




Terkild Brink Buus
@terkild.bsky.social
Assistant Professor intrigued by skin immunology, T cell lymphoma, S. aureus-T cell interactions and single-cell analyses at University of Copenhagen @ucph.bsky.social
Glad to see our article on how cancer drugs and bacterial (S. aureus) infections can affect co-existing malignant subclones very differently in cutaneous T-cell lymphoma.
Thank you Cancer Discovery (@aacrjournals.bsky.social) for the beautiful title-page graphics!
Thank you Cancer Discovery (@aacrjournals.bsky.social) for the beautiful title-page graphics!

November 6, 2025 at 10:31 AM
Glad to see our article on how cancer drugs and bacterial (S. aureus) infections can affect co-existing malignant subclones very differently in cutaneous T-cell lymphoma.
Thank you Cancer Discovery (@aacrjournals.bsky.social) for the beautiful title-page graphics!
Thank you Cancer Discovery (@aacrjournals.bsky.social) for the beautiful title-page graphics!
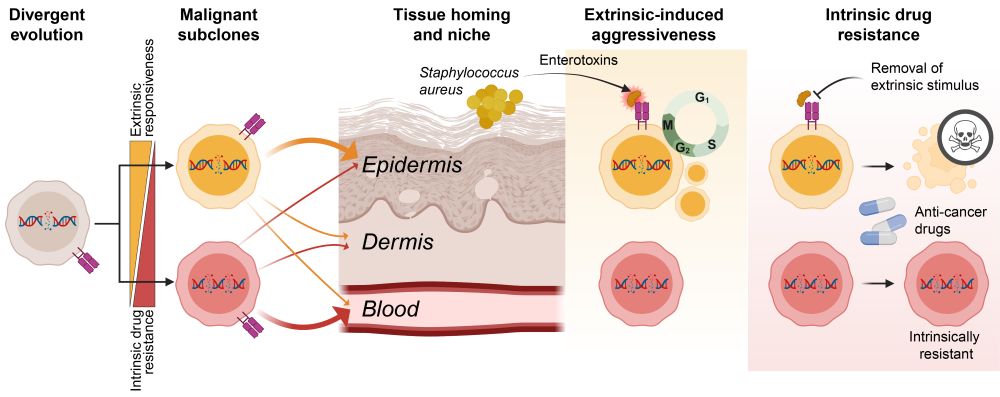
Divergent evolution results in co-existing subclones that have different tissue preferences and respond differently to external factors: cytokines and bacterial infections. The most aggressive subclones are also most sensitive to treatment if stimuli are removed exposing their vulnerabilities. 7/
June 19, 2025 at 11:31 AM
Divergent evolution results in co-existing subclones that have different tissue preferences and respond differently to external factors: cytokines and bacterial infections. The most aggressive subclones are also most sensitive to treatment if stimuli are removed exposing their vulnerabilities. 7/
Here's the trade-off ⚖️: The subclones that respond most strongly to 🦠S. aureus toxins—the aggressive ones—are also the most intrinsically sensitive to 💊anti-cancer drugs when the stimuli are removed.
This means reducing inflammation could unmask therapeutic vulnerabilities in aggressive clones. 6/
This means reducing inflammation could unmask therapeutic vulnerabilities in aggressive clones. 6/

June 19, 2025 at 11:31 AM
Here's the trade-off ⚖️: The subclones that respond most strongly to 🦠S. aureus toxins—the aggressive ones—are also the most intrinsically sensitive to 💊anti-cancer drugs when the stimuli are removed.
This means reducing inflammation could unmask therapeutic vulnerabilities in aggressive clones. 6/
This means reducing inflammation could unmask therapeutic vulnerabilities in aggressive clones. 6/
Bacterial (S. aureus) infections are a major clinical problem in CTCL, fueling malignant growth and persistence. S. aureus toxins selectively activate certain subclones, while leaving others largely unaffected. This provides a selective advantage to responsive subclones!
But it comes at a price… 5/
But it comes at a price… 5/

June 19, 2025 at 11:31 AM
Bacterial (S. aureus) infections are a major clinical problem in CTCL, fueling malignant growth and persistence. S. aureus toxins selectively activate certain subclones, while leaving others largely unaffected. This provides a selective advantage to responsive subclones!
But it comes at a price… 5/
But it comes at a price… 5/
These subclones show differences in tissue homing (some prefer blood, others skin), metabolism, and immune signaling. Intriguingly, the subclone most abundant in blood often has less capacity for interacting with their inflammatory environment, correlating with reduced proliferation in the skin. 4/

June 19, 2025 at 11:31 AM
These subclones show differences in tissue homing (some prefer blood, others skin), metabolism, and immune signaling. Intriguingly, the subclone most abundant in blood often has less capacity for interacting with their inflammatory environment, correlating with reduced proliferation in the skin. 4/
Using advanced single-cell analysis (scTCR+CITE-seq) on matched skin and blood, we found 🧬genetically distinct malignant subclones in more than 80% of L-CTCL patients. Subclones have distinct RNA+protein signatures, are shared between blood and skin, and co-exist over extended periods of time⏳. 3/

June 19, 2025 at 11:31 AM
Using advanced single-cell analysis (scTCR+CITE-seq) on matched skin and blood, we found 🧬genetically distinct malignant subclones in more than 80% of L-CTCL patients. Subclones have distinct RNA+protein signatures, are shared between blood and skin, and co-exist over extended periods of time⏳. 3/
TL;DR
👉Leukemic CTCL patients harbor functionally distinct co-existing subclones
👉Subclones respond differently to external factors such as cytokines, bacterial infections, and cancer drugs
👉The most aggressive subclones are also most sensitive to treatment if their extrinsic stimuli are removed
2/
👉Leukemic CTCL patients harbor functionally distinct co-existing subclones
👉Subclones respond differently to external factors such as cytokines, bacterial infections, and cancer drugs
👉The most aggressive subclones are also most sensitive to treatment if their extrinsic stimuli are removed
2/

June 19, 2025 at 11:31 AM
TL;DR
👉Leukemic CTCL patients harbor functionally distinct co-existing subclones
👉Subclones respond differently to external factors such as cytokines, bacterial infections, and cancer drugs
👉The most aggressive subclones are also most sensitive to treatment if their extrinsic stimuli are removed
2/
👉Leukemic CTCL patients harbor functionally distinct co-existing subclones
👉Subclones respond differently to external factors such as cytokines, bacterial infections, and cancer drugs
👉The most aggressive subclones are also most sensitive to treatment if their extrinsic stimuli are removed
2/
❗How can a cancer exploit its environment and still resist treatment?
✅The answer: co-existing malignant subclones.
Let me walk you through our latest study investigating how divergent evolution drives adaptability, aggressiveness, and drug resistance of T cell cancer. 1/🧵
doi.org/10.1158/2159...
✅The answer: co-existing malignant subclones.
Let me walk you through our latest study investigating how divergent evolution drives adaptability, aggressiveness, and drug resistance of T cell cancer. 1/🧵
doi.org/10.1158/2159...
June 19, 2025 at 11:31 AM
❗How can a cancer exploit its environment and still resist treatment?
✅The answer: co-existing malignant subclones.
Let me walk you through our latest study investigating how divergent evolution drives adaptability, aggressiveness, and drug resistance of T cell cancer. 1/🧵
doi.org/10.1158/2159...
✅The answer: co-existing malignant subclones.
Let me walk you through our latest study investigating how divergent evolution drives adaptability, aggressiveness, and drug resistance of T cell cancer. 1/🧵
doi.org/10.1158/2159...
Divergent evolution results in co-existing subclones that have different tissue preferences and respond differently to external factors such as cytokines and infections. The most aggressive subclones are also most sensitive to treatment if stimuli are removed exposing their vulnerabilities. 7/
June 19, 2025 at 11:17 AM
Divergent evolution results in co-existing subclones that have different tissue preferences and respond differently to external factors such as cytokines and infections. The most aggressive subclones are also most sensitive to treatment if stimuli are removed exposing their vulnerabilities. 7/
Here's the trade-off ⚖️: The subclones that respond most strongly to 🦠S. aureus toxins—the aggressive ones—are also the most intrinsically sensitive to 💊anti-cancer drugs when the stimuli are removed.
This means reducing inflammation could unmask therapeutic vulnerabilities in aggressive clones. 6/
This means reducing inflammation could unmask therapeutic vulnerabilities in aggressive clones. 6/
June 19, 2025 at 11:17 AM
Here's the trade-off ⚖️: The subclones that respond most strongly to 🦠S. aureus toxins—the aggressive ones—are also the most intrinsically sensitive to 💊anti-cancer drugs when the stimuli are removed.
This means reducing inflammation could unmask therapeutic vulnerabilities in aggressive clones. 6/
This means reducing inflammation could unmask therapeutic vulnerabilities in aggressive clones. 6/
Bacterial (S. aureus) infections are a major clinical problem in CTCL, fueling malignant growth and persistence. S. aureus toxins selectively activate certain subclones, while leaving others largely unaffected. This provides a selective advantage to responsive subclones!
But it comes at a price… 5/
But it comes at a price… 5/
June 19, 2025 at 11:17 AM
Bacterial (S. aureus) infections are a major clinical problem in CTCL, fueling malignant growth and persistence. S. aureus toxins selectively activate certain subclones, while leaving others largely unaffected. This provides a selective advantage to responsive subclones!
But it comes at a price… 5/
But it comes at a price… 5/
These subclones show differences in tissue homing (some prefer blood, others skin), metabolism, and immune signaling. Intriguingly, the subclone most abundant in blood often has less capacity for interacting with their inflammatory environment, correlating with reduced proliferation in the skin. 4/
June 19, 2025 at 11:17 AM
These subclones show differences in tissue homing (some prefer blood, others skin), metabolism, and immune signaling. Intriguingly, the subclone most abundant in blood often has less capacity for interacting with their inflammatory environment, correlating with reduced proliferation in the skin. 4/
Using advanced single-cell analysis (scTCR+CITE-seq) on matched skin and blood, we found 🧬genetically distinct malignant subclones in more than 80% of L-CTCL patients. Subclones have distinct RNA+protein signatures, are shared between blood and skin, and co-exist over extended periods of time⏳. 3/
June 19, 2025 at 11:17 AM
Using advanced single-cell analysis (scTCR+CITE-seq) on matched skin and blood, we found 🧬genetically distinct malignant subclones in more than 80% of L-CTCL patients. Subclones have distinct RNA+protein signatures, are shared between blood and skin, and co-exist over extended periods of time⏳. 3/
TL;DR
👉Leukemic CTCL patients harbor functionally distinct co-existing subclones
👉Subclones respond differently to external factors such as cytokines, bacterial infections, and cancer drugs
👉The most aggressive subclones are also most sensitive to treatment if their extrinsic stimuli are removed
2/
👉Leukemic CTCL patients harbor functionally distinct co-existing subclones
👉Subclones respond differently to external factors such as cytokines, bacterial infections, and cancer drugs
👉The most aggressive subclones are also most sensitive to treatment if their extrinsic stimuli are removed
2/
June 19, 2025 at 11:17 AM
TL;DR
👉Leukemic CTCL patients harbor functionally distinct co-existing subclones
👉Subclones respond differently to external factors such as cytokines, bacterial infections, and cancer drugs
👉The most aggressive subclones are also most sensitive to treatment if their extrinsic stimuli are removed
2/
👉Leukemic CTCL patients harbor functionally distinct co-existing subclones
👉Subclones respond differently to external factors such as cytokines, bacterial infections, and cancer drugs
👉The most aggressive subclones are also most sensitive to treatment if their extrinsic stimuli are removed
2/
This indicates that S. aureus enterotoxins can induce treatment resistance through two distinct pathways:
1. Directly through TCR-induced NFkB on malignant cells.
and
2. Indirectly through cytokines induced by SE-activation of both malignant and non-malignant T cells.
1. Directly through TCR-induced NFkB on malignant cells.
and
2. Indirectly through cytokines induced by SE-activation of both malignant and non-malignant T cells.

November 19, 2024 at 5:44 PM
This indicates that S. aureus enterotoxins can induce treatment resistance through two distinct pathways:
1. Directly through TCR-induced NFkB on malignant cells.
and
2. Indirectly through cytokines induced by SE-activation of both malignant and non-malignant T cells.
1. Directly through TCR-induced NFkB on malignant cells.
and
2. Indirectly through cytokines induced by SE-activation of both malignant and non-malignant T cells.
To determine if SE-induced treatment resistance was dependent on cytokine signaling, we used a clinical JAK-inhibitor (Tofacitinib).
Highlighting the heterogeneity of SS, we found that only half the patients were dependent on JAK signaling for their resistance and half were not.
Highlighting the heterogeneity of SS, we found that only half the patients were dependent on JAK signaling for their resistance and half were not.

November 19, 2024 at 5:44 PM
To determine if SE-induced treatment resistance was dependent on cytokine signaling, we used a clinical JAK-inhibitor (Tofacitinib).
Highlighting the heterogeneity of SS, we found that only half the patients were dependent on JAK signaling for their resistance and half were not.
Highlighting the heterogeneity of SS, we found that only half the patients were dependent on JAK signaling for their resistance and half were not.
Consistent with cytokine (JAK-STAT) signaling playing a role, we found that presence of SE induced a range of cytokines produced by both malignant and non-malignant T cells.
We show that a pool of these cytokines was also sufficient to induce drug resistance in malignant cells.
We show that a pool of these cytokines was also sufficient to induce drug resistance in malignant cells.

November 19, 2024 at 5:44 PM
Consistent with cytokine (JAK-STAT) signaling playing a role, we found that presence of SE induced a range of cytokines produced by both malignant and non-malignant T cells.
We show that a pool of these cytokines was also sufficient to induce drug resistance in malignant cells.
We show that a pool of these cytokines was also sufficient to induce drug resistance in malignant cells.
Indeed, blocking TCR signaling or downstream PKC-θ (upstream of NFkB activation) was sufficient to counteract the treatment resistance.
Moreover, only drugs that also inhibited NFkB signaling (Bortezomib & Crystal Violet) were unaffected by SE – implicating the TCR-PKC-NFkB axis.
Moreover, only drugs that also inhibited NFkB signaling (Bortezomib & Crystal Violet) were unaffected by SE – implicating the TCR-PKC-NFkB axis.

November 19, 2024 at 5:44 PM
Indeed, blocking TCR signaling or downstream PKC-θ (upstream of NFkB activation) was sufficient to counteract the treatment resistance.
Moreover, only drugs that also inhibited NFkB signaling (Bortezomib & Crystal Violet) were unaffected by SE – implicating the TCR-PKC-NFkB axis.
Moreover, only drugs that also inhibited NFkB signaling (Bortezomib & Crystal Violet) were unaffected by SE – implicating the TCR-PKC-NFkB axis.
Using CITE-seq we found that presence of SE largely overrides the transcriptional effect of Romidepsin in malignant T cells and identified TCR-signaling and downstream NFkB signaling as well as cytokine signaling as likely culprits (both make cells less sensitive to apoptosis).

November 19, 2024 at 5:44 PM
Using CITE-seq we found that presence of SE largely overrides the transcriptional effect of Romidepsin in malignant T cells and identified TCR-signaling and downstream NFkB signaling as well as cytokine signaling as likely culprits (both make cells less sensitive to apoptosis).
The induced resistance was not limited to Romidepsin but made the cancer cells resistant to other HDACi as well as DNA-targeting drugs, Doxorubicin and Etoposide.
The S. aureus enterotoxins (SE) did not hamper drug uptake, efflux pumps nor interfered directly with the drugs.
The S. aureus enterotoxins (SE) did not hamper drug uptake, efflux pumps nor interfered directly with the drugs.

November 19, 2024 at 5:44 PM
The induced resistance was not limited to Romidepsin but made the cancer cells resistant to other HDACi as well as DNA-targeting drugs, Doxorubicin and Etoposide.
The S. aureus enterotoxins (SE) did not hamper drug uptake, efflux pumps nor interfered directly with the drugs.
The S. aureus enterotoxins (SE) did not hamper drug uptake, efflux pumps nor interfered directly with the drugs.
We pinpointed the effect to a group of toxins called enterotoxins (SE) that have the ability to activate T cells through the T cell receptor (superantigens).
Recombinant SE was sufficient to induce HDACi resistance in cells but a mutated SE without superantigenic effect was not.
Recombinant SE was sufficient to induce HDACi resistance in cells but a mutated SE without superantigenic effect was not.


November 19, 2024 at 5:44 PM
We pinpointed the effect to a group of toxins called enterotoxins (SE) that have the ability to activate T cells through the T cell receptor (superantigens).
Recombinant SE was sufficient to induce HDACi resistance in cells but a mutated SE without superantigenic effect was not.
Recombinant SE was sufficient to induce HDACi resistance in cells but a mutated SE without superantigenic effect was not.
S. aureus produce toxins that modulate the tumor microenvironment. We found toxins produced by S. aureus (SA) isolated from SS patients made malignant cells resistant to treatment.
Importantly, treating the bacteria with SA-specific endolysin abrogated induction of resistance.
Importantly, treating the bacteria with SA-specific endolysin abrogated induction of resistance.

November 19, 2024 at 5:44 PM
S. aureus produce toxins that modulate the tumor microenvironment. We found toxins produced by S. aureus (SA) isolated from SS patients made malignant cells resistant to treatment.
Importantly, treating the bacteria with SA-specific endolysin abrogated induction of resistance.
Importantly, treating the bacteria with SA-specific endolysin abrogated induction of resistance.
Staphylococcus aureus (#MRSA) infections are frequent and major problem in Cutaneous T-cell Lymphoma (#CTCL). Eliminating SA not only clears the infections but also improves the clinical symptoms and treatment response of the cancer.
In this study, we ventured to figure out how.
In this study, we ventured to figure out how.

November 19, 2024 at 5:44 PM
Staphylococcus aureus (#MRSA) infections are frequent and major problem in Cutaneous T-cell Lymphoma (#CTCL). Eliminating SA not only clears the infections but also improves the clinical symptoms and treatment response of the cancer.
In this study, we ventured to figure out how.
In this study, we ventured to figure out how.