




Rajiv Thavanathan
@rajivthava.bsky.social
Emergency Medicine Physician / POCUS in Ottawa, Canada +/- music, comedy, guitars, sandwiches. VU's my own. he/him
Really thought I would have earned this more for the Coomer tweet hah
October 18, 2023 at 3:54 AM
Really thought I would have earned this more for the Coomer tweet hah
Take Home Points:
• POCUS not always perfect for reversible causes or RWMA (especially while on ino/pressors) but can help narrow DDx quickly.
• Anterior STD can be diagnostic of posterior-OMI, even if 12-/15- doesn't meet "STEMI criteria"
See:
hqmeded-ecg.blogspot.com/2022/01/7-st...
• POCUS not always perfect for reversible causes or RWMA (especially while on ino/pressors) but can help narrow DDx quickly.
• Anterior STD can be diagnostic of posterior-OMI, even if 12-/15- doesn't meet "STEMI criteria"
See:
hqmeded-ecg.blogspot.com/2022/01/7-st...
October 6, 2023 at 7:08 PM
Take Home Points:
• POCUS not always perfect for reversible causes or RWMA (especially while on ino/pressors) but can help narrow DDx quickly.
• Anterior STD can be diagnostic of posterior-OMI, even if 12-/15- doesn't meet "STEMI criteria"
See:
hqmeded-ecg.blogspot.com/2022/01/7-st...
• POCUS not always perfect for reversible causes or RWMA (especially while on ino/pressors) but can help narrow DDx quickly.
• Anterior STD can be diagnostic of posterior-OMI, even if 12-/15- doesn't meet "STEMI criteria"
See:
hqmeded-ecg.blogspot.com/2022/01/7-st...
[not strictly necessary for Dx but 15-lead did also meet STEMI criteria]
Cath showed culprit 100% Cx -> balloon/DES across marginal -> TIMI3.
TTE: EF35% with anterolateral/inferior RWMA.
Outcome: Extubated few days later, neuro-intact/oriented, favourable prognosis.
Cath showed culprit 100% Cx -> balloon/DES across marginal -> TIMI3.
TTE: EF35% with anterolateral/inferior RWMA.
Outcome: Extubated few days later, neuro-intact/oriented, favourable prognosis.
October 6, 2023 at 7:07 PM
[not strictly necessary for Dx but 15-lead did also meet STEMI criteria]
Cath showed culprit 100% Cx -> balloon/DES across marginal -> TIMI3.
TTE: EF35% with anterolateral/inferior RWMA.
Outcome: Extubated few days later, neuro-intact/oriented, favourable prognosis.
Cath showed culprit 100% Cx -> balloon/DES across marginal -> TIMI3.
TTE: EF35% with anterolateral/inferior RWMA.
Outcome: Extubated few days later, neuro-intact/oriented, favourable prognosis.
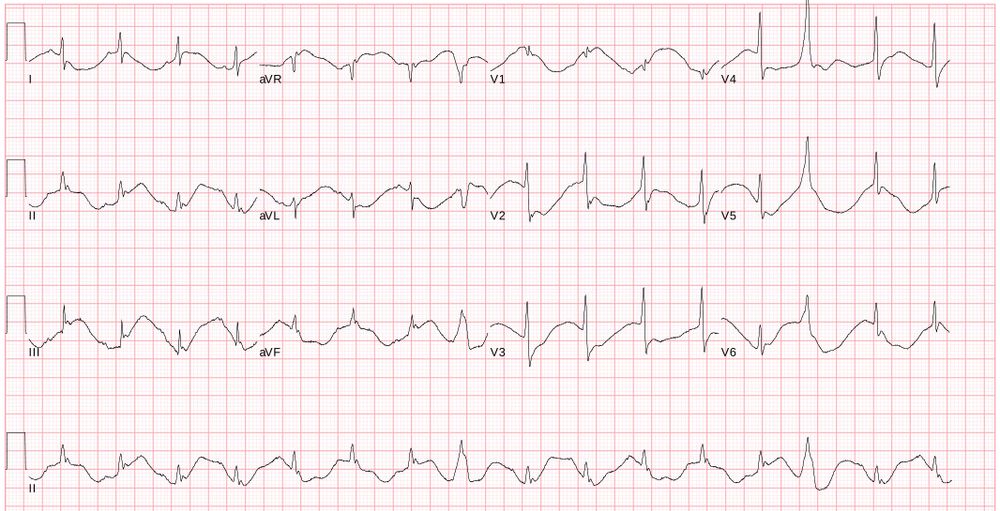
Initial ECG a bit tough, shows very long QTc, possible STE inferiorly. Repeat less inferior STE, but clear STD anterior max V2-4 with R-wave - is this diffuse subendo isch? This is crucial pattern to know- in fact diagnostic posterior OMI.

October 6, 2023 at 7:07 PM
Initial ECG a bit tough, shows very long QTc, possible STE inferiorly. Repeat less inferior STE, but clear STD anterior max V2-4 with R-wave - is this diffuse subendo isch? This is crucial pattern to know- in fact diagnostic posterior OMI.
What's the cause -
Dissection?
OMI/ACS?
PE?
Arrhythmogenic?
POCUS:
Difficult views- No PCE, reasonable LV Fxn (had epi/norepi), initially thought maybe ?inferolateral RWMA but couldn’t convince myself of it, ++pulmonary edema, IVC small/collapsing, Abdo aorta no AAA/flap, no DVT
Dissection?
OMI/ACS?
PE?
Arrhythmogenic?
POCUS:
Difficult views- No PCE, reasonable LV Fxn (had epi/norepi), initially thought maybe ?inferolateral RWMA but couldn’t convince myself of it, ++pulmonary edema, IVC small/collapsing, Abdo aorta no AAA/flap, no DVT

October 6, 2023 at 7:06 PM
What's the cause -
Dissection?
OMI/ACS?
PE?
Arrhythmogenic?
POCUS:
Difficult views- No PCE, reasonable LV Fxn (had epi/norepi), initially thought maybe ?inferolateral RWMA but couldn’t convince myself of it, ++pulmonary edema, IVC small/collapsing, Abdo aorta no AAA/flap, no DVT
Dissection?
OMI/ACS?
PE?
Arrhythmogenic?
POCUS:
Difficult views- No PCE, reasonable LV Fxn (had epi/norepi), initially thought maybe ?inferolateral RWMA but couldn’t convince myself of it, ++pulmonary edema, IVC small/collapsing, Abdo aorta no AAA/flap, no DVT
Can't have sepsis if you have zero suspicion for infection
October 6, 2023 at 2:45 PM
Can't have sepsis if you have zero suspicion for infection
Links should also always be the exact same font as the usual body text so they are completely indistinguishable. Just randomly click on words/phrases hoping it'll take you somewhere else
October 5, 2023 at 5:04 PM
Links should also always be the exact same font as the usual body text so they are completely indistinguishable. Just randomly click on words/phrases hoping it'll take you somewhere else
Hospitalist? You mean EM doc
October 5, 2023 at 4:40 PM
Hospitalist? You mean EM doc