



@sivatrainees.bsky.social
What would you like?
I'll see what we can cobble together!
I'll see what we can cobble together!
August 9, 2025 at 2:05 PM
What would you like?
I'll see what we can cobble together!
I'll see what we can cobble together!
0.2mg/kg bolus has no EEG effect
(See image)
0.3mg/kg may have an effect but I feel clinically un likely
0.5mg/kg often will induce EEG changes that are associated with an rise in BIS index
If bolusing and concerned about rise in BIS value, give during a period of surgical stability
(See image)
0.3mg/kg may have an effect but I feel clinically un likely
0.5mg/kg often will induce EEG changes that are associated with an rise in BIS index
If bolusing and concerned about rise in BIS value, give during a period of surgical stability
July 8, 2025 at 3:28 AM
0.2mg/kg bolus has no EEG effect
(See image)
0.3mg/kg may have an effect but I feel clinically un likely
0.5mg/kg often will induce EEG changes that are associated with an rise in BIS index
If bolusing and concerned about rise in BIS value, give during a period of surgical stability
(See image)
0.3mg/kg may have an effect but I feel clinically un likely
0.5mg/kg often will induce EEG changes that are associated with an rise in BIS index
If bolusing and concerned about rise in BIS value, give during a period of surgical stability
Likewise have a similar recipe. I am enjoying comparing my bolus infusion technique to intermittent boluses
July 6, 2025 at 7:36 AM
Likewise have a similar recipe. I am enjoying comparing my bolus infusion technique to intermittent boluses
After modelling do you have any thoughts on how useful TCI ketamine is Vs bolus infusion? Ie any circumstances you might choose TCI first?
July 6, 2025 at 6:40 AM
After modelling do you have any thoughts on how useful TCI ketamine is Vs bolus infusion? Ie any circumstances you might choose TCI first?
Brilliant, thank you.
Caveats noted!
Caveats noted!
June 23, 2025 at 1:23 PM
Brilliant, thank you.
Caveats noted!
Caveats noted!
7x more failures!?
Do you have a study I can look at?
Do you have a study I can look at?
June 23, 2025 at 1:13 PM
7x more failures!?
Do you have a study I can look at?
Do you have a study I can look at?
If performed by a second
person, the cost isn't their salary. It's the time that could be spent elsewhere. Helping with turnover, prepping for the next case etc
If performed by airway assistant - disagree with this practice - The cost is attention divided between multiple important tasks.
person, the cost isn't their salary. It's the time that could be spent elsewhere. Helping with turnover, prepping for the next case etc
If performed by airway assistant - disagree with this practice - The cost is attention divided between multiple important tasks.
June 8, 2025 at 5:01 AM
If performed by a second
person, the cost isn't their salary. It's the time that could be spent elsewhere. Helping with turnover, prepping for the next case etc
If performed by airway assistant - disagree with this practice - The cost is attention divided between multiple important tasks.
person, the cost isn't their salary. It's the time that could be spent elsewhere. Helping with turnover, prepping for the next case etc
If performed by airway assistant - disagree with this practice - The cost is attention divided between multiple important tasks.
If performed by a second
person, the cost isn't their salary. It's the time that could be spent elsewhere. Helping with turnover, prepping for the next case etc
If performed by airway assistant - disagree with this practice - The cost is attention divided between multiple important tasks.
person, the cost isn't their salary. It's the time that could be spent elsewhere. Helping with turnover, prepping for the next case etc
If performed by airway assistant - disagree with this practice - The cost is attention divided between multiple important tasks.
June 8, 2025 at 4:59 AM
If performed by a second
person, the cost isn't their salary. It's the time that could be spent elsewhere. Helping with turnover, prepping for the next case etc
If performed by airway assistant - disagree with this practice - The cost is attention divided between multiple important tasks.
person, the cost isn't their salary. It's the time that could be spent elsewhere. Helping with turnover, prepping for the next case etc
If performed by airway assistant - disagree with this practice - The cost is attention divided between multiple important tasks.
Completely agree with this point about us not necessarily being great at predicting who has a full stomach, especially in the era of comorbid disease and GLP1s
June 8, 2025 at 4:59 AM
Completely agree with this point about us not necessarily being great at predicting who has a full stomach, especially in the era of comorbid disease and GLP1s
Aspiration has an incidence of between 1:900 - 1:10,000 (NAP4)
Perioperative cardiac arrest has an incidence of 1:3000 (NAP7) - Arguably equally catastrophic so should every patient have defib pads put on at the start of a case?
Perioperative cardiac arrest has an incidence of 1:3000 (NAP7) - Arguably equally catastrophic so should every patient have defib pads put on at the start of a case?
June 8, 2025 at 4:55 AM
Aspiration has an incidence of between 1:900 - 1:10,000 (NAP4)
Perioperative cardiac arrest has an incidence of 1:3000 (NAP7) - Arguably equally catastrophic so should every patient have defib pads put on at the start of a case?
Perioperative cardiac arrest has an incidence of 1:3000 (NAP7) - Arguably equally catastrophic so should every patient have defib pads put on at the start of a case?
But I think your question is less about having cricoid as an absolute but maybe where are we drawing a line as to who to use it on?
a man in a robe is standing in a dark room with the words `` only sith deal in absolutes '' written on the screen .
ALT: a man in a robe is standing in a dark room with the words `` only sith deal in absolutes '' written on the screen .
media.tenor.com
June 8, 2025 at 2:06 AM
But I think your question is less about having cricoid as an absolute but maybe where are we drawing a line as to who to use it on?
Every intervention in healthcare has an opportunity cost.
Cricoid force should be performed by a team member with no other role.
Cricoid time x No of anaesthetics/ per hosp/ per year = large number
Aspiration low incidence in general anaesthetic pop. Cricoid becomes non cost effective.
Cricoid force should be performed by a team member with no other role.
Cricoid time x No of anaesthetics/ per hosp/ per year = large number
Aspiration low incidence in general anaesthetic pop. Cricoid becomes non cost effective.
June 8, 2025 at 2:04 AM
Every intervention in healthcare has an opportunity cost.
Cricoid force should be performed by a team member with no other role.
Cricoid time x No of anaesthetics/ per hosp/ per year = large number
Aspiration low incidence in general anaesthetic pop. Cricoid becomes non cost effective.
Cricoid force should be performed by a team member with no other role.
Cricoid time x No of anaesthetics/ per hosp/ per year = large number
Aspiration low incidence in general anaesthetic pop. Cricoid becomes non cost effective.
That is a great study! One to be kept in the bank of interesting papers.
June 5, 2025 at 2:18 AM
That is a great study! One to be kept in the bank of interesting papers.
Reposted

I don’t think anyone considers thio part of RSI anymore but I’m certain most who’ve abandoned cricoid are still using sux/roc & many aren’t FMV. It’s definitely singled out.
Again, I qtn whether the rationale for RSI is sound.
This is my fav evidence FOR cricoid. journals.lww.com/anesthesia-a...
Again, I qtn whether the rationale for RSI is sound.
This is my fav evidence FOR cricoid. journals.lww.com/anesthesia-a...
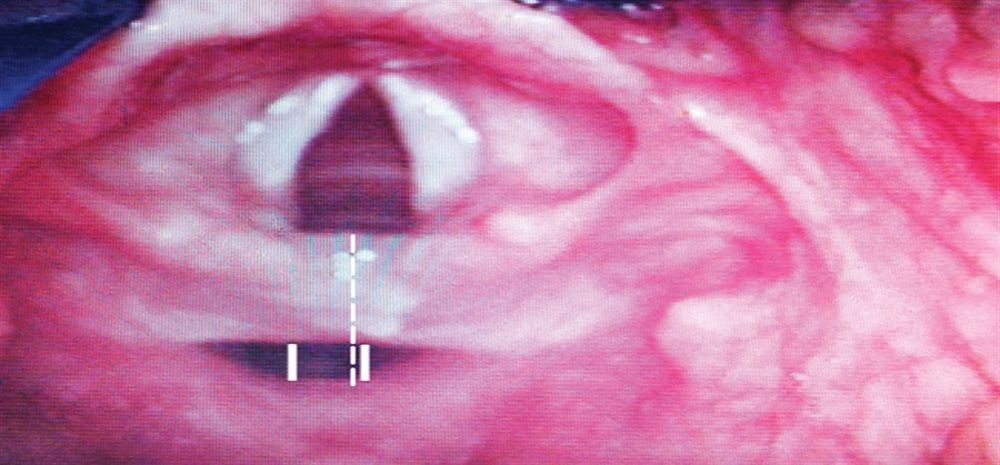
The Effectiveness of Cricoid Pressure for Occluding the... : Anesthesia & Analgesia
al entrance with and without CP in anesthetized and paralyzed adult patients.
METHODS:
One hundred seven, nonobese ASA physical status I and II patients were recruited for the study. A cricoid forc...
journals.lww.com
June 4, 2025 at 4:29 PM
I don’t think anyone considers thio part of RSI anymore but I’m certain most who’ve abandoned cricoid are still using sux/roc & many aren’t FMV. It’s definitely singled out.
Again, I qtn whether the rationale for RSI is sound.
This is my fav evidence FOR cricoid. journals.lww.com/anesthesia-a...
Again, I qtn whether the rationale for RSI is sound.
This is my fav evidence FOR cricoid. journals.lww.com/anesthesia-a...
No thats fair. And perhaps RSI is not the answer to making us take more care. But we're not always careful for a variety of human factor-ey reasons...
Fine you've convinced me! But can I replace it with another fun acronym instead?
Fine you've convinced me! But can I replace it with another fun acronym instead?
June 4, 2025 at 11:44 PM
No thats fair. And perhaps RSI is not the answer to making us take more care. But we're not always careful for a variety of human factor-ey reasons...
Fine you've convinced me! But can I replace it with another fun acronym instead?
Fine you've convinced me! But can I replace it with another fun acronym instead?
Interesting!
So can I gas induce them?
Arguably 8% sevo can be reasonably quick...
I joke of course but I think if you're being really careful in frail patients you can reach an accidental plane of 'excitability'
If I'm honest I don't disagree with your points
So can I gas induce them?
Arguably 8% sevo can be reasonably quick...
I joke of course but I think if you're being really careful in frail patients you can reach an accidental plane of 'excitability'
If I'm honest I don't disagree with your points
June 4, 2025 at 11:07 PM
Interesting!
So can I gas induce them?
Arguably 8% sevo can be reasonably quick...
I joke of course but I think if you're being really careful in frail patients you can reach an accidental plane of 'excitability'
If I'm honest I don't disagree with your points
So can I gas induce them?
Arguably 8% sevo can be reasonably quick...
I joke of course but I think if you're being really careful in frail patients you can reach an accidental plane of 'excitability'
If I'm honest I don't disagree with your points
Then again, here I am arguing about the term rather than the substance of what an RSI is. Perhaps we do need to be rid of the term...
June 4, 2025 at 11:02 PM
Then again, here I am arguing about the term rather than the substance of what an RSI is. Perhaps we do need to be rid of the term...
There were several cases of cardiac arrest in NAP7 related to TIVA use where anaesthetists didn't change their practice in sick patients.
The term RSI serves as a warning 'This patient is sick, Take care'
- Use roc not vec, have the suction under the pillow, think about asking for that NG prior
The term RSI serves as a warning 'This patient is sick, Take care'
- Use roc not vec, have the suction under the pillow, think about asking for that NG prior
June 4, 2025 at 10:59 PM
There were several cases of cardiac arrest in NAP7 related to TIVA use where anaesthetists didn't change their practice in sick patients.
The term RSI serves as a warning 'This patient is sick, Take care'
- Use roc not vec, have the suction under the pillow, think about asking for that NG prior
The term RSI serves as a warning 'This patient is sick, Take care'
- Use roc not vec, have the suction under the pillow, think about asking for that NG prior
By your other point do you mean
that our usual practice has changed ie we should preox and sit up every patient?
I'd argue that a lot of the PUMA recommendations we don't do for all Pts - or at the very least we aren't scrupulously careful.
In a patient who 'needs' an RSI We take time to prepare.
that our usual practice has changed ie we should preox and sit up every patient?
I'd argue that a lot of the PUMA recommendations we don't do for all Pts - or at the very least we aren't scrupulously careful.
In a patient who 'needs' an RSI We take time to prepare.
June 4, 2025 at 10:55 PM
By your other point do you mean
that our usual practice has changed ie we should preox and sit up every patient?
I'd argue that a lot of the PUMA recommendations we don't do for all Pts - or at the very least we aren't scrupulously careful.
In a patient who 'needs' an RSI We take time to prepare.
that our usual practice has changed ie we should preox and sit up every patient?
I'd argue that a lot of the PUMA recommendations we don't do for all Pts - or at the very least we aren't scrupulously careful.
In a patient who 'needs' an RSI We take time to prepare.
Good points!
I would agree, deeply paralysed and anaesthetised pt before instrumentation is key
But I think the 1st part - rapid - is important.
Risk of aspiration is not proportional to length of time without a protected airway, but does this mean I can take as long as I want with my induction?
I would agree, deeply paralysed and anaesthetised pt before instrumentation is key
But I think the 1st part - rapid - is important.
Risk of aspiration is not proportional to length of time without a protected airway, but does this mean I can take as long as I want with my induction?
June 4, 2025 at 10:53 PM
Good points!
I would agree, deeply paralysed and anaesthetised pt before instrumentation is key
But I think the 1st part - rapid - is important.
Risk of aspiration is not proportional to length of time without a protected airway, but does this mean I can take as long as I want with my induction?
I would agree, deeply paralysed and anaesthetised pt before instrumentation is key
But I think the 1st part - rapid - is important.
Risk of aspiration is not proportional to length of time without a protected airway, but does this mean I can take as long as I want with my induction?
The only way to be safe 🤣
June 4, 2025 at 2:23 PM
The only way to be safe 🤣