


@michael-robersmd.bsky.social
neuroimmunology/ multiple sclerosis specialist at Barrow Neurological Institute. Neuroscience educator at Creighton-PHX. Health equity and clinical researcher. Views are my own and do not represent individual medical advice or the views of my employers.
Day 3 of #ECTRIMS2025
extension results for ravulizumab in NMO disease (AQP4+). 0 relapses in 105 patient years! absolutely incredible efficacy!
extension results for ravulizumab in NMO disease (AQP4+). 0 relapses in 105 patient years! absolutely incredible efficacy!

September 26, 2025 at 7:22 AM
Day 3 of #ECTRIMS2025
extension results for ravulizumab in NMO disease (AQP4+). 0 relapses in 105 patient years! absolutely incredible efficacy!
extension results for ravulizumab in NMO disease (AQP4+). 0 relapses in 105 patient years! absolutely incredible efficacy!
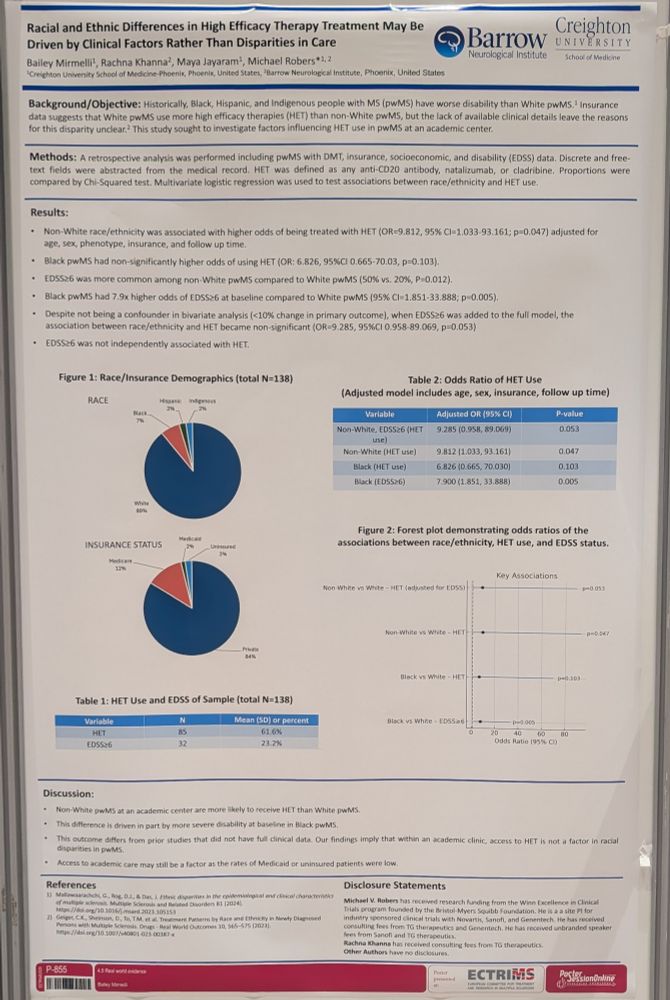
Our abstract on High Efficacy Therapy Use by race/ethnicity. We found that while non-White individuals had higher rates of HET use, the association disappeared when adjusted for disability implying that clinical factors drive prescription patterns. # ECTRIMS2025

September 25, 2025 at 6:12 PM
Our abstract on High Efficacy Therapy Use by race/ethnicity. We found that while non-White individuals had higher rates of HET use, the association disappeared when adjusted for disability implying that clinical factors drive prescription patterns. # ECTRIMS2025
eposter up and available at #ECTRIMS2025. HTN awareness is lower in Hispanic people with MS than the general population and lower than a recent predominantly White MS cohort. younger age is associated with worse awareness, but integrated healthcare is associated with better awareness.

September 24, 2025 at 5:18 PM
eposter up and available at #ECTRIMS2025. HTN awareness is lower in Hispanic people with MS than the general population and lower than a recent predominantly White MS cohort. younger age is associated with worse awareness, but integrated healthcare is associated with better awareness.
P113 American Heart Association Blood Pressure Categories Have Stronger Associations with Worsening Disability than other Hypertension Metrics In Multiple Sclerosis.
- AHA stage II HTN may be a better tool than SBP or DBP alone for future MS HTN comorbidity research
Come visit!
- AHA stage II HTN may be a better tool than SBP or DBP alone for future MS HTN comorbidity research
Come visit!


September 24, 2025 at 2:33 PM
P113 American Heart Association Blood Pressure Categories Have Stronger Associations with Worsening Disability than other Hypertension Metrics In Multiple Sclerosis.
- AHA stage II HTN may be a better tool than SBP or DBP alone for future MS HTN comorbidity research
Come visit!
- AHA stage II HTN may be a better tool than SBP or DBP alone for future MS HTN comorbidity research
Come visit!
-cerebellar lesions now count as a typical presentation
-some additional new "typical" MRI findings
-confidence of diagnostic criteria now separated by quality of antibody test
-some additional new "typical" MRI findings
-confidence of diagnostic criteria now separated by quality of antibody test



September 24, 2025 at 1:27 PM
-cerebellar lesions now count as a typical presentation
-some additional new "typical" MRI findings
-confidence of diagnostic criteria now separated by quality of antibody test
-some additional new "typical" MRI findings
-confidence of diagnostic criteria now separated by quality of antibody test
comorbidities such as hypertension (HTN) are important in #multipleSclerosis care. A Gap in care exists where many people with MS are unaware they have HTN. I look forward to presenting our findings on HTN Unawareness today at #CMSC In the "Disease Management" session (north 122abc from 3-5pm).

May 29, 2025 at 4:49 PM
comorbidities such as hypertension (HTN) are important in #multipleSclerosis care. A Gap in care exists where many people with MS are unaware they have HTN. I look forward to presenting our findings on HTN Unawareness today at #CMSC In the "Disease Management" session (north 122abc from 3-5pm).

It's MS awareness month, and Barrow Neurological Institute will be hosting its 3rd annual MS Empowerment Summit on April 19th. This summit is for people living with MS as well as their family, friends, and support systems. This years topics will be "MS in the workplace" as well as fatigue management

March 5, 2025 at 8:27 PM
It's MS awareness month, and Barrow Neurological Institute will be hosting its 3rd annual MS Empowerment Summit on April 19th. This summit is for people living with MS as well as their family, friends, and support systems. This years topics will be "MS in the workplace" as well as fatigue management
Happy to wake up early to be a part of #WalkMS Tucson, supporting the NMSS and people affected by MS in Southern AZ. Barrow Neuroimmunology takes care of many people from across Arizona. Our first year at this event is one step we're taking to Broaden our community engagement beyond Phoenix.


March 1, 2025 at 11:18 PM
Happy to wake up early to be a part of #WalkMS Tucson, supporting the NMSS and people affected by MS in Southern AZ. Barrow Neuroimmunology takes care of many people from across Arizona. Our first year at this event is one step we're taking to Broaden our community engagement beyond Phoenix.

I'm attending The 10th anniversary #ACTRIMS. I attended as a part of the resident summit in the 2nd year. Now as faculty, I'm supporting the Barrow neuroimmunology fellow Rachna Khanna who is presenting and learning here. Happy to now to be a part of training the future of MS specialists.

February 27, 2025 at 3:58 PM
I'm attending The 10th anniversary #ACTRIMS. I attended as a part of the resident summit in the 2nd year. Now as faculty, I'm supporting the Barrow neuroimmunology fellow Rachna Khanna who is presenting and learning here. Happy to now to be a part of training the future of MS specialists.
Today I advocated with the Arizona chapter of the National MS Society for state legislation which will prevent Insurance from forcing medication changes without physician and patient consent during a plan year or while a patient is on a continuous insurance policy. Local policy matters in healthcare


January 28, 2025 at 9:00 PM
Today I advocated with the Arizona chapter of the National MS Society for state legislation which will prevent Insurance from forcing medication changes without physician and patient consent during a plan year or while a patient is on a continuous insurance policy. Local policy matters in healthcare
Those are my 4 questions to diagnose MS! A one slide workflow is below. Let me know what you think? Find a hole, or have a different idea please let me know! I'm trying to simplify what we heard and teach the new criteria without referencing the old ones.

January 28, 2025 at 12:29 AM
Those are my 4 questions to diagnose MS! A one slide workflow is below. Let me know what you think? Find a hole, or have a different idea please let me know! I'm trying to simplify what we heard and teach the new criteria without referencing the old ones.
How much specificity do you need? Depends on how many locations are in #2.
4-5 locations? No extra specificity needed
2-3 locations? 1 extra specificity sign needed
Only 1 location? Needs 2 extra specificity signs.
4-5 locations? No extra specificity needed
2-3 locations? 1 extra specificity sign needed
Only 1 location? Needs 2 extra specificity signs.

January 28, 2025 at 12:29 AM
How much specificity do you need? Depends on how many locations are in #2.
4-5 locations? No extra specificity needed
2-3 locations? 1 extra specificity sign needed
Only 1 location? Needs 2 extra specificity signs.
4-5 locations? No extra specificity needed
2-3 locations? 1 extra specificity sign needed
Only 1 location? Needs 2 extra specificity signs.
4) now check for specificity.
There are 3 ways to do this.
1) MRI findings (6 central veins or 1 paramagnetic rim lesion)
2) CSF testing (oligoclonal bands OR kappa free light chains)
3) dissemination in time (multiple attacks, new lesions on repeat MRIs, or enhancing and non enhancing lesions)
There are 3 ways to do this.
1) MRI findings (6 central veins or 1 paramagnetic rim lesion)
2) CSF testing (oligoclonal bands OR kappa free light chains)
3) dissemination in time (multiple attacks, new lesions on repeat MRIs, or enhancing and non enhancing lesions)

January 28, 2025 at 12:29 AM
4) now check for specificity.
There are 3 ways to do this.
1) MRI findings (6 central veins or 1 paramagnetic rim lesion)
2) CSF testing (oligoclonal bands OR kappa free light chains)
3) dissemination in time (multiple attacks, new lesions on repeat MRIs, or enhancing and non enhancing lesions)
There are 3 ways to do this.
1) MRI findings (6 central veins or 1 paramagnetic rim lesion)
2) CSF testing (oligoclonal bands OR kappa free light chains)
3) dissemination in time (multiple attacks, new lesions on repeat MRIs, or enhancing and non enhancing lesions)
#3, Not every patient needs every test but make sure to do a thoughtful search for alternative diagnosed (see non exhaustive list in pic)

January 28, 2025 at 12:29 AM
#3, Not every patient needs every test but make sure to do a thoughtful search for alternative diagnosed (see non exhaustive list in pic)
when looking for MS lesions, remember they need to be typical of MS (>3mm, oval, discreet, in typical location). There are 5 locations to include. Optic nerve, touching the cortex, touching and perpendicular to the ventricles, infratentorial, or spinal cord.
Count how many locations are involved.
Count how many locations are involved.

January 28, 2025 at 12:29 AM
when looking for MS lesions, remember they need to be typical of MS (>3mm, oval, discreet, in typical location). There are 5 locations to include. Optic nerve, touching the cortex, touching and perpendicular to the ventricles, infratentorial, or spinal cord.
Count how many locations are involved.
Count how many locations are involved.
Each Question gets a little more detail.
3 ways to suspect MS.
1) clinical Demyelinating event/ CIS. (optic neuritis, myelitis, cerebral Demyelinating syndromes)
2) 1 year of progressive neurologic decline concerning for PPMS (usually myelopathy)
3) Radiologically Isolated Syndrome (see citation)
3 ways to suspect MS.
1) clinical Demyelinating event/ CIS. (optic neuritis, myelitis, cerebral Demyelinating syndromes)
2) 1 year of progressive neurologic decline concerning for PPMS (usually myelopathy)
3) Radiologically Isolated Syndrome (see citation)

January 28, 2025 at 12:29 AM
Each Question gets a little more detail.
3 ways to suspect MS.
1) clinical Demyelinating event/ CIS. (optic neuritis, myelitis, cerebral Demyelinating syndromes)
2) 1 year of progressive neurologic decline concerning for PPMS (usually myelopathy)
3) Radiologically Isolated Syndrome (see citation)
3 ways to suspect MS.
1) clinical Demyelinating event/ CIS. (optic neuritis, myelitis, cerebral Demyelinating syndromes)
2) 1 year of progressive neurologic decline concerning for PPMS (usually myelopathy)
3) Radiologically Isolated Syndrome (see citation)
4 questions can solve the 2024 dx criteria.
1) is there a reason to suspect MS?
2) is there at least one Demyelinating lesion on MRI
- If so how many locations?
3) Have MS mimics been excluded?
4) based on #2, does the patient have enough signs
specific for MS to dx?
4 Yeses= MS diagnosed!
1) is there a reason to suspect MS?
2) is there at least one Demyelinating lesion on MRI
- If so how many locations?
3) Have MS mimics been excluded?
4) based on #2, does the patient have enough signs
specific for MS to dx?
4 Yeses= MS diagnosed!

January 28, 2025 at 12:29 AM
4 questions can solve the 2024 dx criteria.
1) is there a reason to suspect MS?
2) is there at least one Demyelinating lesion on MRI
- If so how many locations?
3) Have MS mimics been excluded?
4) based on #2, does the patient have enough signs
specific for MS to dx?
4 Yeses= MS diagnosed!
1) is there a reason to suspect MS?
2) is there at least one Demyelinating lesion on MRI
- If so how many locations?
3) Have MS mimics been excluded?
4) based on #2, does the patient have enough signs
specific for MS to dx?
4 Yeses= MS diagnosed!