




Kyle Walding
@tbrnaughttb.bsky.social
TB doc, Manhattan TB consultant @ NYC Dept of Health
NYU Clinical Asst Professor of ID @ Bellevue Hospital
Loyola Med/Peds & Stanford ID
❤️: TB, ID, med ed, public health, health equity, immigrant safety/rights
Views = mine = great, & ≠ my employers' | 🏳️🌈
NYU Clinical Asst Professor of ID @ Bellevue Hospital
Loyola Med/Peds & Stanford ID
❤️: TB, ID, med ed, public health, health equity, immigrant safety/rights
Views = mine = great, & ≠ my employers' | 🏳️🌈
in my opinion, *particularly* at a safety net hospital in this current political climate, there is absolutely *no medical necessity* to document citizenship status in a patient’s medical record
if this becomes commonplace, its absence could be taken by some to mean “undocumented”
if this becomes commonplace, its absence could be taken by some to mean “undocumented”

April 18, 2025 at 2:26 PM
in my opinion, *particularly* at a safety net hospital in this current political climate, there is absolutely *no medical necessity* to document citizenship status in a patient’s medical record
if this becomes commonplace, its absence could be taken by some to mean “undocumented”
if this becomes commonplace, its absence could be taken by some to mean “undocumented”
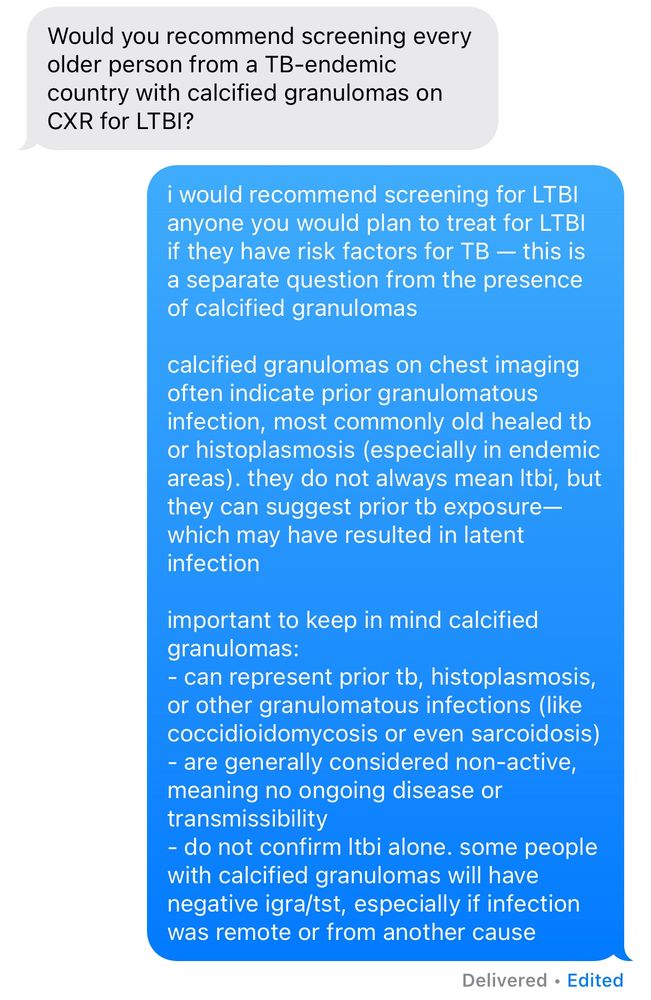
important learning re calcified granulomas vs LTBI (i get asked this Q a lot) — this is nuanced, but here are some important considerations #TBSky
April 16, 2025 at 1:05 PM
important learning re calcified granulomas vs LTBI (i get asked this Q a lot) — this is nuanced, but here are some important considerations #TBSky
>100,000 of us took to the streets of Manhattan (and >400,000 ppl nationwide!) today to stand against dangerous attacks on the federal workforce, immigrants, healthcare, and social safety nets for vulnerable populations #handsoff


April 5, 2025 at 8:44 PM
>100,000 of us took to the streets of Manhattan (and >400,000 ppl nationwide!) today to stand against dangerous attacks on the federal workforce, immigrants, healthcare, and social safety nets for vulnerable populations #handsoff
#IDSky: if you order a CBC diff, please remember to look at the diff, even in pts you don’t expect to find certain abnormalities (like in this asymptomatic US-born patient)
this level of eosinophilia is dangerously high! this patient needs an urgent eval for infectious and hematologic etiologies
this level of eosinophilia is dangerously high! this patient needs an urgent eval for infectious and hematologic etiologies

March 28, 2025 at 2:06 PM
#IDSky: if you order a CBC diff, please remember to look at the diff, even in pts you don’t expect to find certain abnormalities (like in this asymptomatic US-born patient)
this level of eosinophilia is dangerously high! this patient needs an urgent eval for infectious and hematologic etiologies
this level of eosinophilia is dangerously high! this patient needs an urgent eval for infectious and hematologic etiologies
the NYC DOH Bureau of TB Control just released our data for 2024 — another staggering increase in TB cases in NYC
NYC’s current prevalence is 9.5/100k
US national prevalence is ~3/100k
at a time when global and national TB control resources are extremely vulnerable #TBsky
NYC’s current prevalence is 9.5/100k
US national prevalence is ~3/100k
at a time when global and national TB control resources are extremely vulnerable #TBsky

March 27, 2025 at 4:21 PM
the NYC DOH Bureau of TB Control just released our data for 2024 — another staggering increase in TB cases in NYC
NYC’s current prevalence is 9.5/100k
US national prevalence is ~3/100k
at a time when global and national TB control resources are extremely vulnerable #TBsky
NYC’s current prevalence is 9.5/100k
US national prevalence is ~3/100k
at a time when global and national TB control resources are extremely vulnerable #TBsky
public health & city hospital doctors march for medicaid!
medicaid provides health insurance to over 80 million americans (nearly 1 in 4 people / almost 25% of the population!), including low-income families, pregnant people, children, elderly individuals, & people with disabilities
medicaid provides health insurance to over 80 million americans (nearly 1 in 4 people / almost 25% of the population!), including low-income families, pregnant people, children, elderly individuals, & people with disabilities




March 15, 2025 at 8:57 PM
public health & city hospital doctors march for medicaid!
medicaid provides health insurance to over 80 million americans (nearly 1 in 4 people / almost 25% of the population!), including low-income families, pregnant people, children, elderly individuals, & people with disabilities
medicaid provides health insurance to over 80 million americans (nearly 1 in 4 people / almost 25% of the population!), including low-income families, pregnant people, children, elderly individuals, & people with disabilities


us02web.zoom.us/webinar/regi...
please consider joining tomorrow if relevant to your patient population (it likely is!)
please consider joining tomorrow if relevant to your patient population (it likely is!)

February 11, 2025 at 5:29 PM
us02web.zoom.us/webinar/regi...
please consider joining tomorrow if relevant to your patient population (it likely is!)
please consider joining tomorrow if relevant to your patient population (it likely is!)
if anyone else is feeling overwhelmed/worried about the pace of attempted changes from this current administration, i found this argument convincing & helpful—only 15 mins (on spotify & apple)

February 3, 2025 at 10:35 PM
if anyone else is feeling overwhelmed/worried about the pace of attempted changes from this current administration, i found this argument convincing & helpful—only 15 mins (on spotify & apple)
hand vs. meat grinder c/b finger osteo
s/p disarticulation of distal phalanx with concern for ongoing osteo more proximally
culture results and AST in image: what’s your regimen for the MSSA + A baumanii? would you use TMP/SMX monotherapy? TMP/SMX + cipro? doxy + cipro?
DM, no CKD #IDSky
s/p disarticulation of distal phalanx with concern for ongoing osteo more proximally
culture results and AST in image: what’s your regimen for the MSSA + A baumanii? would you use TMP/SMX monotherapy? TMP/SMX + cipro? doxy + cipro?
DM, no CKD #IDSky

January 23, 2025 at 11:38 PM
hand vs. meat grinder c/b finger osteo
s/p disarticulation of distal phalanx with concern for ongoing osteo more proximally
culture results and AST in image: what’s your regimen for the MSSA + A baumanii? would you use TMP/SMX monotherapy? TMP/SMX + cipro? doxy + cipro?
DM, no CKD #IDSky
s/p disarticulation of distal phalanx with concern for ongoing osteo more proximally
culture results and AST in image: what’s your regimen for the MSSA + A baumanii? would you use TMP/SMX monotherapy? TMP/SMX + cipro? doxy + cipro?
DM, no CKD #IDSky
this table feels truer to me based on available data/reason lol — the stakes are high and the CI needs are not insane, so when resources are available, i would try to investigate!

January 15, 2025 at 9:50 PM
this table feels truer to me based on available data/reason lol — the stakes are high and the CI needs are not insane, so when resources are available, i would try to investigate!




sharing some nyc winter vibes for all ❄️




December 21, 2024 at 8:42 PM
sharing some nyc winter vibes for all ❄️
an inadequate mitogen is trickier! a ddx:
Patient:
1. lymphopenia (esp ↓ T cells)
2. inability for lymphocytes to proliferate
3. inherited/acquired inability to produce IFN-γ
4. interfering substance (eg, heterophile Ab)
Lab:
5. lab-related technical issues (see image)
6/10
Patient:
1. lymphopenia (esp ↓ T cells)
2. inability for lymphocytes to proliferate
3. inherited/acquired inability to produce IFN-γ
4. interfering substance (eg, heterophile Ab)
Lab:
5. lab-related technical issues (see image)
6/10

December 7, 2024 at 4:56 PM
an inadequate mitogen is trickier! a ddx:
Patient:
1. lymphopenia (esp ↓ T cells)
2. inability for lymphocytes to proliferate
3. inherited/acquired inability to produce IFN-γ
4. interfering substance (eg, heterophile Ab)
Lab:
5. lab-related technical issues (see image)
6/10
Patient:
1. lymphopenia (esp ↓ T cells)
2. inability for lymphocytes to proliferate
3. inherited/acquired inability to produce IFN-γ
4. interfering substance (eg, heterophile Ab)
Lab:
5. lab-related technical issues (see image)
6/10
a nil that is "too high" has 2 major causes:
(1) lab technical issues (reagent storage, blood collection, handling), or
(2) the patient has "too much" IFN-γ in the background (eg, from another inflammatory condition; this is less common)
5/10
(1) lab technical issues (reagent storage, blood collection, handling), or
(2) the patient has "too much" IFN-γ in the background (eg, from another inflammatory condition; this is less common)
5/10

December 7, 2024 at 4:56 PM
a nil that is "too high" has 2 major causes:
(1) lab technical issues (reagent storage, blood collection, handling), or
(2) the patient has "too much" IFN-γ in the background (eg, from another inflammatory condition; this is less common)
5/10
(1) lab technical issues (reagent storage, blood collection, handling), or
(2) the patient has "too much" IFN-γ in the background (eg, from another inflammatory condition; this is less common)
5/10
notice the nil is ➖d from all values—that's bc it's the pt's *background* IFN-γ unrelated to TB ags.
now, let's look at TB1 & TB2—these are TB-specific ag groups which stimulate CD4 & CD8 responses (resp).
if *both* TB1/TB2 → ↑ IFN-γ prdxn (>0.35 IU/mL), the test is ➕
9/10
now, let's look at TB1 & TB2—these are TB-specific ag groups which stimulate CD4 & CD8 responses (resp).
if *both* TB1/TB2 → ↑ IFN-γ prdxn (>0.35 IU/mL), the test is ➕
9/10

December 7, 2024 at 4:47 PM
notice the nil is ➖d from all values—that's bc it's the pt's *background* IFN-γ unrelated to TB ags.
now, let's look at TB1 & TB2—these are TB-specific ag groups which stimulate CD4 & CD8 responses (resp).
if *both* TB1/TB2 → ↑ IFN-γ prdxn (>0.35 IU/mL), the test is ➕
9/10
now, let's look at TB1 & TB2—these are TB-specific ag groups which stimulate CD4 & CD8 responses (resp).
if *both* TB1/TB2 → ↑ IFN-γ prdxn (>0.35 IU/mL), the test is ➕
9/10
we have effective T cell proliferation & IFN-γ-releasing ability!
now let's look @ the nil, or the background level of IFN-γ in the pt's serum (➖ control): it should be <8 IU/mL (is often <1); ↓er = better!
↓ nil = this pt doesn't have too much IFN-γ in the background
8/10
now let's look @ the nil, or the background level of IFN-γ in the pt's serum (➖ control): it should be <8 IU/mL (is often <1); ↓er = better!
↓ nil = this pt doesn't have too much IFN-γ in the background
8/10

December 7, 2024 at 4:47 PM
we have effective T cell proliferation & IFN-γ-releasing ability!
now let's look @ the nil, or the background level of IFN-γ in the pt's serum (➖ control): it should be <8 IU/mL (is often <1); ↓er = better!
↓ nil = this pt doesn't have too much IFN-γ in the background
8/10
now let's look @ the nil, or the background level of IFN-γ in the pt's serum (➖ control): it should be <8 IU/mL (is often <1); ↓er = better!
↓ nil = this pt doesn't have too much IFN-γ in the background
8/10
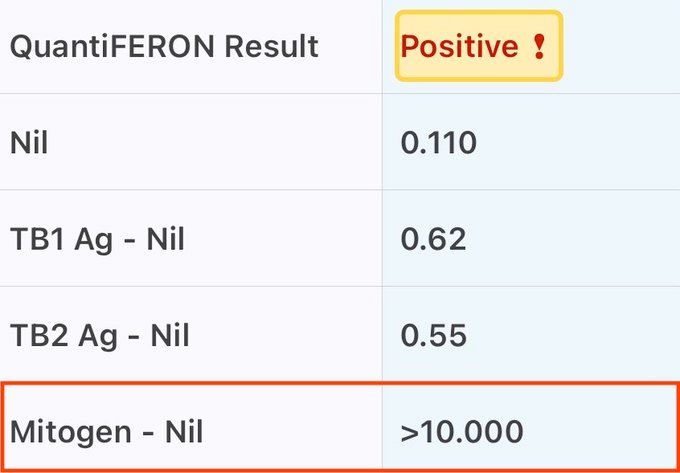
QFT interpretation:
4 values: mitogen, nil, TB1, & TB2 (pic)
@ bottom, mitogen is a nonspecific (not TB) stimulator of T cell proliferation (➕ control): it should be >2 IU/mL, but ↑er = better!
↑ mito = this pt's T cells can proliferate & release IFN-γ *in general*
7/10
4 values: mitogen, nil, TB1, & TB2 (pic)
@ bottom, mitogen is a nonspecific (not TB) stimulator of T cell proliferation (➕ control): it should be >2 IU/mL, but ↑er = better!
↑ mito = this pt's T cells can proliferate & release IFN-γ *in general*
7/10
December 7, 2024 at 4:47 PM
QFT interpretation:
4 values: mitogen, nil, TB1, & TB2 (pic)
@ bottom, mitogen is a nonspecific (not TB) stimulator of T cell proliferation (➕ control): it should be >2 IU/mL, but ↑er = better!
↑ mito = this pt's T cells can proliferate & release IFN-γ *in general*
7/10
4 values: mitogen, nil, TB1, & TB2 (pic)
@ bottom, mitogen is a nonspecific (not TB) stimulator of T cell proliferation (➕ control): it should be >2 IU/mL, but ↑er = better!
↑ mito = this pt's T cells can proliferate & release IFN-γ *in general*
7/10
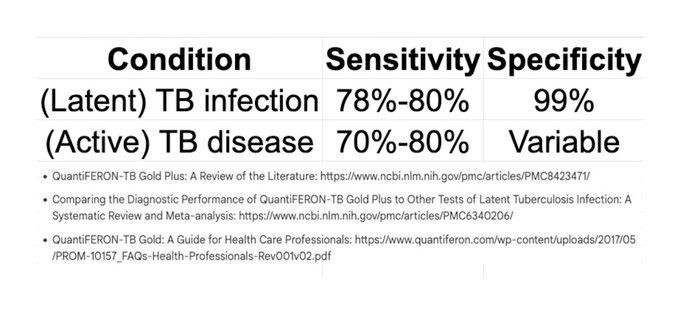
- a ➖ test does not r/o prior exposure OR current infxn/dz
- a ➕ test cannot distinguish bw (latent) TB infxn & (active) TB dz
all test results = probability titrations!
sensitivity & specificity vary widely by tested population (eg, US vs India); here are some ranges:
- a ➕ test cannot distinguish bw (latent) TB infxn & (active) TB dz
all test results = probability titrations!
sensitivity & specificity vary widely by tested population (eg, US vs India); here are some ranges:
December 7, 2024 at 4:47 PM
- a ➖ test does not r/o prior exposure OR current infxn/dz
- a ➕ test cannot distinguish bw (latent) TB infxn & (active) TB dz
all test results = probability titrations!
sensitivity & specificity vary widely by tested population (eg, US vs India); here are some ranges:
- a ➕ test cannot distinguish bw (latent) TB infxn & (active) TB dz
all test results = probability titrations!
sensitivity & specificity vary widely by tested population (eg, US vs India); here are some ranges:
#TBSky #IDSky
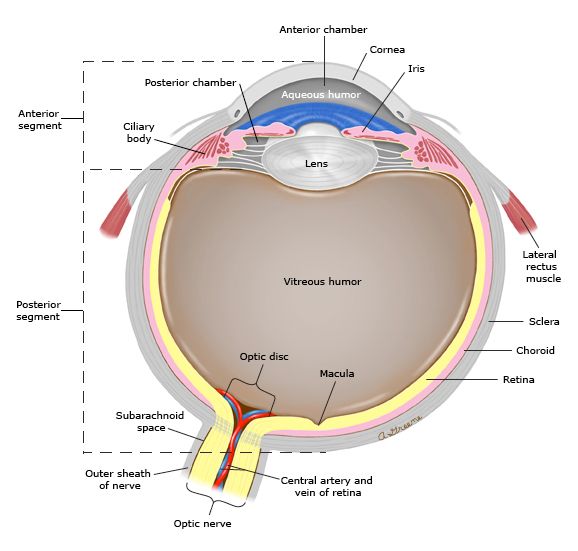
TB can affect any organ (except hair & nails), including the 👁️
any part of the 👁️ can be affected, eg:
- choroiditis/chorioretinitis/choroidal granuloma,
- optic neuritis/disc granuloma,
- subretinal abscess,
- orbital cellulitis,
- [necrotizing] scleritis
- keratitis, & others!
TB can affect any organ (except hair & nails), including the 👁️
any part of the 👁️ can be affected, eg:
- choroiditis/chorioretinitis/choroidal granuloma,
- optic neuritis/disc granuloma,
- subretinal abscess,
- orbital cellulitis,
- [necrotizing] scleritis
- keratitis, & others!
December 7, 2024 at 4:39 PM
#TBSky #IDSky
detecting resistance (R) in MTB:
- GeneXpert MTB/RIF: RIF R
- Pyrosequencing (PSQ): short reads of DNA; INH, RIF, & FQN R (not PZA)
- Sanger sequencing: long reads of DNA; many 1st/2nd-line drugs (incl. PZA)
- Whole genome sequencing (WGS): genus, species, most 1st/2nd-line drugs
detecting resistance (R) in MTB:
- GeneXpert MTB/RIF: RIF R
- Pyrosequencing (PSQ): short reads of DNA; INH, RIF, & FQN R (not PZA)
- Sanger sequencing: long reads of DNA; many 1st/2nd-line drugs (incl. PZA)
- Whole genome sequencing (WGS): genus, species, most 1st/2nd-line drugs

December 7, 2024 at 4:34 PM
#TBSky #IDSky
why is cavitary pulmonary TB dz thought to have a higher risk of transmission than noncavitary dz?
- tendency toward ↑ bacillary (bacterial) load in cavity
- tendency toward sputum smear positivity
- higher risk of relapse & treatment failure
www.sciencedirect.com/science/arti...
why is cavitary pulmonary TB dz thought to have a higher risk of transmission than noncavitary dz?
- tendency toward ↑ bacillary (bacterial) load in cavity
- tendency toward sputum smear positivity
- higher risk of relapse & treatment failure
www.sciencedirect.com/science/arti...

December 7, 2024 at 4:31 PM
#TBSky #IDSky
why is cavitary pulmonary TB dz thought to have a higher risk of transmission than noncavitary dz?
- tendency toward ↑ bacillary (bacterial) load in cavity
- tendency toward sputum smear positivity
- higher risk of relapse & treatment failure
www.sciencedirect.com/science/arti...
why is cavitary pulmonary TB dz thought to have a higher risk of transmission than noncavitary dz?
- tendency toward ↑ bacillary (bacterial) load in cavity
- tendency toward sputum smear positivity
- higher risk of relapse & treatment failure
www.sciencedirect.com/science/arti...
be sure to follow @wearetb.bsky.social here and on instagram, too! @atrophywife.bsky.social gave a talk at a TB course i attended at GTBI and she’s phenomenal :) great support network!

November 26, 2024 at 10:59 PM
be sure to follow @wearetb.bsky.social here and on instagram, too! @atrophywife.bsky.social gave a talk at a TB course i attended at GTBI and she’s phenomenal :) great support network!