky.social
www.termedia.pl/Occlusion-my...
#ECGSky #Medsky #cardiosky
@ecgcases.bsky.social
June 3, 2025 at 8:58 PM
Read our editorial at the link below!
www.termedia.pl/Occlusion-my...
#ECGSky #Medsky #cardiosky
@ecgcases.bsky.social
www.termedia.pl/Occlusion-my...
#ECGSky #Medsky #cardiosky
@ecgcases.bsky.social
I also saw the rhythm start and stop with PVCs.

May 14, 2025 at 9:00 PM
I also saw the rhythm start and stop with PVCs.
And this? Premature but with unchanged morphology. Concealed fusion with nearby PVC? Wobble feels unsatisfactory since cycle length is otherwise stable.
@narrowqrs.bsky.social @danacjohnson.medsky.social @shah.md @jeffreyvinocur.bsky.social @alexturinmd.bsky.social @daverichley.bsky.social
Help.
@narrowqrs.bsky.social @danacjohnson.medsky.social @shah.md @jeffreyvinocur.bsky.social @alexturinmd.bsky.social @daverichley.bsky.social
Help.

May 14, 2025 at 2:06 PM
And this? Premature but with unchanged morphology. Concealed fusion with nearby PVC? Wobble feels unsatisfactory since cycle length is otherwise stable.
@narrowqrs.bsky.social @danacjohnson.medsky.social @shah.md @jeffreyvinocur.bsky.social @alexturinmd.bsky.social @daverichley.bsky.social
Help.
@narrowqrs.bsky.social @danacjohnson.medsky.social @shah.md @jeffreyvinocur.bsky.social @alexturinmd.bsky.social @daverichley.bsky.social
Help.
60M with severe ischemic cardiomyopathy, prior inferoposterior OMI.
Overall impression is VT with fusion complexes. But...fusion with what? I thought supraventricular capture at first, but I am leaning more toward fusion with unrelated PVCs now.
Overall impression is VT with fusion complexes. But...fusion with what? I thought supraventricular capture at first, but I am leaning more toward fusion with unrelated PVCs now.

May 14, 2025 at 2:06 PM
60M with severe ischemic cardiomyopathy, prior inferoposterior OMI.
Overall impression is VT with fusion complexes. But...fusion with what? I thought supraventricular capture at first, but I am leaning more toward fusion with unrelated PVCs now.
Overall impression is VT with fusion complexes. But...fusion with what? I thought supraventricular capture at first, but I am leaning more toward fusion with unrelated PVCs now.
I can't figure out an elegant explanation for the intermittent aberrancy.
Anyone?
#ECGsky #Medsky #cardiosky #EPeeps
Anyone?
#ECGsky #Medsky #cardiosky #EPeeps

April 25, 2025 at 10:33 PM
I can't figure out an elegant explanation for the intermittent aberrancy.
Anyone?
#ECGsky #Medsky #cardiosky #EPeeps
Anyone?
#ECGsky #Medsky #cardiosky #EPeeps
Discussed with some rhythm friends, not everyone is convinced by superconduction. Thoughts?
Including a prior sinus-ish tracing for comparison.
@danacjohnson.medsky.social @narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @alexturinmd.bsky.social @daverichley.bsky.social
Including a prior sinus-ish tracing for comparison.
@danacjohnson.medsky.social @narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @alexturinmd.bsky.social @daverichley.bsky.social

April 13, 2025 at 6:33 PM
Discussed with some rhythm friends, not everyone is convinced by superconduction. Thoughts?
Including a prior sinus-ish tracing for comparison.
@danacjohnson.medsky.social @narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @alexturinmd.bsky.social @daverichley.bsky.social
Including a prior sinus-ish tracing for comparison.
@danacjohnson.medsky.social @narrowqrs.bsky.social @shah.md @jeffreyvinocur.bsky.social @alexturinmd.bsky.social @daverichley.bsky.social
My interpretation: Reverse typical flutter with dual level AVB as shown. Native complexes conduct with LAFB. R2 is Ashman beat. R4, R6 with superconduction through LAF. R8 unclear? Possible superconduction through a subdivision of LAF?

April 13, 2025 at 6:33 PM
My interpretation: Reverse typical flutter with dual level AVB as shown. Native complexes conduct with LAFB. R2 is Ashman beat. R4, R6 with superconduction through LAF. R8 unclear? Possible superconduction through a subdivision of LAF?

April 12, 2025 at 7:15 PM
Overhead page code blue. You arrive bedside to find ongoing chest compressions. First pulse check, you see this.
What next?
#cardiosky
What next?
#cardiosky

April 7, 2025 at 2:25 AM
Overhead page code blue. You arrive bedside to find ongoing chest compressions. First pulse check, you see this.
What next?
#cardiosky
What next?
#cardiosky
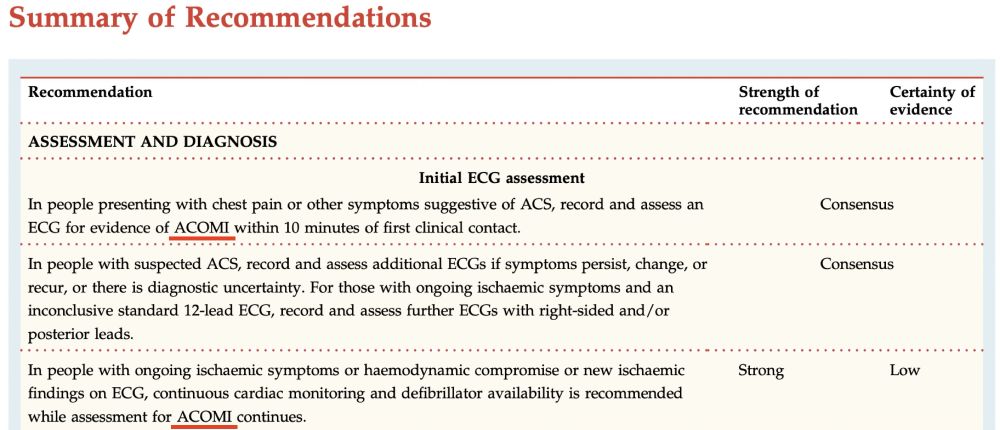
Glad to see the Australian guidelines reflect the data where American guidelines (@accintouch.bsky.social) were stuck in an antiquated era.
The best time to move on from STEMI was years ago. The second best time is now.
www.heartfoundation.org.au/for-professi...
#medsky #cardiosky #ECGsky
The best time to move on from STEMI was years ago. The second best time is now.
www.heartfoundation.org.au/for-professi...
#medsky #cardiosky #ECGsky
April 6, 2025 at 1:17 PM
Glad to see the Australian guidelines reflect the data where American guidelines (@accintouch.bsky.social) were stuck in an antiquated era.
The best time to move on from STEMI was years ago. The second best time is now.
www.heartfoundation.org.au/for-professi...
#medsky #cardiosky #ECGsky
The best time to move on from STEMI was years ago. The second best time is now.
www.heartfoundation.org.au/for-professi...
#medsky #cardiosky #ECGsky
Fred W. Frick, MD FACP, inducted 2000
William H. Frick, MD FACP, inducted 2025
@acpimphysicians.bsky.social
William H. Frick, MD FACP, inducted 2025
@acpimphysicians.bsky.social

April 4, 2025 at 2:21 AM
Fred W. Frick, MD FACP, inducted 2000
William H. Frick, MD FACP, inducted 2025
@acpimphysicians.bsky.social
William H. Frick, MD FACP, inducted 2025
@acpimphysicians.bsky.social
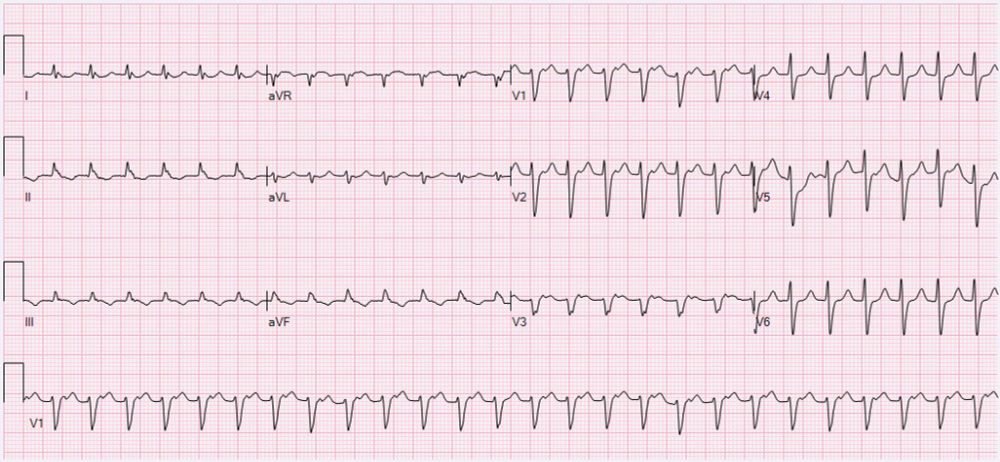
Tough ECG. This is dextrocardia with quadrigeminal PVC fusion.
Patient also has hypertrophy of the systemic ventricle (anatomically, the RV since dextrocardia) which is why it doesn’t look like “usual” dextrocardia. There is hypertrophy repolarization abnormality.
Patient also has hypertrophy of the systemic ventricle (anatomically, the RV since dextrocardia) which is why it doesn’t look like “usual” dextrocardia. There is hypertrophy repolarization abnormality.

April 1, 2025 at 10:20 PM
Tough ECG. This is dextrocardia with quadrigeminal PVC fusion.
Patient also has hypertrophy of the systemic ventricle (anatomically, the RV since dextrocardia) which is why it doesn’t look like “usual” dextrocardia. There is hypertrophy repolarization abnormality.
Patient also has hypertrophy of the systemic ventricle (anatomically, the RV since dextrocardia) which is why it doesn’t look like “usual” dextrocardia. There is hypertrophy repolarization abnormality.

April 1, 2025 at 12:58 AM
New update just dropped in the coronary anomalies section!

March 15, 2025 at 5:41 PM
New update just dropped in the coronary anomalies section!
But hard to argue RV failure when wedge is high and RA is not. This is pre Impella.

March 8, 2025 at 11:00 PM
But hard to argue RV failure when wedge is high and RA is not. This is pre Impella.
Agree RP could've been considered. She was hemodynamically stable until she wasn't and family asked for cessation of resuscitation efforts.
RHC tracings attached.
RHC tracings attached.




March 8, 2025 at 11:00 PM
Agree RP could've been considered. She was hemodynamically stable until she wasn't and family asked for cessation of resuscitation efforts.
RHC tracings attached.
RHC tracings attached.
It looks like VT to me, are we seeing 2:1 VA conduction?

March 7, 2025 at 3:04 AM
It looks like VT to me, are we seeing 2:1 VA conduction?
I accidentally posted the hard version of this! Although MUSE gives V1 rhythm strip by default, I changed it to lead I when I was reviewing since there was less artifact.
Lead I shows sinus bradycardia with PACs and interatrial block.
Lead I shows sinus bradycardia with PACs and interatrial block.

February 10, 2025 at 10:32 PM
I accidentally posted the hard version of this! Although MUSE gives V1 rhythm strip by default, I changed it to lead I when I was reviewing since there was less artifact.
Lead I shows sinus bradycardia with PACs and interatrial block.
Lead I shows sinus bradycardia with PACs and interatrial block.

February 5, 2025 at 8:50 PM
Prior ECG shows manifest pre-excitation.
Telemetry shows LOSS of pre-excitation at tachycardia onset indicating exclusive ventricular activation via AVN (since the accessory pathway is the retrograde limb of the circuit).
Diagnosis: orthodromic reciprocating tachycardia
Telemetry shows LOSS of pre-excitation at tachycardia onset indicating exclusive ventricular activation via AVN (since the accessory pathway is the retrograde limb of the circuit).
Diagnosis: orthodromic reciprocating tachycardia


February 5, 2025 at 8:19 PM
Prior ECG shows manifest pre-excitation.
Telemetry shows LOSS of pre-excitation at tachycardia onset indicating exclusive ventricular activation via AVN (since the accessory pathway is the retrograde limb of the circuit).
Diagnosis: orthodromic reciprocating tachycardia
Telemetry shows LOSS of pre-excitation at tachycardia onset indicating exclusive ventricular activation via AVN (since the accessory pathway is the retrograde limb of the circuit).
Diagnosis: orthodromic reciprocating tachycardia