



Mark Geyer, M.D.
@markgeyermd.bsky.social
Leukemia/cell therapy doc; Adolescent/Young Adult and ALL Leukemia Program Leader at Memorial Sloan Kettering Cancer Center. Indie rock and Boston sports fan. Opinions=my own. https://www.mskcc.org/cancer-care/doctors/mark-geyer. 💖💜💙
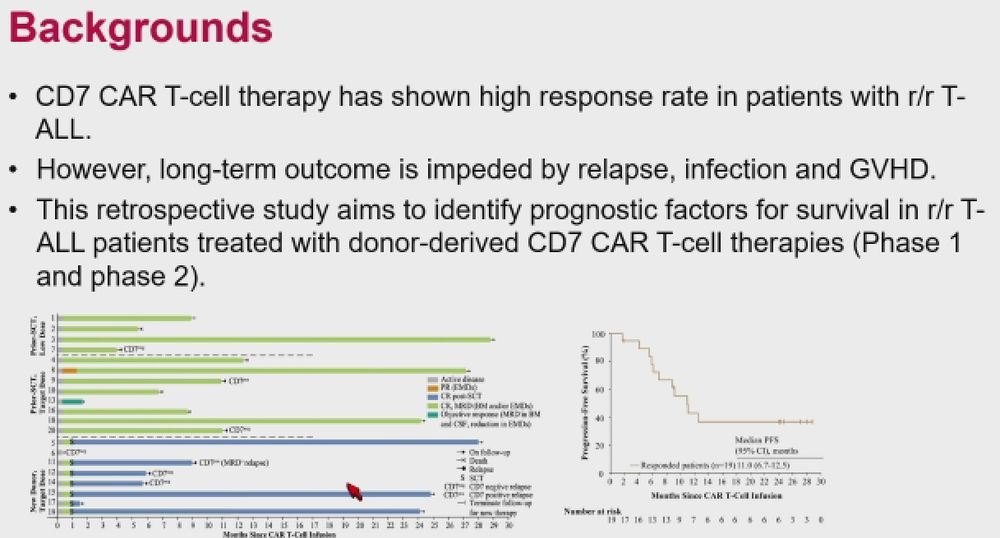
14 pts treated so far. Good expansion in PB/CSF. G1 CRS 64%, no G2+ CRS, no ICANS. Median f/u 244 days, 1 pt w/ molR at 6m post-CAR T-cells. No deaths or other relapses. Very short f/u (only 2 post-12 months). Interesting approach for short course tx in hard-to-treat group of pts. 2/2 #ash24 #allsm


December 10, 2024 at 1:55 AM
Dr. Ibrahim Aldoss from @cityofhope.bsky.social presents data on definitive CD19-targeted CAR T-cell therapy in pts ≥55 years w/ B-cell ALL in CR1. Lower disease burden pre-conditioning/LDC associated w/ ↓ toxicity and ↑ LFS. Pilot study schema as below. #ash24 #allsm 1/x


December 10, 2024 at 1:54 AM
Dr. Ibrahim Aldoss from @cityofhope.bsky.social presents data on definitive CD19-targeted CAR T-cell therapy in pts ≥55 years w/ B-cell ALL in CR1. Lower disease burden pre-conditioning/LDC associated w/ ↓ toxicity and ↑ LFS. Pilot study schema as below. #ash24 #allsm 1/x
82% of the CART2 products were cryopreserved leftover cells; details as below. 50% of relapsed pts achieved MRD- CR w/ CART2. ↓ disease burden associated w/ better LFS/OS w/ CART2. Time from CART1 to CART2 not associated w/ outcome. May be effective bridge to alloHCT or further tx. 2/2 #ASH24 #allsm




December 10, 2024 at 1:38 AM
82% of the CART2 products were cryopreserved leftover cells; details as below. 50% of relapsed pts achieved MRD- CR w/ CART2. ↓ disease burden associated w/ better LFS/OS w/ CART2. Time from CART1 to CART2 not associated w/ outcome. May be effective bridge to alloHCT or further tx. 2/2 #ASH24 #allsm







Dr. Jing Pan from Beijing Gobroad Hospital presents update on outcomes post-donor derived CD7 CAR T-cell therapy for pts w/ R/R T-ALL/LBL. Risks of relapse and death from infection significant in prior studies; authors aimed to clarify predictors of survival in 75 pts. 1/x #ash24 #allsm


December 10, 2024 at 1:22 AM



Dr. Jabbour from @mdanderson.bsky.social presents on long-term outcomes following obecabtagene autoleucel (obe-cel, Aucatzyl) stratified by depth of response by clonoSEQ NGS (sensitivity 10^-6). 84% of responders achieved clonoSEQ negativity. 1/x #ash24 #allsm




December 10, 2024 at 1:09 AM
Dr. Jabbour from @mdanderson.bsky.social presents on long-term outcomes following obecabtagene autoleucel (obe-cel, Aucatzyl) stratified by depth of response by clonoSEQ NGS (sensitivity 10^-6). 84% of responders achieved clonoSEQ negativity. 1/x #ash24 #allsm






OS/RD similar across transplant and non-transplant groups. No CNS relapses. HR T-ALL pts had ↑OS w/o alloHCT vs B-ALL pts w/ non-sig ↑trend w/ alloHCT; small #s of pts. Poor outcomes in those w/ mol relapse. Addition of blina in B-ALL may improve outcomes w/o HCT as well. 3/x #ASH24 #allsm




December 10, 2024 at 12:45 AM



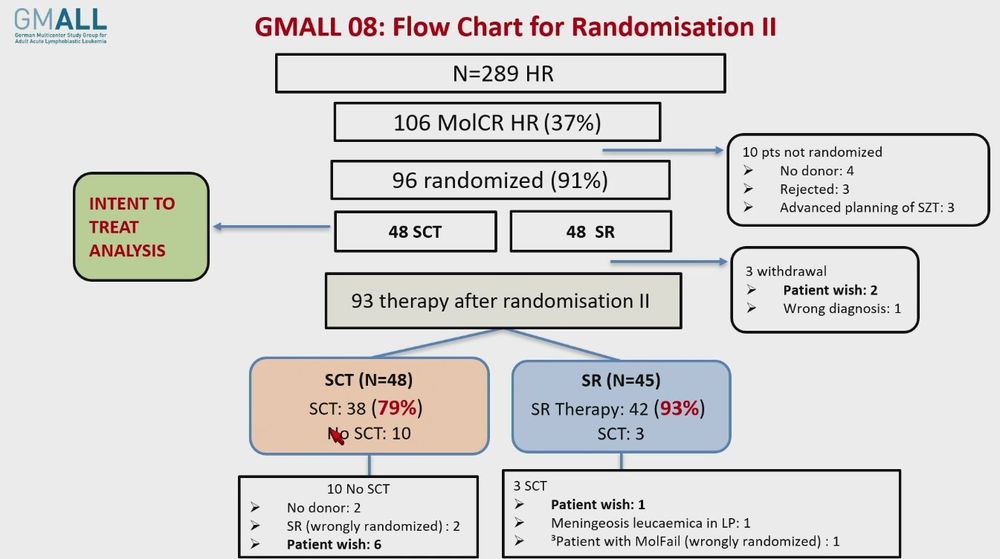
Dr. Nicola Goekbuget from Goethe University, University Hospital, Frankfurt reports on results of GMALL 08/2013 (age 18-55); this included randomization for Ph-neg HR ALL pts w/ available donor and molecular CR (<0.01% by qPCR) after induction phase 2 (IP2). 1/x #ash24 #allsm


December 10, 2024 at 12:42 AM
Very high rates of alloHCT realization; study recommending adjusting dose of TBI in conditioning regimen based on age. 5-year OS 72%. Encouraging results despite use of imatinib vs 2G/3G TKI; MRD at time of alloHCT not predictive. Risk of relapse in IKZF1+ pts remains a concern. 2/2 #ash24
#allsm
#allsm


December 10, 2024 at 12:08 AM





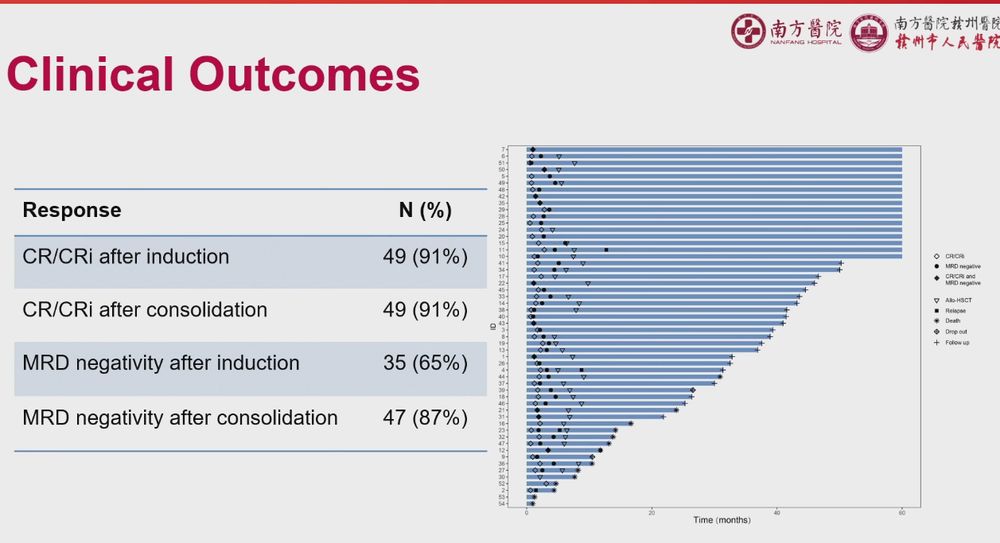
Single-arm phase 2 trial conducted; 54 pts treated; 49/54 CR/CRi post-induction. All pts considered for alloHCT during consolidation. 35 underwent alloHCT. 2/x




December 9, 2024 at 11:55 PM
Single-arm phase 2 trial conducted; 54 pts treated; 49/54 CR/CRi post-induction. All pts considered for alloHCT during consolidation. 35 underwent alloHCT. 2/x
Jieping Lin from Southern Medical University, Guangzhou, China presents on the HDAC inhibitor (HDACi) tucidinostat + pediatric-inspired chemo in pts age 14-55 w/ ETP-ALL/LBL. Role of HDACi hypothesized based on recurrent mutations in histone-modifying genes. 1/x #allsm #ash24


December 9, 2024 at 11:54 PM
Assessed circulating immune cells in 110 PON/BLIN recipients (compared w/ 43 DAS/BLIN). ↑NK, T-NK and Treg immunomod w/ DAS/BLIN (vs PON/BLIN). ↑T-cells, NK, NK-T, ↓Tregs w/ DAS/BLIN. NK-T cells in DAS/BLIN pts showed ↑CD25/CD69 (activation) and ↓exhaustion markers (PD1+TIM3+). 2/2 #allsm #ash24




December 9, 2024 at 11:42 PM
Dr. Michela Ansuinelli from Sapienza University of Rome reports on immunomodulatory effect of DAS + BLIN vs PON + BLIN in ND BCR::ABL+ ALL. Previous reports: DAS + BLIN ↑ NK, T-NK and CD8+ T cells, and a ↓of (Tregs), more evident after repeated cycles of BLIN. 1/x #allsm #ash24



December 9, 2024 at 11:40 PM
Higher WBC at dx, CNS dz at dx, VPREB1 deletion associated w/ higher risk of relapse. Neither p190 vs p210 nor IKZF1+ phenotype predicted relapse. 3-year OS 88%. How to intensify therapy for HR BCR::ABL+ ALL and how/if to transition off TKI safely unclear. 2/2 #ash24 #allsm


December 9, 2024 at 11:29 PM
Dr. Short from @mdanderson.bsky.social presents an update on their ponatinib/blinatumomab (pon/blin) experience. Regimen updated to include 15 LPs (rather than 12) to protect against CNS relapse. Pts w/ persistent BCR::ABL were clonoSEQ neg, suggesting BCR::ABL wasn't MRD. 1/x #ash24 #allsm




December 9, 2024 at 11:28 PM
Dr. Short from @mdanderson.bsky.social presents an update on their ponatinib/blinatumomab (pon/blin) experience. Regimen updated to include 15 LPs (rather than 12) to protect against CNS relapse. Pts w/ persistent BCR::ABL were clonoSEQ neg, suggesting BCR::ABL wasn't MRD. 1/x #ash24 #allsm
Dr. Shanshan Suo presents on venetoclax + HAG (homoharringtonine [aka HHT or omacetaxine] + ARA-C + G-CSF) for pts w/ ETP-ALL. Authors believe HHT synergizes w/ ven in ETP-ALL in vivo and in vitro. 31 txed pts received V-HAG (ven d1-14, longer if blasts ≥5% d14, HHT d1-10, LDAC d1-14, G-CSF d1-14).




December 9, 2024 at 11:12 PM
Dr. Shanshan Suo presents on venetoclax + HAG (homoharringtonine [aka HHT or omacetaxine] + ARA-C + G-CSF) for pts w/ ETP-ALL. Authors believe HHT synergizes w/ ven in ETP-ALL in vivo and in vitro. 31 txed pts received V-HAG (ven d1-14, longer if blasts ≥5% d14, HHT d1-10, LDAC d1-14, G-CSF d1-14).


