




MondayNightIBD
@mondaynightibd.bsky.social
Created by @dcharabaty.bsky.social
🧵Every other MONDAY @ 5p ET ~ Join us here for #Back2Basics IBD threads
🎙️Join us on Twitter for #IBD #IBDPoll & convo ~ #PatientExperience WED ~ #IBDAlgorithm THUR
Opinions≠med advice
🆓 #CME bit.ly/MNIBD24-25
🧵Every other MONDAY @ 5p ET ~ Join us here for #Back2Basics IBD threads
🎙️Join us on Twitter for #IBD #IBDPoll & convo ~ #PatientExperience WED ~ #IBDAlgorithm THUR
Opinions≠med advice
🆓 #CME bit.ly/MNIBD24-25
12/ICIs can cause diarrhea & serious enterocolitis
🔹🗝️Recognize & TxT early
🔹Work-up: labs,💩,🔦w/ bx
🔹Severity grading guides treatment: supportive -> budesonide/PO pred -> IV steroids -> biologics
🔹Resuming ICI depends on irAE severity, TxT response & oncologic benefits
🔹🗝️Recognize & TxT early
🔹Work-up: labs,💩,🔦w/ bx
🔹Severity grading guides treatment: supportive -> budesonide/PO pred -> IV steroids -> biologics
🔹Resuming ICI depends on irAE severity, TxT response & oncologic benefits

April 15, 2025 at 8:21 PM
12/ICIs can cause diarrhea & serious enterocolitis
🔹🗝️Recognize & TxT early
🔹Work-up: labs,💩,🔦w/ bx
🔹Severity grading guides treatment: supportive -> budesonide/PO pred -> IV steroids -> biologics
🔹Resuming ICI depends on irAE severity, TxT response & oncologic benefits
🔹🗝️Recognize & TxT early
🔹Work-up: labs,💩,🔦w/ bx
🔹Severity grading guides treatment: supportive -> budesonide/PO pred -> IV steroids -> biologics
🔹Resuming ICI depends on irAE severity, TxT response & oncologic benefits
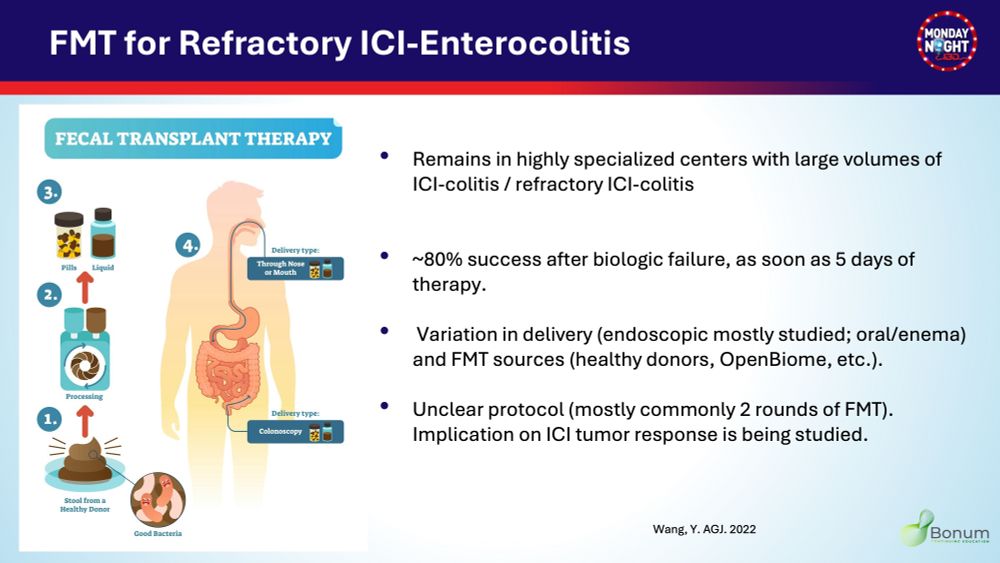
11/ If refractory to IFX and/or Vedo
🔹UST: 97% clinical remission after 1 bio-failure, 54% after 2 bio-failures
🔹JAKi used in case series
🔹FMT In specialized🏥: 80% Response, as soon as day 5
pmc.ncbi.nlm.nih.gov/articles/PMC...
🔹UST: 97% clinical remission after 1 bio-failure, 54% after 2 bio-failures
🔹JAKi used in case series
🔹FMT In specialized🏥: 80% Response, as soon as day 5
pmc.ncbi.nlm.nih.gov/articles/PMC...


April 15, 2025 at 8:21 PM
11/ If refractory to IFX and/or Vedo
🔹UST: 97% clinical remission after 1 bio-failure, 54% after 2 bio-failures
🔹JAKi used in case series
🔹FMT In specialized🏥: 80% Response, as soon as day 5
pmc.ncbi.nlm.nih.gov/articles/PMC...
🔹UST: 97% clinical remission after 1 bio-failure, 54% after 2 bio-failures
🔹JAKi used in case series
🔹FMT In specialized🏥: 80% Response, as soon as day 5
pmc.ncbi.nlm.nih.gov/articles/PMC...
10/⚠️Better outcomes if:
✅⏲️ Earlier scope, steroids & biologic use
✅Total 3 biologic induction doses vs 1
✅Endo remission
⚖️IFX vs Vedo?
✅ Favor IFX if high-risk endo features
✅Overall survival Vedo>IFX
✅Cancer progression Vedo<IFX
✅⏲️ Earlier scope, steroids & biologic use
✅Total 3 biologic induction doses vs 1
✅Endo remission
⚖️IFX vs Vedo?
✅ Favor IFX if high-risk endo features
✅Overall survival Vedo>IFX
✅Cancer progression Vedo<IFX

April 15, 2025 at 8:21 PM
10/⚠️Better outcomes if:
✅⏲️ Earlier scope, steroids & biologic use
✅Total 3 biologic induction doses vs 1
✅Endo remission
⚖️IFX vs Vedo?
✅ Favor IFX if high-risk endo features
✅Overall survival Vedo>IFX
✅Cancer progression Vedo<IFX
✅⏲️ Earlier scope, steroids & biologic use
✅Total 3 biologic induction doses vs 1
✅Endo remission
⚖️IFX vs Vedo?
✅ Favor IFX if high-risk endo features
✅Overall survival Vedo>IFX
✅Cancer progression Vedo<IFX
9/ Management
🔹If steroids response➡️ 4-8wks taper
🔹Start biologic IFX/Vedo if:
✅No/Partial response to IV steroids on day3
✅Recurrence w steroids taper
✅🔦 ulcerations, extensive dis
www.sciencedirect.com/science/arti...
🔹If steroids response➡️ 4-8wks taper
🔹Start biologic IFX/Vedo if:
✅No/Partial response to IV steroids on day3
✅Recurrence w steroids taper
✅🔦 ulcerations, extensive dis
www.sciencedirect.com/science/arti...
April 15, 2025 at 8:21 PM
9/ Management
🔹If steroids response➡️ 4-8wks taper
🔹Start biologic IFX/Vedo if:
✅No/Partial response to IV steroids on day3
✅Recurrence w steroids taper
✅🔦 ulcerations, extensive dis
www.sciencedirect.com/science/arti...
🔹If steroids response➡️ 4-8wks taper
🔹Start biologic IFX/Vedo if:
✅No/Partial response to IV steroids on day3
✅Recurrence w steroids taper
✅🔦 ulcerations, extensive dis
www.sciencedirect.com/science/arti...
8/ Management
G1:Keep ICI, Loperamide,🔽 fiber diet,🥤,Budesonide
G2:Hold ICI, eval for colitis, prednisone 1mg/kg/d
G3/4: as above +🏥 , IV solumedrol 1-2mg/kg/d, if not better at day 3-5→IFX or Vedo
🔦If high risk endo features (deep or large ulcers, extensive dis)➡️ biologics
G1:Keep ICI, Loperamide,🔽 fiber diet,🥤,Budesonide
G2:Hold ICI, eval for colitis, prednisone 1mg/kg/d
G3/4: as above +🏥 , IV solumedrol 1-2mg/kg/d, if not better at day 3-5→IFX or Vedo
🔦If high risk endo features (deep or large ulcers, extensive dis)➡️ biologics


April 15, 2025 at 8:21 PM
8/ Management
G1:Keep ICI, Loperamide,🔽 fiber diet,🥤,Budesonide
G2:Hold ICI, eval for colitis, prednisone 1mg/kg/d
G3/4: as above +🏥 , IV solumedrol 1-2mg/kg/d, if not better at day 3-5→IFX or Vedo
🔦If high risk endo features (deep or large ulcers, extensive dis)➡️ biologics
G1:Keep ICI, Loperamide,🔽 fiber diet,🥤,Budesonide
G2:Hold ICI, eval for colitis, prednisone 1mg/kg/d
G3/4: as above +🏥 , IV solumedrol 1-2mg/kg/d, if not better at day 3-5→IFX or Vedo
🔦If high risk endo features (deep or large ulcers, extensive dis)➡️ biologics
7/ Endoscopic🔦findings in ICI colitis range from normal to IBD-like
🔬Histo: destructive pattern w crypt/epithelial apoptosis; acute/chronic inflam, cryptitis & crypt architecture distortion
📌Can mimic microscopic colitis or celiac
⚠️Always biopsy—even if mucosa looks normal
🔬Histo: destructive pattern w crypt/epithelial apoptosis; acute/chronic inflam, cryptitis & crypt architecture distortion
📌Can mimic microscopic colitis or celiac
⚠️Always biopsy—even if mucosa looks normal

April 15, 2025 at 8:21 PM
7/ Endoscopic🔦findings in ICI colitis range from normal to IBD-like
🔬Histo: destructive pattern w crypt/epithelial apoptosis; acute/chronic inflam, cryptitis & crypt architecture distortion
📌Can mimic microscopic colitis or celiac
⚠️Always biopsy—even if mucosa looks normal
🔬Histo: destructive pattern w crypt/epithelial apoptosis; acute/chronic inflam, cryptitis & crypt architecture distortion
📌Can mimic microscopic colitis or celiac
⚠️Always biopsy—even if mucosa looks normal
6/ Initial work-up for suspected ICI colitis includes:
🧪 CBC, CMP, CRP
🦠 Stool studies: C. diff, culture, Giardia
🧫 Fecal calprotectin/lactoferrin
🔦Scope: at least Flex sig, prefer EGD/CLN w bx
🔍 TB test, hepatitis B screen before starting biologic
🧪 CBC, CMP, CRP
🦠 Stool studies: C. diff, culture, Giardia
🧫 Fecal calprotectin/lactoferrin
🔦Scope: at least Flex sig, prefer EGD/CLN w bx
🔍 TB test, hepatitis B screen before starting biologic

April 15, 2025 at 8:21 PM
6/ Initial work-up for suspected ICI colitis includes:
🧪 CBC, CMP, CRP
🦠 Stool studies: C. diff, culture, Giardia
🧫 Fecal calprotectin/lactoferrin
🔦Scope: at least Flex sig, prefer EGD/CLN w bx
🔍 TB test, hepatitis B screen before starting biologic
🧪 CBC, CMP, CRP
🦠 Stool studies: C. diff, culture, Giardia
🧫 Fecal calprotectin/lactoferrin
🔦Scope: at least Flex sig, prefer EGD/CLN w bx
🔍 TB test, hepatitis B screen before starting biologic
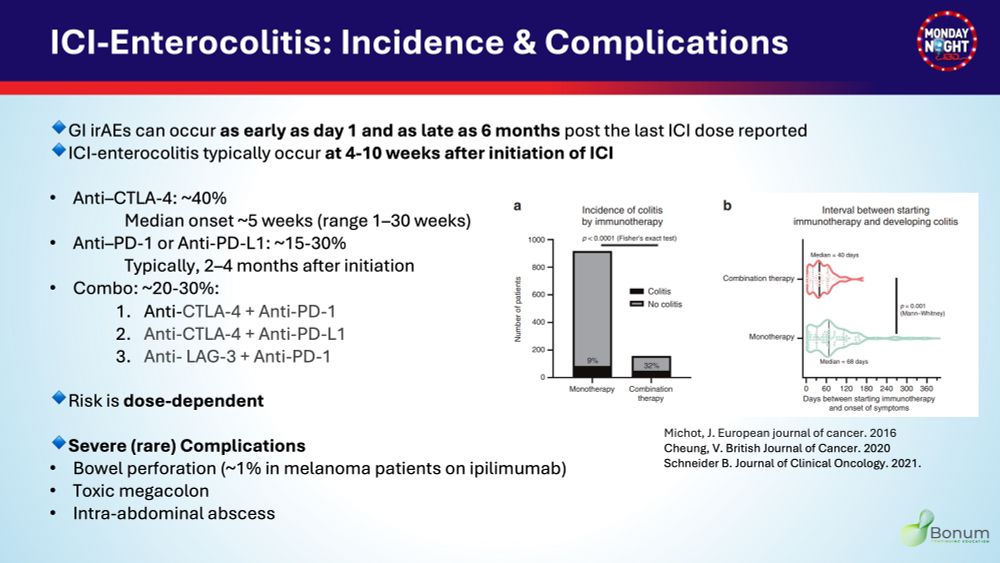
5/ ICI-induced enterocolitis:
🔹Incidence & interval between starting ICI & developing colitis vary by agent
⬆️risk w ⬆️ICI dose
⬆️risk & earlier onset w ICI combo vs monotherapy
⚠️ Can progress rapidly -> complications: perforation, toxic megacolon, Intra-abdominal abscess
#Back2Basics
🔹Incidence & interval between starting ICI & developing colitis vary by agent
⬆️risk w ⬆️ICI dose
⬆️risk & earlier onset w ICI combo vs monotherapy
⚠️ Can progress rapidly -> complications: perforation, toxic megacolon, Intra-abdominal abscess
#Back2Basics
April 15, 2025 at 8:21 PM
5/ ICI-induced enterocolitis:
🔹Incidence & interval between starting ICI & developing colitis vary by agent
⬆️risk w ⬆️ICI dose
⬆️risk & earlier onset w ICI combo vs monotherapy
⚠️ Can progress rapidly -> complications: perforation, toxic megacolon, Intra-abdominal abscess
#Back2Basics
🔹Incidence & interval between starting ICI & developing colitis vary by agent
⬆️risk w ⬆️ICI dose
⬆️risk & earlier onset w ICI combo vs monotherapy
⚠️ Can progress rapidly -> complications: perforation, toxic megacolon, Intra-abdominal abscess
#Back2Basics
4/ CTCAE grading of ICI-diarrhea & ICI-colitis severity:
⬆️in # of BM/day over baseline (or⬆️ostomy output)
🔹Abdo pain, blood in stool
🔹Fever, HE instability, 🏥, peritoneal signs
#Back2Basics
⬆️in # of BM/day over baseline (or⬆️ostomy output)
🔹Abdo pain, blood in stool
🔹Fever, HE instability, 🏥, peritoneal signs
#Back2Basics

April 15, 2025 at 8:21 PM
4/ CTCAE grading of ICI-diarrhea & ICI-colitis severity:
⬆️in # of BM/day over baseline (or⬆️ostomy output)
🔹Abdo pain, blood in stool
🔹Fever, HE instability, 🏥, peritoneal signs
#Back2Basics
⬆️in # of BM/day over baseline (or⬆️ostomy output)
🔹Abdo pain, blood in stool
🔹Fever, HE instability, 🏥, peritoneal signs
#Back2Basics
3/It's important to recognize that ICI can cause diarrhea without colitis
🔹% ICI-diarrhea > %ICI-colitis
⚠️ Confirm colitis vs simple diarrhea to
❌Avoid over-use of steroids
❌Avoid missing colitis dx:
⚠️Earlier scope & treatment= better prognosis
doi.org/10.1016/j.ct...
#Back2Basics
🔹% ICI-diarrhea > %ICI-colitis
⚠️ Confirm colitis vs simple diarrhea to
❌Avoid over-use of steroids
❌Avoid missing colitis dx:
⚠️Earlier scope & treatment= better prognosis
doi.org/10.1016/j.ct...
#Back2Basics

April 15, 2025 at 8:21 PM
3/It's important to recognize that ICI can cause diarrhea without colitis
🔹% ICI-diarrhea > %ICI-colitis
⚠️ Confirm colitis vs simple diarrhea to
❌Avoid over-use of steroids
❌Avoid missing colitis dx:
⚠️Earlier scope & treatment= better prognosis
doi.org/10.1016/j.ct...
#Back2Basics
🔹% ICI-diarrhea > %ICI-colitis
⚠️ Confirm colitis vs simple diarrhea to
❌Avoid over-use of steroids
❌Avoid missing colitis dx:
⚠️Earlier scope & treatment= better prognosis
doi.org/10.1016/j.ct...
#Back2Basics
2/⚠️ T cells activated by ICI can cross-react w normal tissue -> Autoimmune-like phenomena called immune-related adverse events (irAEs)
💩GI, skin, liver, lungs, & endocrine systems are most commonly affected
⌛️ Organ specific irAEs occur at different time from ICI initiation
#Back2Basics
💩GI, skin, liver, lungs, & endocrine systems are most commonly affected
⌛️ Organ specific irAEs occur at different time from ICI initiation
#Back2Basics

April 15, 2025 at 8:21 PM
2/⚠️ T cells activated by ICI can cross-react w normal tissue -> Autoimmune-like phenomena called immune-related adverse events (irAEs)
💩GI, skin, liver, lungs, & endocrine systems are most commonly affected
⌛️ Organ specific irAEs occur at different time from ICI initiation
#Back2Basics
💩GI, skin, liver, lungs, & endocrine systems are most commonly affected
⌛️ Organ specific irAEs occur at different time from ICI initiation
#Back2Basics
1/ 🔹Immune checkpoints like CTLA-4, PD-1,PD-L1 AND LAG-3 suppress T-cell activity -> cancer cells evade immune anti-tumor response
🔹IC inhibitors (ICI)➡️ Reactivation T-cell response to CA
➡️ improved survival across many cancers
#Back2Basics
🔹IC inhibitors (ICI)➡️ Reactivation T-cell response to CA
➡️ improved survival across many cancers
#Back2Basics

April 15, 2025 at 8:21 PM
1/ 🔹Immune checkpoints like CTLA-4, PD-1,PD-L1 AND LAG-3 suppress T-cell activity -> cancer cells evade immune anti-tumor response
🔹IC inhibitors (ICI)➡️ Reactivation T-cell response to CA
➡️ improved survival across many cancers
#Back2Basics
🔹IC inhibitors (ICI)➡️ Reactivation T-cell response to CA
➡️ improved survival across many cancers
#Back2Basics

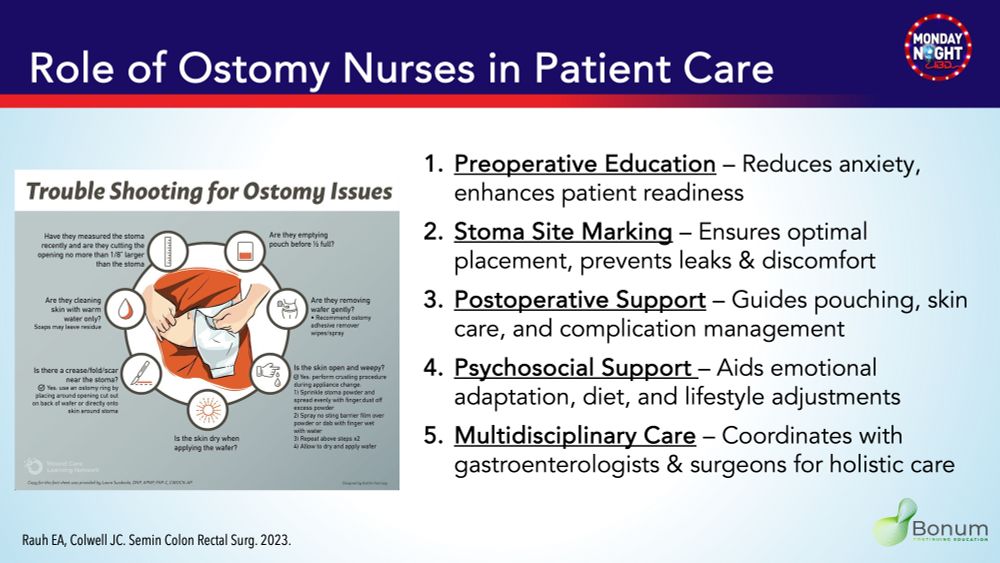
11/💡 Ostomy #nurses improve QoL & outcomes!
🔹 Reduce anxiety & aid adaptation
🔹 Ensure optimal stoma placement
🔹 Guide pouching & skin care
🔹 Support emotional & lifestyle needs
🔹 Collaborate with GI & surgery teams
👏 Their role is vital! #OstomyCare #IBD #Nursing
🔹 Reduce anxiety & aid adaptation
🔹 Ensure optimal stoma placement
🔹 Guide pouching & skin care
🔹 Support emotional & lifestyle needs
🔹 Collaborate with GI & surgery teams
👏 Their role is vital! #OstomyCare #IBD #Nursing
February 28, 2025 at 1:11 AM
11/💡 Ostomy #nurses improve QoL & outcomes!
🔹 Reduce anxiety & aid adaptation
🔹 Ensure optimal stoma placement
🔹 Guide pouching & skin care
🔹 Support emotional & lifestyle needs
🔹 Collaborate with GI & surgery teams
👏 Their role is vital! #OstomyCare #IBD #Nursing
🔹 Reduce anxiety & aid adaptation
🔹 Ensure optimal stoma placement
🔹 Guide pouching & skin care
🔹 Support emotional & lifestyle needs
🔹 Collaborate with GI & surgery teams
👏 Their role is vital! #OstomyCare #IBD #Nursing
10/ Stomal Prolapse
🔹Rate : 5%- 10 %
🔹The elongation of the intestinal portion of the stoma.
🚨Acute prolapse → Incarceration and Ischemia→
☹️Pain, obstipation, and purple/ black discoloration of stoma. 🚨emergency surgery. #CRSurgery
🔹Rate : 5%- 10 %
🔹The elongation of the intestinal portion of the stoma.
🚨Acute prolapse → Incarceration and Ischemia→
☹️Pain, obstipation, and purple/ black discoloration of stoma. 🚨emergency surgery. #CRSurgery

February 28, 2025 at 1:11 AM
10/ Stomal Prolapse
🔹Rate : 5%- 10 %
🔹The elongation of the intestinal portion of the stoma.
🚨Acute prolapse → Incarceration and Ischemia→
☹️Pain, obstipation, and purple/ black discoloration of stoma. 🚨emergency surgery. #CRSurgery
🔹Rate : 5%- 10 %
🔹The elongation of the intestinal portion of the stoma.
🚨Acute prolapse → Incarceration and Ischemia→
☹️Pain, obstipation, and purple/ black discoloration of stoma. 🚨emergency surgery. #CRSurgery
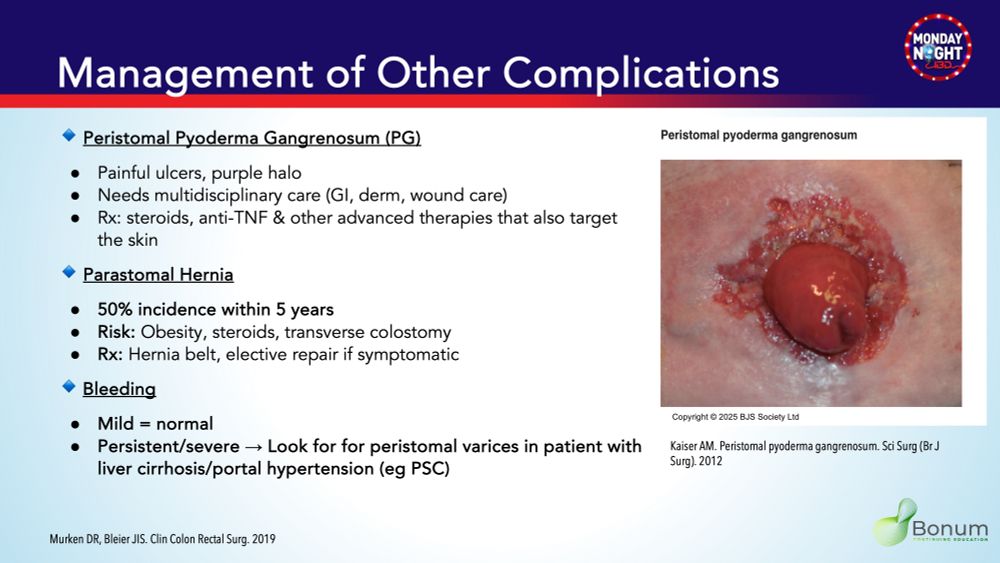
9/Other #ostomy complications
⭕️Pyoderma gangrenosum: painful ulcer around the stoma
⭕️Parastomal hernia: Common
⭕️Stoma bleeding : think peristomal varices in pts with liver dis/PSC
📸for more details👇
⭕️Pyoderma gangrenosum: painful ulcer around the stoma
⭕️Parastomal hernia: Common
⭕️Stoma bleeding : think peristomal varices in pts with liver dis/PSC
📸for more details👇
February 28, 2025 at 1:11 AM
9/Other #ostomy complications
⭕️Pyoderma gangrenosum: painful ulcer around the stoma
⭕️Parastomal hernia: Common
⭕️Stoma bleeding : think peristomal varices in pts with liver dis/PSC
📸for more details👇
⭕️Pyoderma gangrenosum: painful ulcer around the stoma
⭕️Parastomal hernia: Common
⭕️Stoma bleeding : think peristomal varices in pts with liver dis/PSC
📸for more details👇
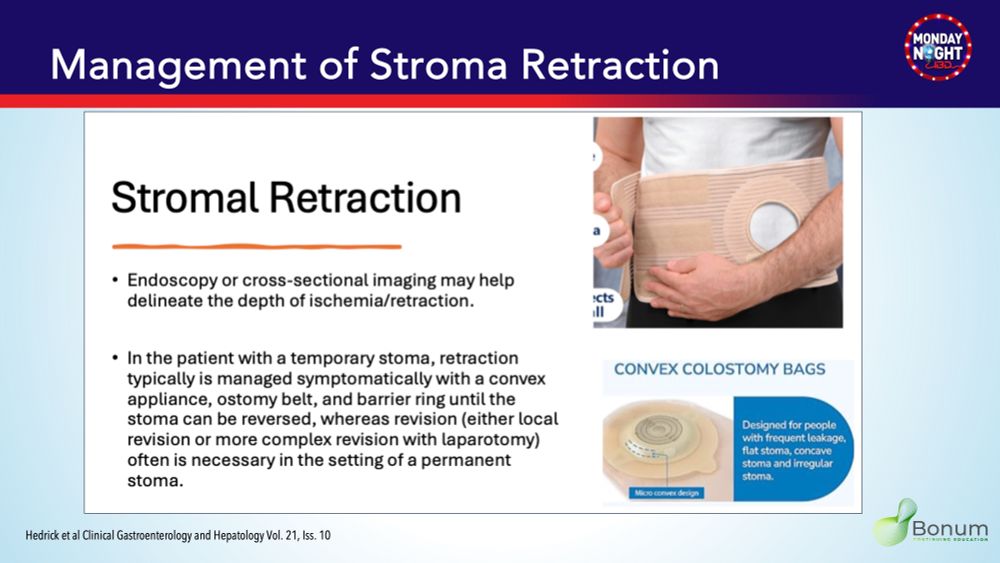
8/🔹 Stomal Retraction/Flat stoma
Cause: Ischemia, obesity
Assess depth of retraction by Endoscopy/imaging
Rx: Convex appliance, barrier ring, revision
#IBD #OstomyCare #GITwitter
Cause: Ischemia, obesity
Assess depth of retraction by Endoscopy/imaging
Rx: Convex appliance, barrier ring, revision
#IBD #OstomyCare #GITwitter
February 28, 2025 at 1:11 AM
8/🔹 Stomal Retraction/Flat stoma
Cause: Ischemia, obesity
Assess depth of retraction by Endoscopy/imaging
Rx: Convex appliance, barrier ring, revision
#IBD #OstomyCare #GITwitter
Cause: Ischemia, obesity
Assess depth of retraction by Endoscopy/imaging
Rx: Convex appliance, barrier ring, revision
#IBD #OstomyCare #GITwitter
7/🔹 Ostomy Leakage
Risk factors: Obesity, skin creases, flat stoma
Prevention: Proper Pre-op marking, surgical technique
Rx: Antidiarrheals, appliance change, more tips👇
#IBD #OstomyCare #CRSurgery
Risk factors: Obesity, skin creases, flat stoma
Prevention: Proper Pre-op marking, surgical technique
Rx: Antidiarrheals, appliance change, more tips👇
#IBD #OstomyCare #CRSurgery

February 28, 2025 at 1:11 AM
7/🔹 Ostomy Leakage
Risk factors: Obesity, skin creases, flat stoma
Prevention: Proper Pre-op marking, surgical technique
Rx: Antidiarrheals, appliance change, more tips👇
#IBD #OstomyCare #CRSurgery
Risk factors: Obesity, skin creases, flat stoma
Prevention: Proper Pre-op marking, surgical technique
Rx: Antidiarrheals, appliance change, more tips👇
#IBD #OstomyCare #CRSurgery
6/ 🚨 High Ostomy Output (HOO)>1.5L/day
🔹 Early ≤3 wks post-ileostomy
🔹 Chronic >3 wks post-op, in jejunal ostomy, short bowel syndrome
📌 Rx: Rule out infection, bulking, antimotility, antisecretory agents, IVF, ostomy reversal.
🔹 Early ≤3 wks post-ileostomy
🔹 Chronic >3 wks post-op, in jejunal ostomy, short bowel syndrome
📌 Rx: Rule out infection, bulking, antimotility, antisecretory agents, IVF, ostomy reversal.

February 28, 2025 at 1:11 AM
6/ 🚨 High Ostomy Output (HOO)>1.5L/day
🔹 Early ≤3 wks post-ileostomy
🔹 Chronic >3 wks post-op, in jejunal ostomy, short bowel syndrome
📌 Rx: Rule out infection, bulking, antimotility, antisecretory agents, IVF, ostomy reversal.
🔹 Early ≤3 wks post-ileostomy
🔹 Chronic >3 wks post-op, in jejunal ostomy, short bowel syndrome
📌 Rx: Rule out infection, bulking, antimotility, antisecretory agents, IVF, ostomy reversal.
5/Complications of Ostomy
🎯Short Term
🔥Early High ostomy output
🔥Ostomy Leakage
🔥Mucocutaneous separation
🔥Stromal Retraction
🎯Long Term
🔥Dermatological Problems
🔥Chronic High ostomy output
🔥Parastomal Hernia
🔥Stromal Prolapse
🔥Bleeding
🎯Short Term
🔥Early High ostomy output
🔥Ostomy Leakage
🔥Mucocutaneous separation
🔥Stromal Retraction
🎯Long Term
🔥Dermatological Problems
🔥Chronic High ostomy output
🔥Parastomal Hernia
🔥Stromal Prolapse
🔥Bleeding

February 28, 2025 at 1:11 AM
5/Complications of Ostomy
🎯Short Term
🔥Early High ostomy output
🔥Ostomy Leakage
🔥Mucocutaneous separation
🔥Stromal Retraction
🎯Long Term
🔥Dermatological Problems
🔥Chronic High ostomy output
🔥Parastomal Hernia
🔥Stromal Prolapse
🔥Bleeding
🎯Short Term
🔥Early High ostomy output
🔥Ostomy Leakage
🔥Mucocutaneous separation
🔥Stromal Retraction
🎯Long Term
🔥Dermatological Problems
🔥Chronic High ostomy output
🔥Parastomal Hernia
🔥Stromal Prolapse
🔥Bleeding
4/ Ileostomy is often a step to #IPAA #CRSurgery
2⃣Stage✂️: Total colectomy +IPAA & DLI➡️DLI closure
✅If Stable healthy pt (eg ✂️for dysplasia)
3⃣Stage✂️:colectomy+EI➡️proctectomy +IPAA+DLI➡️DLI closure
✅If active dis, malnourished, steroids & IS (eg ASUC)
📸More details👇
2⃣Stage✂️: Total colectomy +IPAA & DLI➡️DLI closure
✅If Stable healthy pt (eg ✂️for dysplasia)
3⃣Stage✂️:colectomy+EI➡️proctectomy +IPAA+DLI➡️DLI closure
✅If active dis, malnourished, steroids & IS (eg ASUC)
📸More details👇


February 28, 2025 at 1:11 AM
4/ Ileostomy is often a step to #IPAA #CRSurgery
2⃣Stage✂️: Total colectomy +IPAA & DLI➡️DLI closure
✅If Stable healthy pt (eg ✂️for dysplasia)
3⃣Stage✂️:colectomy+EI➡️proctectomy +IPAA+DLI➡️DLI closure
✅If active dis, malnourished, steroids & IS (eg ASUC)
📸More details👇
2⃣Stage✂️: Total colectomy +IPAA & DLI➡️DLI closure
✅If Stable healthy pt (eg ✂️for dysplasia)
3⃣Stage✂️:colectomy+EI➡️proctectomy +IPAA+DLI➡️DLI closure
✅If active dis, malnourished, steroids & IS (eg ASUC)
📸More details👇
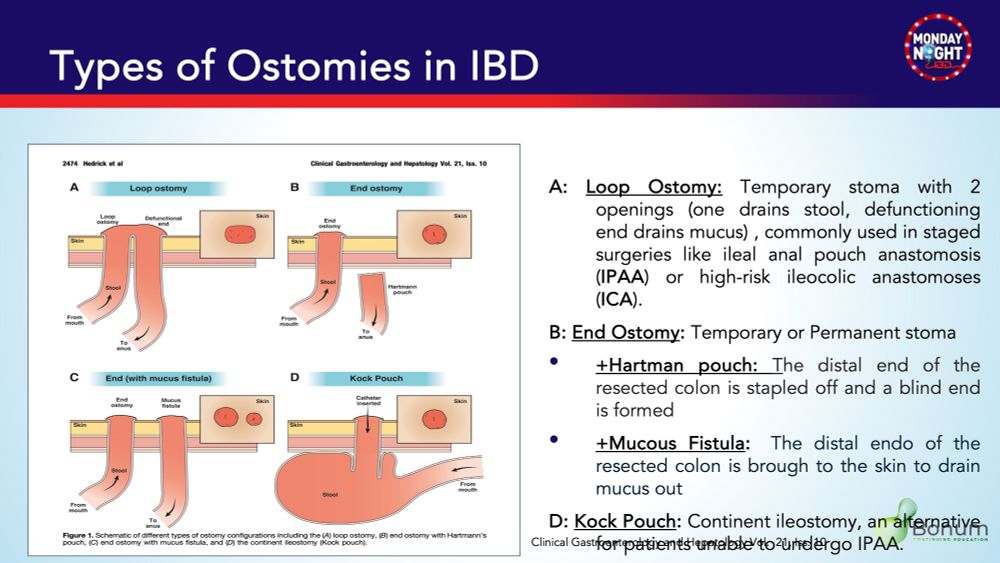
3/ #Ostomies aren’t one-size-fits-all!
⏳ Temporary vs. Permanent
🌀 Loop vs. End (two vs. single opening)
🔚End-ostomy w Hartman pouch vs mucous fistula
💧 Continent pouch vs. Non-Continent (external appliance)
💡 Know the indications & differences & what to expect on endoscopy
⏳ Temporary vs. Permanent
🌀 Loop vs. End (two vs. single opening)
🔚End-ostomy w Hartman pouch vs mucous fistula
💧 Continent pouch vs. Non-Continent (external appliance)
💡 Know the indications & differences & what to expect on endoscopy
February 28, 2025 at 1:11 AM
3/ #Ostomies aren’t one-size-fits-all!
⏳ Temporary vs. Permanent
🌀 Loop vs. End (two vs. single opening)
🔚End-ostomy w Hartman pouch vs mucous fistula
💧 Continent pouch vs. Non-Continent (external appliance)
💡 Know the indications & differences & what to expect on endoscopy
⏳ Temporary vs. Permanent
🌀 Loop vs. End (two vs. single opening)
🔚End-ostomy w Hartman pouch vs mucous fistula
💧 Continent pouch vs. Non-Continent (external appliance)
💡 Know the indications & differences & what to expect on endoscopy

