




Rahul Banerjee, MD, FACP
@rahulbanerjeemd.bsky.social
Assistant Professor at Fred Hutch Cancer Center (Seattle, WA, USA) specializing in multiple myeloma #MMsm and CAR-T therapy.
My research focus: improving the patient experience in myeloma.
COI: https://coi.asco.org/share/VU2-FHC3/Rahul%20Banerjee
My research focus: improving the patient experience in myeloma.
COI: https://coi.asco.org/share/VU2-FHC3/Rahul%20Banerjee
My takeaways from RedirecTT-1 (tal/tec dual bsAbs in myeloma #MMsm) for @fredhutch journal watch.
[Images but technically no memes in my talk 😉]
Efficacy & safety profiles are both striking! I can't help but wonder what earlier IVIG and bsAb de-escalation might have done.
[Images but technically no memes in my talk 😉]
Efficacy & safety profiles are both striking! I can't help but wonder what earlier IVIG and bsAb de-escalation might have done.




January 17, 2025 at 3:30 AM
My takeaways from RedirecTT-1 (tal/tec dual bsAbs in myeloma #MMsm) for @fredhutch journal watch.
[Images but technically no memes in my talk 😉]
Efficacy & safety profiles are both striking! I can't help but wonder what earlier IVIG and bsAb de-escalation might have done.
[Images but technically no memes in my talk 😉]
Efficacy & safety profiles are both striking! I can't help but wonder what earlier IVIG and bsAb de-escalation might have done.
Also out in @BloodAdvances during #ASH24 by rising 🌟 @nadineabdal and @MayoMyeloma!
PROs strongly correlate with OS in #MMsm. In MVA, fatigue as prognostic for OS as FISH and ASCT 😳
Some confounders (anemia, frailty) but worth studying interventions!
ashpublications.org/bloodadvance...
PROs strongly correlate with OS in #MMsm. In MVA, fatigue as prognostic for OS as FISH and ASCT 😳
Some confounders (anemia, frailty) but worth studying interventions!
ashpublications.org/bloodadvance...


December 13, 2024 at 6:51 PM
Also out in @BloodAdvances during #ASH24 by rising 🌟 @nadineabdal and @MayoMyeloma!
PROs strongly correlate with OS in #MMsm. In MVA, fatigue as prognostic for OS as FISH and ASCT 😳
Some confounders (anemia, frailty) but worth studying interventions!
ashpublications.org/bloodadvance...
PROs strongly correlate with OS in #MMsm. In MVA, fatigue as prognostic for OS as FISH and ASCT 😳
Some confounders (anemia, frailty) but worth studying interventions!
ashpublications.org/bloodadvance...
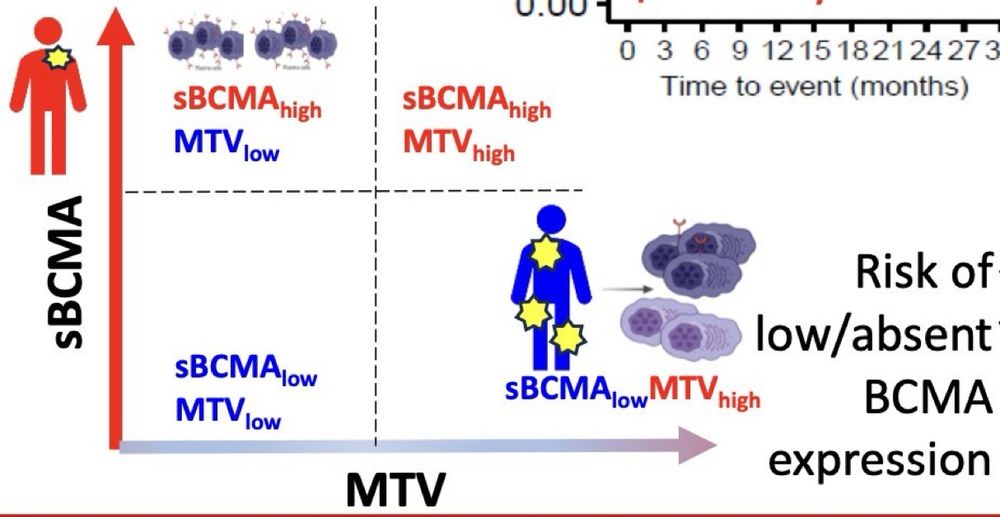
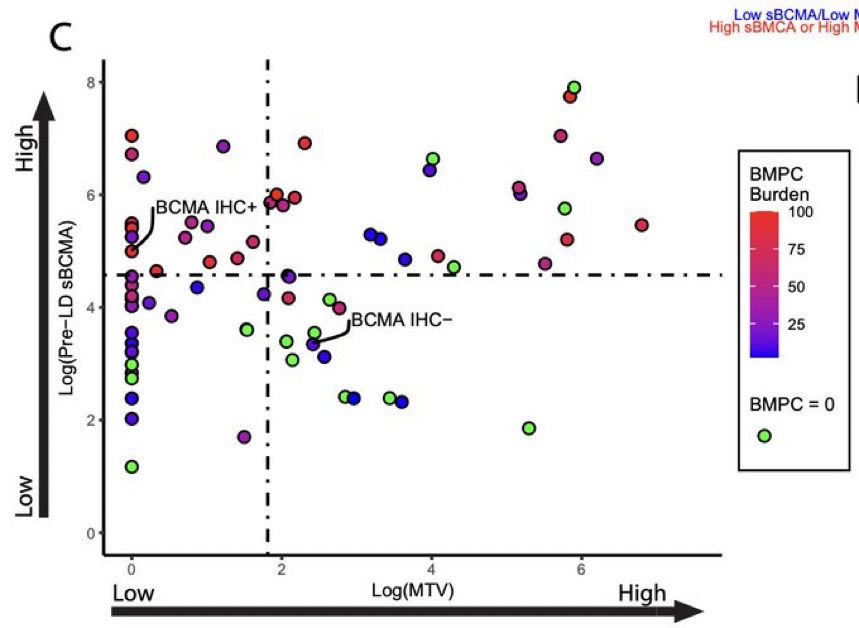
Out in @bloodjournal during #ASH24 - cool work by @freemanlciaraMD @DrFredLocke et al looking at #MMsm CAR-T in myeloma:
MTV (by PET-CT), sBCMA, BMPC don't always correlate. Some MTV-high but sBCMA-low pts exist - may not respond durably to BCMA CAR-T.
ashpublications.org/blood/articl...
MTV (by PET-CT), sBCMA, BMPC don't always correlate. Some MTV-high but sBCMA-low pts exist - may not respond durably to BCMA CAR-T.
ashpublications.org/blood/articl...
December 13, 2024 at 6:49 PM
Out in @bloodjournal during #ASH24 - cool work by @freemanlciaraMD @DrFredLocke et al looking at #MMsm CAR-T in myeloma:
MTV (by PET-CT), sBCMA, BMPC don't always correlate. Some MTV-high but sBCMA-low pts exist - may not respond durably to BCMA CAR-T.
ashpublications.org/blood/articl...
MTV (by PET-CT), sBCMA, BMPC don't always correlate. Some MTV-high but sBCMA-low pts exist - may not respond durably to BCMA CAR-T.
ashpublications.org/blood/articl...
Almost every review I've ever read about myeloma #MMsm starts with something (true) like, "Recent advances in myeloma have led to significant improvements in..."
Quite a jolt to see how different the prognosis was for myeloma 60 years ago... and how these papers used to begin!
Quite a jolt to see how different the prognosis was for myeloma 60 years ago... and how these papers used to begin!

November 30, 2024 at 5:03 AM
Almost every review I've ever read about myeloma #MMsm starts with something (true) like, "Recent advances in myeloma have led to significant improvements in..."
Quite a jolt to see how different the prognosis was for myeloma 60 years ago... and how these papers used to begin!
Quite a jolt to see how different the prognosis was for myeloma 60 years ago... and how these papers used to begin!
With my apologies to toddler parents everywhere…
“Don’t lose it, reuse it!”
Excellent @BloodAdvances work by Goel @MayoMyeloma @VincentRK @myelomaMD et al.
Re-using old myeloma #MMsm drugs can work, esp if years out.
Very relevant to post-CAR-T!
ashpublications.org/bloodadvance...
“Don’t lose it, reuse it!”
Excellent @BloodAdvances work by Goel @MayoMyeloma @VincentRK @myelomaMD et al.
Re-using old myeloma #MMsm drugs can work, esp if years out.
Very relevant to post-CAR-T!
ashpublications.org/bloodadvance...
November 19, 2024 at 9:17 PM
With my apologies to toddler parents everywhere…
“Don’t lose it, reuse it!”
Excellent @BloodAdvances work by Goel @MayoMyeloma @VincentRK @myelomaMD et al.
Re-using old myeloma #MMsm drugs can work, esp if years out.
Very relevant to post-CAR-T!
ashpublications.org/bloodadvance...
“Don’t lose it, reuse it!”
Excellent @BloodAdvances work by Goel @MayoMyeloma @VincentRK @myelomaMD et al.
Re-using old myeloma #MMsm drugs can work, esp if years out.
Very relevant to post-CAR-T!
ashpublications.org/bloodadvance...
Excellent open-access #MMsm work in @AjHematology by Zabaleta @BrunoPaiva_UNAV et al!
An important footnote for all the CAR-T vs bsAb efficacy debates: when stratified by MRD status, CAR-T and bsAbs do identically.
Getting to MRD neg is what matters!
onlinelibrary.wiley.com/doi/10.1002/...
An important footnote for all the CAR-T vs bsAb efficacy debates: when stratified by MRD status, CAR-T and bsAbs do identically.
Getting to MRD neg is what matters!
onlinelibrary.wiley.com/doi/10.1002/...

November 17, 2024 at 2:26 AM
Excellent open-access #MMsm work in @AjHematology by Zabaleta @BrunoPaiva_UNAV et al!
An important footnote for all the CAR-T vs bsAb efficacy debates: when stratified by MRD status, CAR-T and bsAbs do identically.
Getting to MRD neg is what matters!
onlinelibrary.wiley.com/doi/10.1002/...
An important footnote for all the CAR-T vs bsAb efficacy debates: when stratified by MRD status, CAR-T and bsAbs do identically.
Getting to MRD neg is what matters!
onlinelibrary.wiley.com/doi/10.1002/...
11/ #ASH24 Abstract 774 (Manier)
IFM2017-03 trial of Rd vs Dara-R with ø dex after 2 months. Huge PFS, OS, QOL benefits with #downwithdex.
Expected? Yes.
Practice-changing to make "ø dex after 2 cycles" the default control arm in #MMsm? I hope so! 🤞🏻
ash.confex.com/ash/2024/web...
IFM2017-03 trial of Rd vs Dara-R with ø dex after 2 months. Huge PFS, OS, QOL benefits with #downwithdex.
Expected? Yes.
Practice-changing to make "ø dex after 2 cycles" the default control arm in #MMsm? I hope so! 🤞🏻
ash.confex.com/ash/2024/web...

November 14, 2024 at 5:15 AM
11/ #ASH24 Abstract 774 (Manier)
IFM2017-03 trial of Rd vs Dara-R with ø dex after 2 months. Huge PFS, OS, QOL benefits with #downwithdex.
Expected? Yes.
Practice-changing to make "ø dex after 2 cycles" the default control arm in #MMsm? I hope so! 🤞🏻
ash.confex.com/ash/2024/web...
IFM2017-03 trial of Rd vs Dara-R with ø dex after 2 months. Huge PFS, OS, QOL benefits with #downwithdex.
Expected? Yes.
Practice-changing to make "ø dex after 2 cycles" the default control arm in #MMsm? I hope so! 🤞🏻
ash.confex.com/ash/2024/web...
10/ #ASH24 Abstract 773 (Dimopoulos)
🚨 AQUILA trial of dara in high-risk SMM. (Dara way more tolerated than len IMO...)
And I quote:
"60-month OS rates: DARA, 93.0%; active monitoring, 86.9%; HR, 0.52; 95% CI, 0.27-0.98)."
New approval coming soon??
ash.confex.com/ash/2024/web...
🚨 AQUILA trial of dara in high-risk SMM. (Dara way more tolerated than len IMO...)
And I quote:
"60-month OS rates: DARA, 93.0%; active monitoring, 86.9%; HR, 0.52; 95% CI, 0.27-0.98)."
New approval coming soon??
ash.confex.com/ash/2024/web...

November 14, 2024 at 5:15 AM
10/ #ASH24 Abstract 773 (Dimopoulos)
🚨 AQUILA trial of dara in high-risk SMM. (Dara way more tolerated than len IMO...)
And I quote:
"60-month OS rates: DARA, 93.0%; active monitoring, 86.9%; HR, 0.52; 95% CI, 0.27-0.98)."
New approval coming soon??
ash.confex.com/ash/2024/web...
🚨 AQUILA trial of dara in high-risk SMM. (Dara way more tolerated than len IMO...)
And I quote:
"60-month OS rates: DARA, 93.0%; active monitoring, 86.9%; HR, 0.52; 95% CI, 0.27-0.98)."
New approval coming soon??
ash.confex.com/ash/2024/web...
9/ #ASH24 Abstract 256 (Cheruvalath)
Preemptive strategy #2 to make BCMA bsAbs safer in #MMsm
Don't wait until IgG < 400 (this is myeloma, not rheumatology)... give IVIG now!
Or even start IVIG right before bsAb starts... both better than waiting!
ash.confex.com/ash/2024/web...
Preemptive strategy #2 to make BCMA bsAbs safer in #MMsm
Don't wait until IgG < 400 (this is myeloma, not rheumatology)... give IVIG now!
Or even start IVIG right before bsAb starts... both better than waiting!
ash.confex.com/ash/2024/web...

November 14, 2024 at 5:15 AM
9/ #ASH24 Abstract 256 (Cheruvalath)
Preemptive strategy #2 to make BCMA bsAbs safer in #MMsm
Don't wait until IgG < 400 (this is myeloma, not rheumatology)... give IVIG now!
Or even start IVIG right before bsAb starts... both better than waiting!
ash.confex.com/ash/2024/web...
Preemptive strategy #2 to make BCMA bsAbs safer in #MMsm
Don't wait until IgG < 400 (this is myeloma, not rheumatology)... give IVIG now!
Or even start IVIG right before bsAb starts... both better than waiting!
ash.confex.com/ash/2024/web...
8/ #ASH24 Abstract 932 (Kowalski)
Preemptive strategy #1 to make bsAbs safer in #MMsm...
PPx toci to prevent CRS. n=72, only 14% CRS and only one Gr2 event? Seems better than TEC-1 cohort for sure.
Maybe PPx toci can be cost-effective, after all!
ash.confex.com/ash/2024/web...
Preemptive strategy #1 to make bsAbs safer in #MMsm...
PPx toci to prevent CRS. n=72, only 14% CRS and only one Gr2 event? Seems better than TEC-1 cohort for sure.
Maybe PPx toci can be cost-effective, after all!
ash.confex.com/ash/2024/web...

November 14, 2024 at 5:15 AM
8/ #ASH24 Abstract 932 (Kowalski)
Preemptive strategy #1 to make bsAbs safer in #MMsm...
PPx toci to prevent CRS. n=72, only 14% CRS and only one Gr2 event? Seems better than TEC-1 cohort for sure.
Maybe PPx toci can be cost-effective, after all!
ash.confex.com/ash/2024/web...
Preemptive strategy #1 to make bsAbs safer in #MMsm...
PPx toci to prevent CRS. n=72, only 14% CRS and only one Gr2 event? Seems better than TEC-1 cohort for sure.
Maybe PPx toci can be cost-effective, after all!
ash.confex.com/ash/2024/web...
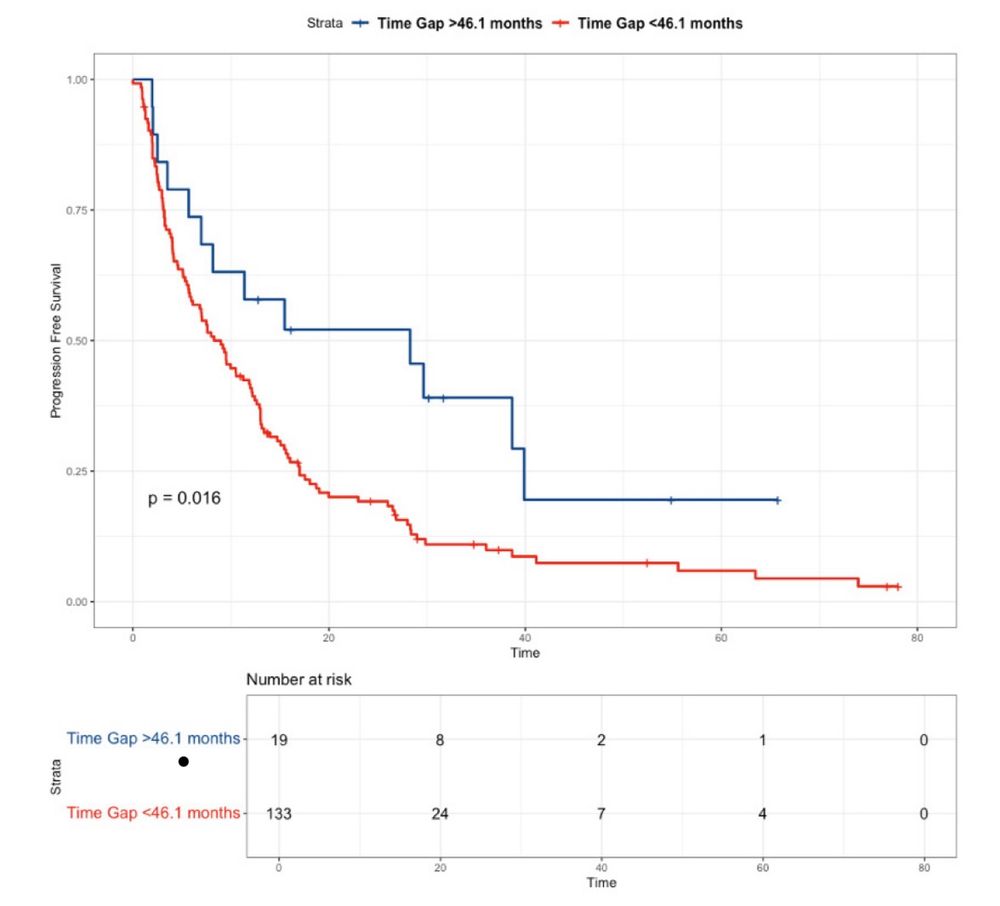
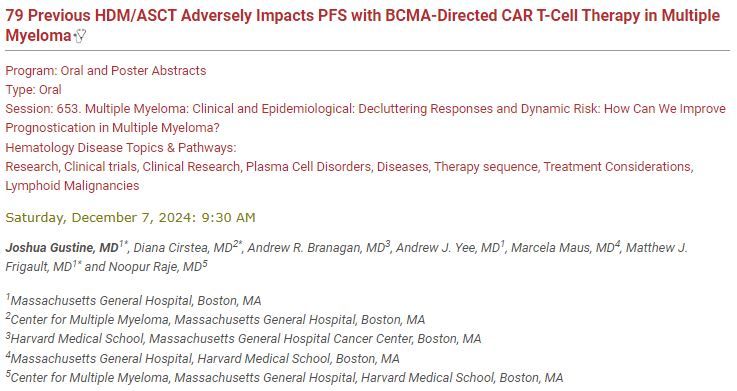
7/ #ASH24 Abstract 79 (Gustine)
BUT, are ASCT and CAR-T friends?
Possibly not (I know this is provocative)...
Might high-dose melphalan interfere with T-cell fitness & subsequent #MMsm CAR-T? This might explain PFS discordance between KarMMa-2A and –2B!
ash.confex.com/ash/2024/web...
BUT, are ASCT and CAR-T friends?
Possibly not (I know this is provocative)...
Might high-dose melphalan interfere with T-cell fitness & subsequent #MMsm CAR-T? This might explain PFS discordance between KarMMa-2A and –2B!
ash.confex.com/ash/2024/web...
November 14, 2024 at 5:15 AM
7/ #ASH24 Abstract 79 (Gustine)
BUT, are ASCT and CAR-T friends?
Possibly not (I know this is provocative)...
Might high-dose melphalan interfere with T-cell fitness & subsequent #MMsm CAR-T? This might explain PFS discordance between KarMMa-2A and –2B!
ash.confex.com/ash/2024/web...
BUT, are ASCT and CAR-T friends?
Possibly not (I know this is provocative)...
Might high-dose melphalan interfere with T-cell fitness & subsequent #MMsm CAR-T? This might explain PFS discordance between KarMMa-2A and –2B!
ash.confex.com/ash/2024/web...
6/ #ASH24 Abstract 931 (Dhakal)
bsAbs and CAR-T are friends, not foes!
Talquetamab bridging before BCMA CAR-T.
@end_myeloma: "Only place where BCMA must precede GPRC5D is dictionary."
In real life, tal's one of the best #MMsm bridging tools we have!
ash.confex.com/ash/2024/web...
bsAbs and CAR-T are friends, not foes!
Talquetamab bridging before BCMA CAR-T.
@end_myeloma: "Only place where BCMA must precede GPRC5D is dictionary."
In real life, tal's one of the best #MMsm bridging tools we have!
ash.confex.com/ash/2024/web...

November 14, 2024 at 5:15 AM
6/ #ASH24 Abstract 931 (Dhakal)
bsAbs and CAR-T are friends, not foes!
Talquetamab bridging before BCMA CAR-T.
@end_myeloma: "Only place where BCMA must precede GPRC5D is dictionary."
In real life, tal's one of the best #MMsm bridging tools we have!
ash.confex.com/ash/2024/web...
bsAbs and CAR-T are friends, not foes!
Talquetamab bridging before BCMA CAR-T.
@end_myeloma: "Only place where BCMA must precede GPRC5D is dictionary."
In real life, tal's one of the best #MMsm bridging tools we have!
ash.confex.com/ash/2024/web...
5/ #ASH24 Abstract 366 (Ikeda)
Well, can't we just replace all response assessments with sBCMA?
Maybe! It’s a great predictor of relapses, and WAY better than BMBx/imaging status quo for non-secretory #MMsm.
Now we just need validated assays & cutoffs!
ash.confex.com/ash/2024/web...
Well, can't we just replace all response assessments with sBCMA?
Maybe! It’s a great predictor of relapses, and WAY better than BMBx/imaging status quo for non-secretory #MMsm.
Now we just need validated assays & cutoffs!
ash.confex.com/ash/2024/web...

November 14, 2024 at 5:15 AM
5/ #ASH24 Abstract 366 (Ikeda)
Well, can't we just replace all response assessments with sBCMA?
Maybe! It’s a great predictor of relapses, and WAY better than BMBx/imaging status quo for non-secretory #MMsm.
Now we just need validated assays & cutoffs!
ash.confex.com/ash/2024/web...
Well, can't we just replace all response assessments with sBCMA?
Maybe! It’s a great predictor of relapses, and WAY better than BMBx/imaging status quo for non-secretory #MMsm.
Now we just need validated assays & cutoffs!
ash.confex.com/ash/2024/web...
3/ #ASH24 Abstract 83 (Claveau)
Q: Well if MRD-P is PD, what isn’t PD in #MMsm?
A: Waiting for a confirmatory set of labs... 98% of the time, single PD timepoint is sufficient.
Asking pt to return for extra labs means more #timetoxicity and no benefit.
ash.confex.com/ash/2024/web...
Q: Well if MRD-P is PD, what isn’t PD in #MMsm?
A: Waiting for a confirmatory set of labs... 98% of the time, single PD timepoint is sufficient.
Asking pt to return for extra labs means more #timetoxicity and no benefit.
ash.confex.com/ash/2024/web...

November 14, 2024 at 5:15 AM
3/ #ASH24 Abstract 83 (Claveau)
Q: Well if MRD-P is PD, what isn’t PD in #MMsm?
A: Waiting for a confirmatory set of labs... 98% of the time, single PD timepoint is sufficient.
Asking pt to return for extra labs means more #timetoxicity and no benefit.
ash.confex.com/ash/2024/web...
Q: Well if MRD-P is PD, what isn’t PD in #MMsm?
A: Waiting for a confirmatory set of labs... 98% of the time, single PD timepoint is sufficient.
Asking pt to return for extra labs means more #timetoxicity and no benefit.
ash.confex.com/ash/2024/web...
2/ #ASH24 Abstract 363 (Costa)
Is MRD ⬆️ the new PD in #MMsm?
Great work by @End_myeloma @nsc_natalie et al. "MRD-P" (10x increase in MRD by marrow NGS) basically behaves the same as biochemical PD.
Hard to tame MRD ⬆️ with CD38 triplets once occurs.
ash.confex.com/ash/2024/web...
Is MRD ⬆️ the new PD in #MMsm?
Great work by @End_myeloma @nsc_natalie et al. "MRD-P" (10x increase in MRD by marrow NGS) basically behaves the same as biochemical PD.
Hard to tame MRD ⬆️ with CD38 triplets once occurs.
ash.confex.com/ash/2024/web...

November 14, 2024 at 5:15 AM
2/ #ASH24 Abstract 363 (Costa)
Is MRD ⬆️ the new PD in #MMsm?
Great work by @End_myeloma @nsc_natalie et al. "MRD-P" (10x increase in MRD by marrow NGS) basically behaves the same as biochemical PD.
Hard to tame MRD ⬆️ with CD38 triplets once occurs.
ash.confex.com/ash/2024/web...
Is MRD ⬆️ the new PD in #MMsm?
Great work by @End_myeloma @nsc_natalie et al. "MRD-P" (10x increase in MRD by marrow NGS) basically behaves the same as biochemical PD.
Hard to tame MRD ⬆️ with CD38 triplets once occurs.
ash.confex.com/ash/2024/web...
1/ #ASH24 Choosing my top 10 myeloma abstracts this year was harder than ever!! Kudos to all @ASH_hematology authors for GREAT work 👏
For simplicity, I excluded investigational drugs and focused on:
1️⃣ #MMsm response assessments
2️⃣ Optimizing bsAbs
3️⃣ (Soon) practice-changing
For simplicity, I excluded investigational drugs and focused on:
1️⃣ #MMsm response assessments
2️⃣ Optimizing bsAbs
3️⃣ (Soon) practice-changing

November 14, 2024 at 5:15 AM
1/ And since we can’t tweet during #IMS24, also worth highlighting CEPHEUS as another LBA!
D-VRd vs VRd in ASCT-ineligible #MMsm - large PFS benefit with CD38 addition even if no ASCT. Love simplicity of the last line: ASCT decision-making should not dictate induction choice!
D-VRd vs VRd in ASCT-ineligible #MMsm - large PFS benefit with CD38 addition even if no ASCT. Love simplicity of the last line: ASCT decision-making should not dictate induction choice!

September 8, 2024 at 1:30 PM
