



Project for Universal Management of Airways
@universalairway.org
PUMA is a global collaboration to produce universal guidelines for airway management that can be applied independent of geography, discipline or context.
Reposted by Project for Universal Management of Airways

International Consensus Guidelines for Preventing Unrecognised Oesophageal Intubation.
Free full text in @anaesjournal.bsky.social
Supported by @dasairway.bsky.social @safeairwaysociety.org @asahq.bsky.social @rcoanews.bsky.social & many more…
www.universalairway.org/puoi/support
Free full text in @anaesjournal.bsky.social
Supported by @dasairway.bsky.social @safeairwaysociety.org @asahq.bsky.social @rcoanews.bsky.social & many more…
www.universalairway.org/puoi/support
September 1, 2025 at 5:45 AM
International Consensus Guidelines for Preventing Unrecognised Oesophageal Intubation.
Free full text in @anaesjournal.bsky.social
Supported by @dasairway.bsky.social @safeairwaysociety.org @asahq.bsky.social @rcoanews.bsky.social & many more…
www.universalairway.org/puoi/support
Free full text in @anaesjournal.bsky.social
Supported by @dasairway.bsky.social @safeairwaysociety.org @asahq.bsky.social @rcoanews.bsky.social & many more…
www.universalairway.org/puoi/support
Reposted by Project for Universal Management of Airways

The Safe Airway Liaison Group in the UK have released a statement on displaying the waveform capnography trace in line with the @universalairway.org recommendations. The CO2 trace should be:
1. The bottom trace
2. White
3. Shaded in
www.salg.ac.uk/salg-publica...
1. The bottom trace
2. White
3. Shaded in
www.salg.ac.uk/salg-publica...
SALG | SALG Statement on Waveform Capnography
www.salg.ac.uk
August 14, 2025 at 6:21 PM
The Safe Airway Liaison Group in the UK have released a statement on displaying the waveform capnography trace in line with the @universalairway.org recommendations. The CO2 trace should be:
1. The bottom trace
2. White
3. Shaded in
www.salg.ac.uk/salg-publica...
1. The bottom trace
2. White
3. Shaded in
www.salg.ac.uk/salg-publica...
Reposted by Project for Universal Management of Airways
The @universalairway.org guidelines for preventing unrecognised oesophageal intubation are supported by @safeairwaysociety.org, @anzca.bsky.social & @dasairway.bsky.social
VL should be used routinely whenever feasible.
Clinical signs should not be used to exclude oesophageal intubation.
VL should be used routinely whenever feasible.
Clinical signs should not be used to exclude oesophageal intubation.


August 14, 2025 at 6:33 PM
The @universalairway.org guidelines for preventing unrecognised oesophageal intubation are supported by @safeairwaysociety.org, @anzca.bsky.social & @dasairway.bsky.social
VL should be used routinely whenever feasible.
Clinical signs should not be used to exclude oesophageal intubation.
VL should be used routinely whenever feasible.
Clinical signs should not be used to exclude oesophageal intubation.
Reposted by Project for Universal Management of Airways

🚨We have retired "no trace, wrong place" to align with PUMA guidelines.
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
August 14, 2025 at 12:14 PM
🚨We have retired "no trace, wrong place" to align with PUMA guidelines.
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
Instead, with @assocanaes.bsky.social and @dasairway.bsky.social, our message is that if sustained exhaled CO2 is not detected, then oesophageal intubation must be ruled out.
See our dedicated webpage👉 ow.ly/vOZs50WA03r
Reposted by Project for Universal Management of Airways
3-step guide to mastering #HAVL from @cliffreid.bsky.social
1. Watch the video
m.youtube.com/watch?v=aYo7...
2. Read the stepwise guide
drive.google.com/file/d/14r_W...
3. Deliberate team practice
(rinse & repeat)
1. Watch the video
m.youtube.com/watch?v=aYo7...
2. Read the stepwise guide
drive.google.com/file/d/14r_W...
3. Deliberate team practice
(rinse & repeat)

July 27, 2025 at 10:34 PM
3-step guide to mastering #HAVL from @cliffreid.bsky.social
1. Watch the video
m.youtube.com/watch?v=aYo7...
2. Read the stepwise guide
drive.google.com/file/d/14r_W...
3. Deliberate team practice
(rinse & repeat)
1. Watch the video
m.youtube.com/watch?v=aYo7...
2. Read the stepwise guide
drive.google.com/file/d/14r_W...
3. Deliberate team practice
(rinse & repeat)
Reposted by Project for Universal Management of Airways
International consensus guidelines for preventing unrecognised oesophageal intubation from @universalairway.org

Preventing unrecognised oesophageal intubation: a consensus guideline from the Project for Universal Management of Airways and international airway societies*
Across multiple disciplines undertaking airway management globally, preventable episodes of unrecognised oesophageal intubation result in profound hypoxaemia, brain injury and death. These events occ...
associationofanaesthetists-publications.onlinelibrary.wiley.com
July 27, 2025 at 8:42 PM
International consensus guidelines for preventing unrecognised oesophageal intubation from @universalairway.org
The Project for Universal Management of Airways (PUMA) will no longer post on Twitter.
Join us
#Xodus
Join us
#Xodus
How about some more medical-related organisations make an ethical stand and abandon Twitter? If you're still posting there you're part of the problem. Trust your followers to come with you.
@dasairway.bsky.social @anaesjournal.bsky.social @bjajournals.bsky.social @rcoanews.bsky.social
@dasairway.bsky.social @anaesjournal.bsky.social @bjajournals.bsky.social @rcoanews.bsky.social
July 27, 2025 at 2:34 AM
The Project for Universal Management of Airways (PUMA) will no longer post on Twitter.
Join us
#Xodus
Join us
#Xodus
Reposted by Project for Universal Management of Airways

Airway assistant (ala airway ally) litfl.com/airway-assis... the forgotten role in airway management in ED, ICU, and the wards… but an important one! #foamed #foamcc

Airway Assistant
Description of the airway assistant role in the ANZ critical care setting: responsibilities, tips, pitfalls for newcomers to the role
litfl.com
July 17, 2025 at 10:31 PM
Airway assistant (ala airway ally) litfl.com/airway-assis... the forgotten role in airway management in ED, ICU, and the wards… but an important one! #foamed #foamcc
Reposted by Project for Universal Management of Airways
Unrecognised esophageal intubation litfl.com/unrecognised... Largely derived from the superb PUMA guidelines by @chrimesy.com et al #foamed #foamcc
Unrecognised oesophageal intubation
Unrecognised oesophageal intubation: frequency, causes, prevention, recognition, actions, and confounders. Derived from PUMA guidelines.
litfl.com
July 17, 2025 at 10:29 PM
Unrecognised esophageal intubation litfl.com/unrecognised... Largely derived from the superb PUMA guidelines by @chrimesy.com et al #foamed #foamcc
Reposted by Project for Universal Management of Airways
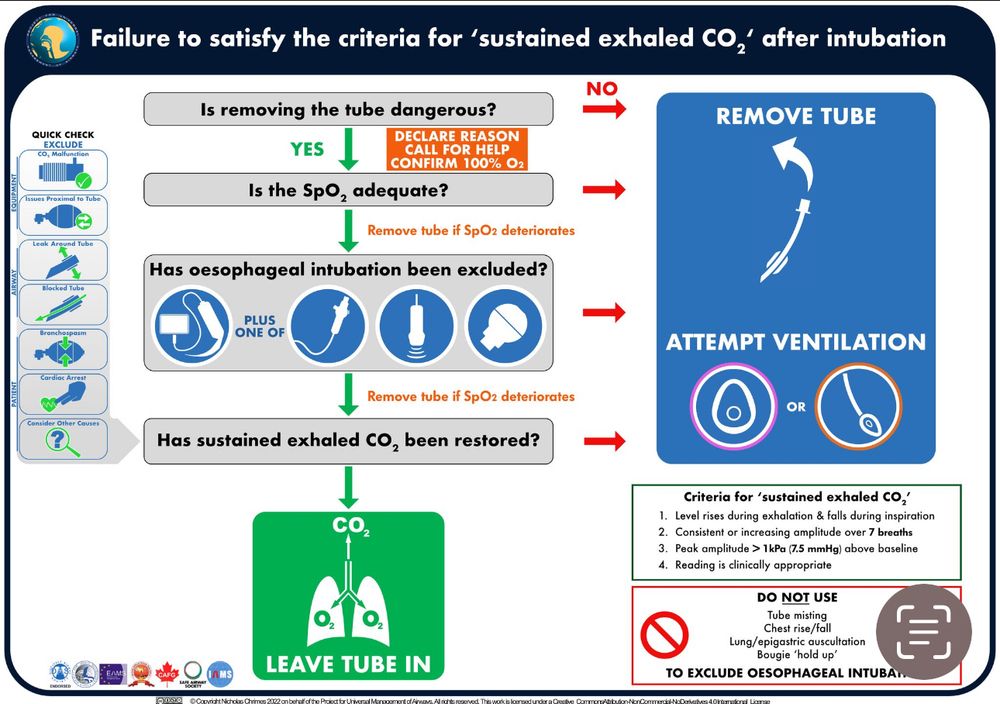
Key points:
1. ALWAYS confirm criteria for sustained exhaled CO2 are satisfied.
2. NEVER use clinical signs to exclude oesophageal intubation
3. The fastest, simplest & most definitive way to exclude oesophageal intubation is to remove the tube AND ventilate with an alternate device.
1. ALWAYS confirm criteria for sustained exhaled CO2 are satisfied.
2. NEVER use clinical signs to exclude oesophageal intubation
3. The fastest, simplest & most definitive way to exclude oesophageal intubation is to remove the tube AND ventilate with an alternate device.
June 19, 2025 at 6:44 PM
Key points:
1. ALWAYS confirm criteria for sustained exhaled CO2 are satisfied.
2. NEVER use clinical signs to exclude oesophageal intubation
3. The fastest, simplest & most definitive way to exclude oesophageal intubation is to remove the tube AND ventilate with an alternate device.
1. ALWAYS confirm criteria for sustained exhaled CO2 are satisfied.
2. NEVER use clinical signs to exclude oesophageal intubation
3. The fastest, simplest & most definitive way to exclude oesophageal intubation is to remove the tube AND ventilate with an alternate device.
Organisations supporting the 'Consensus guidelines for preventing unrecognised oesophageal intubation' incl both @anzca.bsky.social and @rcoanews.bsky.social.
Guidelines free full text in @anaesjournal.bsky.social:
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/...
Guidelines free full text in @anaesjournal.bsky.social:
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/...
Preventing unrecognised oesophageal intubation: a consensus guideline from the Project for Universal Management of Airways and international airway societies*
Across multiple disciplines undertaking airway management globally, preventable episodes of unrecognised oesophageal intubation result in profound hypoxaemia, brain injury and death. These events occ....
associationofanaesthetists-publications.onlinelibrary.wiley.com
June 19, 2025 at 3:03 AM
Organisations supporting the 'Consensus guidelines for preventing unrecognised oesophageal intubation' incl both @anzca.bsky.social and @rcoanews.bsky.social.
Guidelines free full text in @anaesjournal.bsky.social:
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/...
Guidelines free full text in @anaesjournal.bsky.social:
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/10.1111/...
Reposted by Project for Universal Management of Airways
But do patients at risk of aspiration need “a tube stuck in quickly”? It’s unlikely there’s actually a proportional incr in asp risk the longer the airway is unprotected. I’d suggest that regurg/asp mainly occurs w change in m tone at induction or w instrumentation while inadeq anaesthetised/relaxed
June 4, 2025 at 3:10 PM
But do patients at risk of aspiration need “a tube stuck in quickly”? It’s unlikely there’s actually a proportional incr in asp risk the longer the airway is unprotected. I’d suggest that regurg/asp mainly occurs w change in m tone at induction or w instrumentation while inadeq anaesthetised/relaxed
Reposted by Project for Universal Management of Airways
Aren’t there already things we would do when extubating a patient at incr risk of aspiration?
Rather than being ‘rapid’ they relate to ensuring return of airway reflexes prior to removing tube (awake), potentially decreasing risk of regurg (gastric suction) & aspiration (lat position).
Rather than being ‘rapid’ they relate to ensuring return of airway reflexes prior to removing tube (awake), potentially decreasing risk of regurg (gastric suction) & aspiration (lat position).
June 4, 2025 at 3:26 PM
Aren’t there already things we would do when extubating a patient at incr risk of aspiration?
Rather than being ‘rapid’ they relate to ensuring return of airway reflexes prior to removing tube (awake), potentially decreasing risk of regurg (gastric suction) & aspiration (lat position).
Rather than being ‘rapid’ they relate to ensuring return of airway reflexes prior to removing tube (awake), potentially decreasing risk of regurg (gastric suction) & aspiration (lat position).
Reposted by Project for Universal Management of Airways
But what are the elements of intubation technique you’d encourage to reduce aspiration risk & do any of them relate to the components of RSI?
I’d suggest that it’s more important that a patient is deeply anaesthetised/paralysed before the airway is instrumented than anything relating to rapidity.
I’d suggest that it’s more important that a patient is deeply anaesthetised/paralysed before the airway is instrumented than anything relating to rapidity.
June 4, 2025 at 3:30 PM
But what are the elements of intubation technique you’d encourage to reduce aspiration risk & do any of them relate to the components of RSI?
I’d suggest that it’s more important that a patient is deeply anaesthetised/paralysed before the airway is instrumented than anything relating to rapidity.
I’d suggest that it’s more important that a patient is deeply anaesthetised/paralysed before the airway is instrumented than anything relating to rapidity.
Reposted by Project for Universal Management of Airways
Background reading for this week’s debate - this excellent editorial by @sthjournalclub.bsky.social & Craig Lyons in @anaesjournal.bsky.social
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/epdf/10....
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/epdf/10....
June 4, 2025 at 10:10 AM
Background reading for this week’s debate - this excellent editorial by @sthjournalclub.bsky.social & Craig Lyons in @anaesjournal.bsky.social
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/epdf/10....
associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/epdf/10....
Reposted by Project for Universal Management of Airways
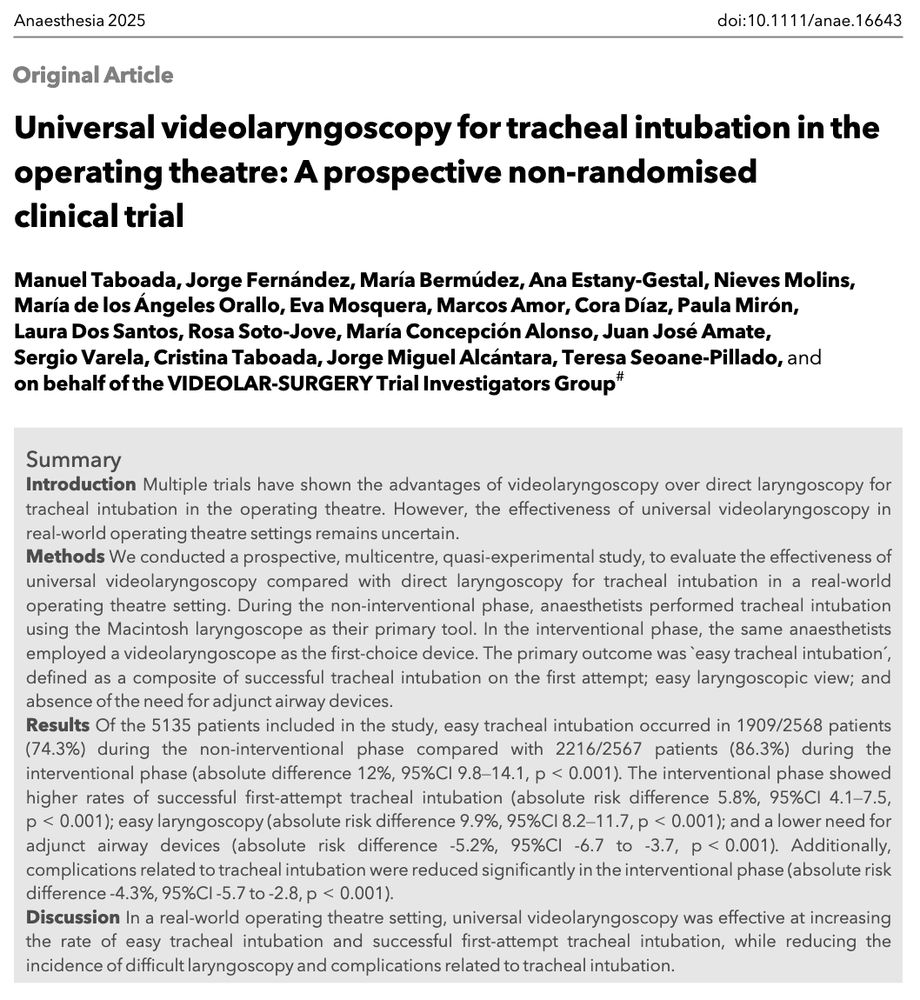
Should we use universal videolaryngoscopy in real-world operating theatre settings?
YES!
↑ rate of easy intubation
↑ rate successful first-attempt intubation
↓ incidence of difficult laryngoscopy
↓ complications related to intubation
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...
YES!
↑ rate of easy intubation
↑ rate successful first-attempt intubation
↓ incidence of difficult laryngoscopy
↓ complications related to intubation
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...


June 3, 2025 at 6:03 AM
Should we use universal videolaryngoscopy in real-world operating theatre settings?
YES!
↑ rate of easy intubation
↑ rate successful first-attempt intubation
↓ incidence of difficult laryngoscopy
↓ complications related to intubation
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...
YES!
↑ rate of easy intubation
↑ rate successful first-attempt intubation
↓ incidence of difficult laryngoscopy
↓ complications related to intubation
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...
Reposted by Project for Universal Management of Airways
In adult patients undergoing tracheal intubation in real-world operating theatre settings, universal VL showed clear advantages over direct laryngoscopy.
This is the largest comparative analysis conducted to date!
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...
This is the largest comparative analysis conducted to date!
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...
June 3, 2025 at 8:06 AM
In adult patients undergoing tracheal intubation in real-world operating theatre settings, universal VL showed clear advantages over direct laryngoscopy.
This is the largest comparative analysis conducted to date!
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...
This is the largest comparative analysis conducted to date!
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...
Reposted by Project for Universal Management of Airways
Brilliant, provocative editorial from @sthjournalclub.bsky.social & Craig Lyons.
While cricoid has been vilified out of existence in some areas by the EBM zealots, there's no evidence for benefit of any other aspect of RSI. Conversely CV compromise & use of rapid-onset NMBAs may cause harm.
While cricoid has been vilified out of existence in some areas by the EBM zealots, there's no evidence for benefit of any other aspect of RSI. Conversely CV compromise & use of rapid-onset NMBAs may cause harm.
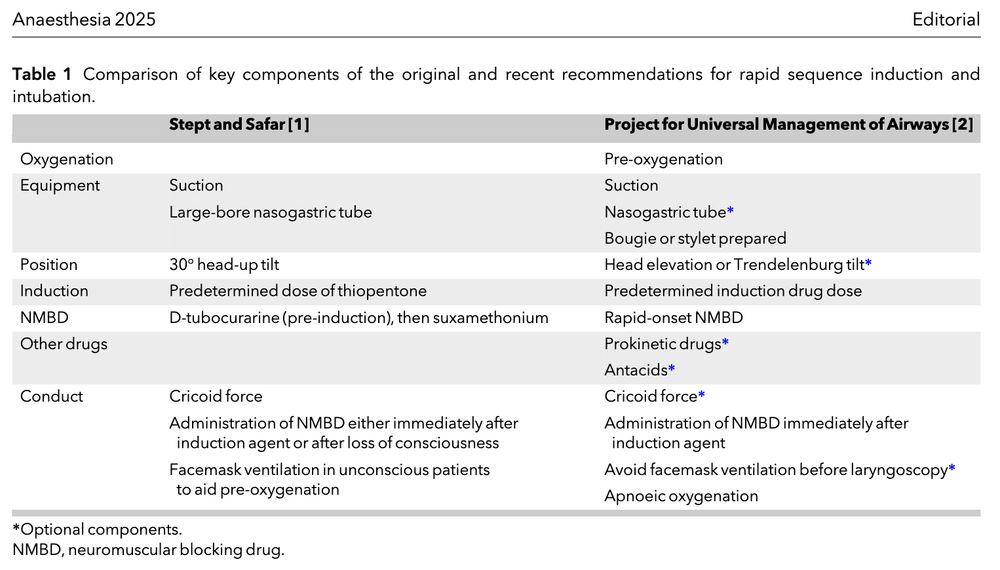
Editorial: Rapid sequence induction: a modern-day example of Theseus' Paradox?
Stept and Safar described ‘rapid induction/intubation’ in 1970.
PUMA recently issued a consensus statement on RSI.
Let's compare.
@sthjournalclub.bsky.social
#AnSky #AirwaySky
doi.org/10.1111/anae...
Stept and Safar described ‘rapid induction/intubation’ in 1970.
PUMA recently issued a consensus statement on RSI.
Let's compare.
@sthjournalclub.bsky.social
#AnSky #AirwaySky
doi.org/10.1111/anae...
May 29, 2025 at 12:27 AM
Brilliant, provocative editorial from @sthjournalclub.bsky.social & Craig Lyons.
While cricoid has been vilified out of existence in some areas by the EBM zealots, there's no evidence for benefit of any other aspect of RSI. Conversely CV compromise & use of rapid-onset NMBAs may cause harm.
While cricoid has been vilified out of existence in some areas by the EBM zealots, there's no evidence for benefit of any other aspect of RSI. Conversely CV compromise & use of rapid-onset NMBAs may cause harm.
Reposted by Project for Universal Management of Airways
Important paper on Airway Leads and implementing comprehensive airway quality improvement process in the Emergency Department from @emcrit.bsky.social
Whether or not you agree w the specific interventions, this should be the template for all airway management programs.
Whether or not you agree w the specific interventions, this should be the template for all airway management programs.


May 31, 2025 at 11:44 PM
Important paper on Airway Leads and implementing comprehensive airway quality improvement process in the Emergency Department from @emcrit.bsky.social
Whether or not you agree w the specific interventions, this should be the template for all airway management programs.
Whether or not you agree w the specific interventions, this should be the template for all airway management programs.
Reposted by Project for Universal Management of Airways
Thio sux is the only classic (but I've never seen it done one, hence all being mRSI).
I think otherwise it ought to be fast acting hypnotic and 1/kg or more of sux or roc. Opioids seem reasonable but I'd be worried about that being your sole "relaxant"
I love www.universalairway.org/rsi above
I think otherwise it ought to be fast acting hypnotic and 1/kg or more of sux or roc. Opioids seem reasonable but I'd be worried about that being your sole "relaxant"
I love www.universalairway.org/rsi above

RSI — Project for Universal Management of Airways
www.universalairway.org
April 19, 2025 at 2:35 PM
Thio sux is the only classic (but I've never seen it done one, hence all being mRSI).
I think otherwise it ought to be fast acting hypnotic and 1/kg or more of sux or roc. Opioids seem reasonable but I'd be worried about that being your sole "relaxant"
I love www.universalairway.org/rsi above
I think otherwise it ought to be fast acting hypnotic and 1/kg or more of sux or roc. Opioids seem reasonable but I'd be worried about that being your sole "relaxant"
I love www.universalairway.org/rsi above
Reposted by Project for Universal Management of Airways
For exactly this reason the @universalairway.org guidelines have removed the term “modified RSI” in favour of a defined spectrum of variations that constitute RSI. Anything outside this is not RSI.
www.universalairway.org/rsi
www.universalairway.org/rsi

RSI — Project for Universal Management of Airways
www.universalairway.org
April 19, 2025 at 7:46 AM
For exactly this reason the @universalairway.org guidelines have removed the term “modified RSI” in favour of a defined spectrum of variations that constitute RSI. Anything outside this is not RSI.
www.universalairway.org/rsi
www.universalairway.org/rsi
Reposted by Project for Universal Management of Airways
It’s extraordinary that this is a case report in 2025.
It’s like publishing a case of a CVC wire being lost intravascularly in which the authors conclude that it might be a good idea to always hold onto the wire.
It’s like publishing a case of a CVC wire being lost intravascularly in which the authors conclude that it might be a good idea to always hold onto the wire.

During hyperangulated #videolaryngoscopy #HAVL the ETT was passed through the soft palate
The authors discuss a ‘blind spot’ of the oropharynx during videolaryngoscopy.
Any thoughts?
buff.ly/L50WWP4
#AnSky #MedSky #AirwaySky #SurgSky #ENTSky
The authors discuss a ‘blind spot’ of the oropharynx during videolaryngoscopy.
Any thoughts?
buff.ly/L50WWP4
#AnSky #MedSky #AirwaySky #SurgSky #ENTSky

April 12, 2025 at 11:18 PM
It’s extraordinary that this is a case report in 2025.
It’s like publishing a case of a CVC wire being lost intravascularly in which the authors conclude that it might be a good idea to always hold onto the wire.
It’s like publishing a case of a CVC wire being lost intravascularly in which the authors conclude that it might be a good idea to always hold onto the wire.
Reposted by Project for Universal Management of Airways
“At least seven respondents reported in the free text comments that UOI could not happen to a competent anaesthetist and that further training was therefore not warranted”
In my experience, the greatest barrier to uptake of the PUOI guidelines is getting clinicians to recognise they need them.
In my experience, the greatest barrier to uptake of the PUOI guidelines is getting clinicians to recognise they need them.

April 13, 2025 at 11:20 AM
“At least seven respondents reported in the free text comments that UOI could not happen to a competent anaesthetist and that further training was therefore not warranted”
In my experience, the greatest barrier to uptake of the PUOI guidelines is getting clinicians to recognise they need them.
In my experience, the greatest barrier to uptake of the PUOI guidelines is getting clinicians to recognise they need them.
Reposted by Project for Universal Management of Airways
But I'm sure you'd agree that's clearly outdated & something the majority of clinicians would disagree with.
In the @universalairway.org guidelines we've defined RSI based on a spectrum of practice that adheres to specific principles.
www.universalairway.org/rsi
In the @universalairway.org guidelines we've defined RSI based on a spectrum of practice that adheres to specific principles.
www.universalairway.org/rsi

RSI — Project for Universal Management of Airways
www.universalairway.org
April 11, 2025 at 1:26 AM
But I'm sure you'd agree that's clearly outdated & something the majority of clinicians would disagree with.
In the @universalairway.org guidelines we've defined RSI based on a spectrum of practice that adheres to specific principles.
www.universalairway.org/rsi
In the @universalairway.org guidelines we've defined RSI based on a spectrum of practice that adheres to specific principles.
www.universalairway.org/rsi
Reposted by Project for Universal Management of Airways
The term "TIVA RSI" misrepresents the issue.
All RSIs are IV. Whether it's a TIVA anaesthetic depends on whether the subseq maintenance agent is inhaled or IV (& irrelevant to the process of RSI).
The question is whether IV induction agents should be administered by an infusion pump during RSI.
All RSIs are IV. Whether it's a TIVA anaesthetic depends on whether the subseq maintenance agent is inhaled or IV (& irrelevant to the process of RSI).
The question is whether IV induction agents should be administered by an infusion pump during RSI.
Do you use TIVA when you are doing a rapid sequence induction in theatre?
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...
#AnSky #AirwaySky #MedSky
doi.org/10.1111/anae...

April 11, 2025 at 12:43 AM
The term "TIVA RSI" misrepresents the issue.
All RSIs are IV. Whether it's a TIVA anaesthetic depends on whether the subseq maintenance agent is inhaled or IV (& irrelevant to the process of RSI).
The question is whether IV induction agents should be administered by an infusion pump during RSI.
All RSIs are IV. Whether it's a TIVA anaesthetic depends on whether the subseq maintenance agent is inhaled or IV (& irrelevant to the process of RSI).
The question is whether IV induction agents should be administered by an infusion pump during RSI.