



Psych Scene
@psychscene.bsky.social
We provide psychiatry education for Psychiatrists, GPs & Mental Health Practitioners.
Autism isn’t “just genetic”.
The gut–brain–immune axis can shape how symptoms show up—especially when GI problems are in the mix.
Here’s what clinicians needs to know about Gut Microbiome and Autism Spectrum Disorder (ASD) 👇🧵
The gut–brain–immune axis can shape how symptoms show up—especially when GI problems are in the mix.
Here’s what clinicians needs to know about Gut Microbiome and Autism Spectrum Disorder (ASD) 👇🧵

December 5, 2025 at 1:32 PM
Autism isn’t “just genetic”.
The gut–brain–immune axis can shape how symptoms show up—especially when GI problems are in the mix.
Here’s what clinicians needs to know about Gut Microbiome and Autism Spectrum Disorder (ASD) 👇🧵
The gut–brain–immune axis can shape how symptoms show up—especially when GI problems are in the mix.
Here’s what clinicians needs to know about Gut Microbiome and Autism Spectrum Disorder (ASD) 👇🧵
Here’s what one of your colleagues is saying about our course Focussed Psychological Strategies: Advanced CPD Training for General Practitioners (RACGP) 👇

December 1, 2025 at 4:01 AM
Here’s what one of your colleagues is saying about our course Focussed Psychological Strategies: Advanced CPD Training for General Practitioners (RACGP) 👇
Here’s what clinicians are saying about the course: Dialectical Behaviour Therapy - A Practical Guide for Clinicians.

November 22, 2025 at 5:01 AM
Here’s what clinicians are saying about the course: Dialectical Behaviour Therapy - A Practical Guide for Clinicians.
This curriculum offers diagnostic clarity and management strategies for melancholic, psychotic, and mixed-feature depression.

November 15, 2025 at 7:23 AM
This curriculum offers diagnostic clarity and management strategies for melancholic, psychotic, and mixed-feature depression.
Here’s what your colleague has to say about our course: “The Art of Strategic Problem Solving in Psychiatry – From Diagnostic Formulation to Management”:

November 8, 2025 at 2:09 PM
Here’s what your colleague has to say about our course: “The Art of Strategic Problem Solving in Psychiatry – From Diagnostic Formulation to Management”:
GAD-7 Self-Assessment
This diagnostic tool detects a patient’s latent anxiety.
These items are answered by frequency (not at all, most days, etc.)
[Spitzer et al., 2006]
This diagnostic tool detects a patient’s latent anxiety.
These items are answered by frequency (not at all, most days, etc.)
[Spitzer et al., 2006]
November 4, 2025 at 2:42 PM
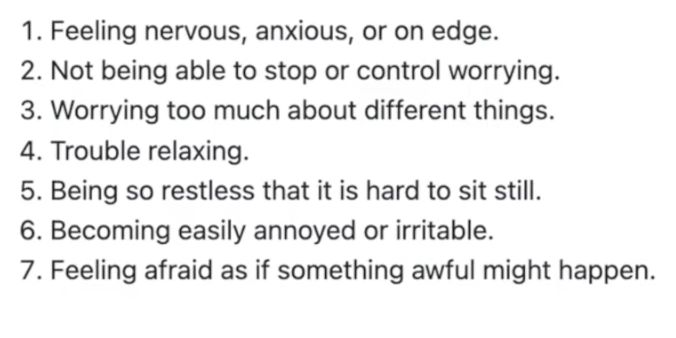
GAD-7 Self-Assessment
This diagnostic tool detects a patient’s latent anxiety.
These items are answered by frequency (not at all, most days, etc.)
[Spitzer et al., 2006]
This diagnostic tool detects a patient’s latent anxiety.
These items are answered by frequency (not at all, most days, etc.)
[Spitzer et al., 2006]
DSM-5 anchors you can count.
Excessive worry more days than not for ≥6 months about multiple domains, difficult to control.
Plus ≥3 of restlessness, fatigue, poor concentration/mind blank, irritability, muscle tension, and sleep disturbance.
Excessive worry more days than not for ≥6 months about multiple domains, difficult to control.
Plus ≥3 of restlessness, fatigue, poor concentration/mind blank, irritability, muscle tension, and sleep disturbance.

November 4, 2025 at 2:42 PM
DSM-5 anchors you can count.
Excessive worry more days than not for ≥6 months about multiple domains, difficult to control.
Plus ≥3 of restlessness, fatigue, poor concentration/mind blank, irritability, muscle tension, and sleep disturbance.
Excessive worry more days than not for ≥6 months about multiple domains, difficult to control.
Plus ≥3 of restlessness, fatigue, poor concentration/mind blank, irritability, muscle tension, and sleep disturbance.
Chelsea, 20, says she’s “going mad with anxiety.”
Onset with VCE exams; now pervasive worry, decision paralysis, and no depressive features.
You suspect GAD.
What would you do to confirm this? 👇
Onset with VCE exams; now pervasive worry, decision paralysis, and no depressive features.
You suspect GAD.
What would you do to confirm this? 👇

November 4, 2025 at 2:42 PM
Chelsea, 20, says she’s “going mad with anxiety.”
Onset with VCE exams; now pervasive worry, decision paralysis, and no depressive features.
You suspect GAD.
What would you do to confirm this? 👇
Onset with VCE exams; now pervasive worry, decision paralysis, and no depressive features.
You suspect GAD.
What would you do to confirm this? 👇
Females with ADHD are often underdiagnosed and undertreated, forming a silent minority.
Research shows a significant male-to-female diagnosis gap (Berry et al., 1985).
Let’s explore why ADHD presents differently in females.
Research shows a significant male-to-female diagnosis gap (Berry et al., 1985).
Let’s explore why ADHD presents differently in females.

November 3, 2025 at 5:19 AM
Females with ADHD are often underdiagnosed and undertreated, forming a silent minority.
Research shows a significant male-to-female diagnosis gap (Berry et al., 1985).
Let’s explore why ADHD presents differently in females.
Research shows a significant male-to-female diagnosis gap (Berry et al., 1985).
Let’s explore why ADHD presents differently in females.
Females with ADHD are often underdiagnosed and undertreated, forming a silent minority.
Research shows a significant male-to-female diagnosis gap (Berry et al., 1985).
Let’s explore why ADHD presents differently in females.
Research shows a significant male-to-female diagnosis gap (Berry et al., 1985).
Let’s explore why ADHD presents differently in females.
November 3, 2025 at 5:18 AM
Females with ADHD are often underdiagnosed and undertreated, forming a silent minority.
Research shows a significant male-to-female diagnosis gap (Berry et al., 1985).
Let’s explore why ADHD presents differently in females.
Research shows a significant male-to-female diagnosis gap (Berry et al., 1985).
Let’s explore why ADHD presents differently in females.
What would change today if Phenomenology and Pharmacology were your primary safety tools?
Miss one, and you may miss risk.
Here’s what to look for and how to act 👇🧵
Miss one, and you may miss risk.
Here’s what to look for and how to act 👇🧵

November 1, 2025 at 3:14 AM
What would change today if Phenomenology and Pharmacology were your primary safety tools?
Miss one, and you may miss risk.
Here’s what to look for and how to act 👇🧵
Miss one, and you may miss risk.
Here’s what to look for and how to act 👇🧵
What would change today if Phenomenology and Pharmacology were your primary safety tools?
Miss one, and you may miss risk.
Here’s what to look for and how to act 👇🧵
Miss one, and you may miss risk.
Here’s what to look for and how to act 👇🧵
November 1, 2025 at 3:14 AM
What would change today if Phenomenology and Pharmacology were your primary safety tools?
Miss one, and you may miss risk.
Here’s what to look for and how to act 👇🧵
Miss one, and you may miss risk.
Here’s what to look for and how to act 👇🧵
Want to go deeper into the neurobiology of ADHD?
Join Dr Sanil Rege for the ADHD Masterclass: From Neurobiology to Clinical Practice on the 29th of November:
https://learn.psychscene.com/adhdmasterclasslive
Join Dr Sanil Rege for the ADHD Masterclass: From Neurobiology to Clinical Practice on the 29th of November:
https://learn.psychscene.com/adhdmasterclasslive

October 11, 2025 at 2:30 AM
Want to go deeper into the neurobiology of ADHD?
Join Dr Sanil Rege for the ADHD Masterclass: From Neurobiology to Clinical Practice on the 29th of November:
https://learn.psychscene.com/adhdmasterclasslive
Join Dr Sanil Rege for the ADHD Masterclass: From Neurobiology to Clinical Practice on the 29th of November:
https://learn.psychscene.com/adhdmasterclasslive
Bottom-Up 'Competition'
Bottom-up circuits respond to salience: movement, novelty, reward.
In ADHD, underactive prefrontal regulation means bottom-up inputs (e.g. phone alerts, noise) more easily capture attention.
Bottom-up circuits respond to salience: movement, novelty, reward.
In ADHD, underactive prefrontal regulation means bottom-up inputs (e.g. phone alerts, noise) more easily capture attention.

October 11, 2025 at 2:30 AM
Bottom-Up 'Competition'
Bottom-up circuits respond to salience: movement, novelty, reward.
In ADHD, underactive prefrontal regulation means bottom-up inputs (e.g. phone alerts, noise) more easily capture attention.
Bottom-up circuits respond to salience: movement, novelty, reward.
In ADHD, underactive prefrontal regulation means bottom-up inputs (e.g. phone alerts, noise) more easily capture attention.
The prefrontal cortex (PFC) directs top-down attention, choosing what’s relevant, suppressing distraction, and maintaining goal-oriented focus.
When this system falters, stimulus-driven (“bottom-up”) networks dominate, explaining distractibility and inconsistent attention in ADHD.
When this system falters, stimulus-driven (“bottom-up”) networks dominate, explaining distractibility and inconsistent attention in ADHD.

October 11, 2025 at 2:30 AM
The prefrontal cortex (PFC) directs top-down attention, choosing what’s relevant, suppressing distraction, and maintaining goal-oriented focus.
When this system falters, stimulus-driven (“bottom-up”) networks dominate, explaining distractibility and inconsistent attention in ADHD.
When this system falters, stimulus-driven (“bottom-up”) networks dominate, explaining distractibility and inconsistent attention in ADHD.
ADHD isn’t just an “attention” problem.
It’s impaired prefrontal regulation across distributed circuits that shape attention, inhibition, and emotion.
Here’s how these circuits interact and what clinicians need to know about the neurobiology behind ADHD 🧵👇
It’s impaired prefrontal regulation across distributed circuits that shape attention, inhibition, and emotion.
Here’s how these circuits interact and what clinicians need to know about the neurobiology behind ADHD 🧵👇

October 11, 2025 at 2:30 AM
ADHD isn’t just an “attention” problem.
It’s impaired prefrontal regulation across distributed circuits that shape attention, inhibition, and emotion.
Here’s how these circuits interact and what clinicians need to know about the neurobiology behind ADHD 🧵👇
It’s impaired prefrontal regulation across distributed circuits that shape attention, inhibition, and emotion.
Here’s how these circuits interact and what clinicians need to know about the neurobiology behind ADHD 🧵👇
Explore our deep dive: “Navigating Female-Specific Complexities in Psychiatry” on Psych Scene Hub 👇
https://psychscene.co/4nIEfTu
https://psychscene.co/4nIEfTu

September 28, 2025 at 4:11 PM
Explore our deep dive: “Navigating Female-Specific Complexities in Psychiatry” on Psych Scene Hub 👇
https://psychscene.co/4nIEfTu
https://psychscene.co/4nIEfTu
Men are 1.4× more likely to develop schizophrenia, with onset 3–4 years earlier (Li, 2022).
Oestrogen delays onset in women—but symptoms surge after menopause.
Here’s how hormones shape outcomes + guide care. 👇🧵
Oestrogen delays onset in women—but symptoms surge after menopause.
Here’s how hormones shape outcomes + guide care. 👇🧵

September 28, 2025 at 4:11 PM
Men are 1.4× more likely to develop schizophrenia, with onset 3–4 years earlier (Li, 2022).
Oestrogen delays onset in women—but symptoms surge after menopause.
Here’s how hormones shape outcomes + guide care. 👇🧵
Oestrogen delays onset in women—but symptoms surge after menopause.
Here’s how hormones shape outcomes + guide care. 👇🧵
Why do hot flushes happen in menopause?

September 27, 2025 at 2:02 PM
Why do hot flushes happen in menopause?
Want to learn more about recognising and managing dissociation in PTSD?
Check out our evidence-based course, “PTSD & Complex PTSD: Advanced Clinical Training for Psychiatrists & Clinicians” on The Academy:
https://psychscene.co/4niwl3s
Check out our evidence-based course, “PTSD & Complex PTSD: Advanced Clinical Training for Psychiatrists & Clinicians” on The Academy:
https://psychscene.co/4niwl3s

September 25, 2025 at 1:31 PM
Want to learn more about recognising and managing dissociation in PTSD?
Check out our evidence-based course, “PTSD & Complex PTSD: Advanced Clinical Training for Psychiatrists & Clinicians” on The Academy:
https://psychscene.co/4niwl3s
Check out our evidence-based course, “PTSD & Complex PTSD: Advanced Clinical Training for Psychiatrists & Clinicians” on The Academy:
https://psychscene.co/4niwl3s
Fear & memory circuits:
Amygdala → acute fear.
BNST → sustained anxiety.
Hippocampal dysfunction → poor trauma contextualisation.
Dissociation disrupts these networks, leaving patients stuck in hyperarousal or shutdown.
Amygdala → acute fear.
BNST → sustained anxiety.
Hippocampal dysfunction → poor trauma contextualisation.
Dissociation disrupts these networks, leaving patients stuck in hyperarousal or shutdown.

September 25, 2025 at 1:31 PM
Fear & memory circuits:
Amygdala → acute fear.
BNST → sustained anxiety.
Hippocampal dysfunction → poor trauma contextualisation.
Dissociation disrupts these networks, leaving patients stuck in hyperarousal or shutdown.
Amygdala → acute fear.
BNST → sustained anxiety.
Hippocampal dysfunction → poor trauma contextualisation.
Dissociation disrupts these networks, leaving patients stuck in hyperarousal or shutdown.
Neurobiology of the dissociative subtype:
🔹 Excess inhibition of the amygdala by the medial prefrontal cortex.
🔹 Over-regulation of fear → emotional numbing, detachment.
Psych Scene Tip: therapies that restore limbic-prefrontal balance (e.g., somatic and trauma-focused approaches) can help.
🔹 Excess inhibition of the amygdala by the medial prefrontal cortex.
🔹 Over-regulation of fear → emotional numbing, detachment.
Psych Scene Tip: therapies that restore limbic-prefrontal balance (e.g., somatic and trauma-focused approaches) can help.

September 25, 2025 at 1:31 PM
Neurobiology of the dissociative subtype:
🔹 Excess inhibition of the amygdala by the medial prefrontal cortex.
🔹 Over-regulation of fear → emotional numbing, detachment.
Psych Scene Tip: therapies that restore limbic-prefrontal balance (e.g., somatic and trauma-focused approaches) can help.
🔹 Excess inhibition of the amygdala by the medial prefrontal cortex.
🔹 Over-regulation of fear → emotional numbing, detachment.
Psych Scene Tip: therapies that restore limbic-prefrontal balance (e.g., somatic and trauma-focused approaches) can help.
The Defence Cascade (Schauer & Elbert, 2010):
Freeze → Flight → Fight → Fright → Flag → Faint.
Dissociation arises in fright/flag/faint when parasympathetic dominance triggers shutdown, immobility, and numbing.
Tracking shifts in arousal helps clinicians intervene.
Freeze → Flight → Fight → Fright → Flag → Faint.
Dissociation arises in fright/flag/faint when parasympathetic dominance triggers shutdown, immobility, and numbing.
Tracking shifts in arousal helps clinicians intervene.

September 25, 2025 at 1:30 PM
The Defence Cascade (Schauer & Elbert, 2010):
Freeze → Flight → Fight → Fright → Flag → Faint.
Dissociation arises in fright/flag/faint when parasympathetic dominance triggers shutdown, immobility, and numbing.
Tracking shifts in arousal helps clinicians intervene.
Freeze → Flight → Fight → Fright → Flag → Faint.
Dissociation arises in fright/flag/faint when parasympathetic dominance triggers shutdown, immobility, and numbing.
Tracking shifts in arousal helps clinicians intervene.
Two PTSD phenotypes:
1️⃣ Emotional undermodulation → hyperarousal, re-experiencing.
2️⃣ Emotional overmodulation → numbing, detachment, dissociation.
Understanding these helps match interventions:
- grounding for hyperarousal
- stabilisation before trauma processing in dissociation.
1️⃣ Emotional undermodulation → hyperarousal, re-experiencing.
2️⃣ Emotional overmodulation → numbing, detachment, dissociation.
Understanding these helps match interventions:
- grounding for hyperarousal
- stabilisation before trauma processing in dissociation.

September 25, 2025 at 1:30 PM
Two PTSD phenotypes:
1️⃣ Emotional undermodulation → hyperarousal, re-experiencing.
2️⃣ Emotional overmodulation → numbing, detachment, dissociation.
Understanding these helps match interventions:
- grounding for hyperarousal
- stabilisation before trauma processing in dissociation.
1️⃣ Emotional undermodulation → hyperarousal, re-experiencing.
2️⃣ Emotional overmodulation → numbing, detachment, dissociation.
Understanding these helps match interventions:
- grounding for hyperarousal
- stabilisation before trauma processing in dissociation.
Is dissociation in PTSD just a symptom, or the brain’s survival strategy?
Around 15–30% of patients with PTSD experience dissociative symptoms such as depersonalisation or derealisation.
Let’s discover why recognising dissociation is critical for tailoring therapy and improving outcomes. 👇🧵
Around 15–30% of patients with PTSD experience dissociative symptoms such as depersonalisation or derealisation.
Let’s discover why recognising dissociation is critical for tailoring therapy and improving outcomes. 👇🧵

September 25, 2025 at 1:30 PM
Is dissociation in PTSD just a symptom, or the brain’s survival strategy?
Around 15–30% of patients with PTSD experience dissociative symptoms such as depersonalisation or derealisation.
Let’s discover why recognising dissociation is critical for tailoring therapy and improving outcomes. 👇🧵
Around 15–30% of patients with PTSD experience dissociative symptoms such as depersonalisation or derealisation.
Let’s discover why recognising dissociation is critical for tailoring therapy and improving outcomes. 👇🧵