




مالك المطرودي
@malekpsych.bsky.social
طبيب نفسي مقيم في السنة الثانية
مهتم بالفلسفة و بفلسفة العلم بشكل خاص.
مهتم بالفلسفة و بفلسفة العلم بشكل خاص.
Last but not least
📌Manual based therapies (Interpersonal Social Rhythm therapy, CBT, Mindfulness)
📌Manual based therapies (Interpersonal Social Rhythm therapy, CBT, Mindfulness)


January 21, 2025 at 10:14 AM
Last but not least
📌Manual based therapies (Interpersonal Social Rhythm therapy, CBT, Mindfulness)
📌Manual based therapies (Interpersonal Social Rhythm therapy, CBT, Mindfulness)
📌 Lithium monotherapy (Evidenced for superiority in prevention of Manic episodes)
📌Lamotrigine (evidence strongest for prevention of Depressive episodes)
📌 if stable on Divalproex, then, maintain.
*A very interesting note: “be aware that there are limited data on longterm efficacy of Divalproex.”
📌Lamotrigine (evidence strongest for prevention of Depressive episodes)
📌 if stable on Divalproex, then, maintain.
*A very interesting note: “be aware that there are limited data on longterm efficacy of Divalproex.”
January 21, 2025 at 10:14 AM
📌 Lithium monotherapy (Evidenced for superiority in prevention of Manic episodes)
📌Lamotrigine (evidence strongest for prevention of Depressive episodes)
📌 if stable on Divalproex, then, maintain.
*A very interesting note: “be aware that there are limited data on longterm efficacy of Divalproex.”
📌Lamotrigine (evidence strongest for prevention of Depressive episodes)
📌 if stable on Divalproex, then, maintain.
*A very interesting note: “be aware that there are limited data on longterm efficacy of Divalproex.”
💊 Maintenance/Continuation treatment of Bipolar Disorder (Algorithm)
📌 due to the many choices in maintenance phase of BD Continue with the effective regimen used in acute mania. (However, be vigilant for adverse effects and patient needs and adjust accordingly)
📌 due to the many choices in maintenance phase of BD Continue with the effective regimen used in acute mania. (However, be vigilant for adverse effects and patient needs and adjust accordingly)
January 21, 2025 at 10:12 AM
💊 Maintenance/Continuation treatment of Bipolar Disorder (Algorithm)
📌 due to the many choices in maintenance phase of BD Continue with the effective regimen used in acute mania. (However, be vigilant for adverse effects and patient needs and adjust accordingly)
📌 due to the many choices in maintenance phase of BD Continue with the effective regimen used in acute mania. (However, be vigilant for adverse effects and patient needs and adjust accordingly)
📌 Severe episode (requiring hospitalization)
- Lithium or Divalproex + Aripiprazole, Asenapine, Quetiapine or Risperidone.
📌 If none of the above works
Consider Haloperidol or Olanzapine.
📌 If still no benefit move to Level 2 then Level 3 then Level 4 as indicated by the algorithm.
- Lithium or Divalproex + Aripiprazole, Asenapine, Quetiapine or Risperidone.
📌 If none of the above works
Consider Haloperidol or Olanzapine.
📌 If still no benefit move to Level 2 then Level 3 then Level 4 as indicated by the algorithm.


January 21, 2025 at 10:12 AM
📌 Severe episode (requiring hospitalization)
- Lithium or Divalproex + Aripiprazole, Asenapine, Quetiapine or Risperidone.
📌 If none of the above works
Consider Haloperidol or Olanzapine.
📌 If still no benefit move to Level 2 then Level 3 then Level 4 as indicated by the algorithm.
- Lithium or Divalproex + Aripiprazole, Asenapine, Quetiapine or Risperidone.
📌 If none of the above works
Consider Haloperidol or Olanzapine.
📌 If still no benefit move to Level 2 then Level 3 then Level 4 as indicated by the algorithm.
😆Acute Bipolar Mania (Algorithm)
📌 If Mild to moderate severity (not requiring hospitalization)
- Lithium (The GOAT) still holds sway as first line agent.
- Aripiprazole, Asenapine, Divalproex, Risperidone, Ziprasidone, or Cariprazine. (Also good choices as Monotherapy)
📌 If Mild to moderate severity (not requiring hospitalization)
- Lithium (The GOAT) still holds sway as first line agent.
- Aripiprazole, Asenapine, Divalproex, Risperidone, Ziprasidone, or Cariprazine. (Also good choices as Monotherapy)
January 21, 2025 at 10:11 AM
😆Acute Bipolar Mania (Algorithm)
📌 If Mild to moderate severity (not requiring hospitalization)
- Lithium (The GOAT) still holds sway as first line agent.
- Aripiprazole, Asenapine, Divalproex, Risperidone, Ziprasidone, or Cariprazine. (Also good choices as Monotherapy)
📌 If Mild to moderate severity (not requiring hospitalization)
- Lithium (The GOAT) still holds sway as first line agent.
- Aripiprazole, Asenapine, Divalproex, Risperidone, Ziprasidone, or Cariprazine. (Also good choices as Monotherapy)
📌 In both BD-I and BD-II, if the patient was already started on a mood stabilizer previously then consider augmenting with Lirasidone or Lamotrigine.
(Cariprazine doesn’t have enough evidence with it comes down to augmentation with mood stabilizer)
(Cariprazine doesn’t have enough evidence with it comes down to augmentation with mood stabilizer)


January 21, 2025 at 10:11 AM
📌 In both BD-I and BD-II, if the patient was already started on a mood stabilizer previously then consider augmenting with Lirasidone or Lamotrigine.
(Cariprazine doesn’t have enough evidence with it comes down to augmentation with mood stabilizer)
(Cariprazine doesn’t have enough evidence with it comes down to augmentation with mood stabilizer)
📌 Bipolar Type II — Quetiapine still holds sway as first line here.
📌 In both BD-I and BD-II, if the patient was already started on a mood stabilizer previously then consider augmenting with Lirasidone or Lamotrigine.
📌 Bipolar Type II — Quetiapine still holds sway as first line here.
📌 In both BD-I and BD-II, if the patient was already started on a mood stabilizer previously then consider augmenting with Lirasidone or Lamotrigine.
📌 Bipolar Type II — Quetiapine still holds sway as first line here.
January 21, 2025 at 10:10 AM
📌 Bipolar Type II — Quetiapine still holds sway as first line here.
📌 In both BD-I and BD-II, if the patient was already started on a mood stabilizer previously then consider augmenting with Lirasidone or Lamotrigine.
📌 Bipolar Type II — Quetiapine still holds sway as first line here.
📌 In both BD-I and BD-II, if the patient was already started on a mood stabilizer previously then consider augmenting with Lirasidone or Lamotrigine.
📌 Bipolar Type II — Quetiapine still holds sway as first line here.
☹️ Acute Bipolar Depression (Algorithm)
📌 Bipolar Type I — Lurasidone and Cariprazine as first line (due to their favorable metabolic profile)
🔴 A change from their 2017 guidelines where Quetiapine or Lurasidone were their first line agents.
📌 Bipolar Type I — Lurasidone and Cariprazine as first line (due to their favorable metabolic profile)
🔴 A change from their 2017 guidelines where Quetiapine or Lurasidone were their first line agents.
January 21, 2025 at 10:09 AM
☹️ Acute Bipolar Depression (Algorithm)
📌 Bipolar Type I — Lurasidone and Cariprazine as first line (due to their favorable metabolic profile)
🔴 A change from their 2017 guidelines where Quetiapine or Lurasidone were their first line agents.
📌 Bipolar Type I — Lurasidone and Cariprazine as first line (due to their favorable metabolic profile)
🔴 A change from their 2017 guidelines where Quetiapine or Lurasidone were their first line agents.
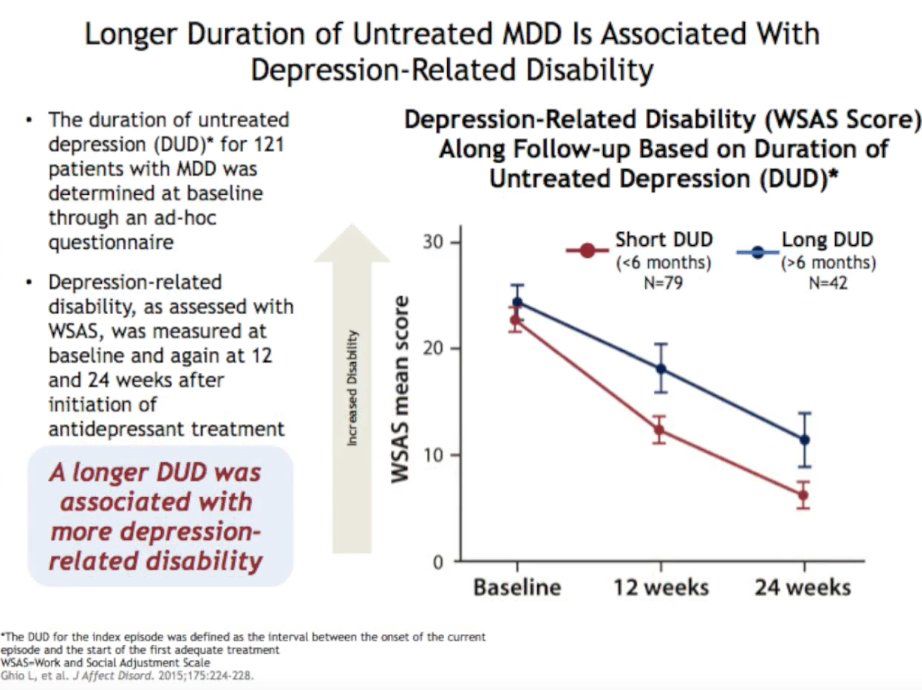
📌 DUE (Duration of untreated Episode)
is strongly associated with increasein depression-related disability
The earlier you intervene the better the outcome (much like in Early Psychosis prevention programs)
is strongly associated with increasein depression-related disability
The earlier you intervene the better the outcome (much like in Early Psychosis prevention programs)
January 21, 2025 at 10:08 AM
📌 DUE (Duration of untreated Episode)
is strongly associated with increasein depression-related disability
The earlier you intervene the better the outcome (much like in Early Psychosis prevention programs)
is strongly associated with increasein depression-related disability
The earlier you intervene the better the outcome (much like in Early Psychosis prevention programs)
(take history again as treatment resistance sometimes point to a faulty diagnosis)
January 21, 2025 at 10:07 AM
(take history again as treatment resistance sometimes point to a faulty diagnosis)
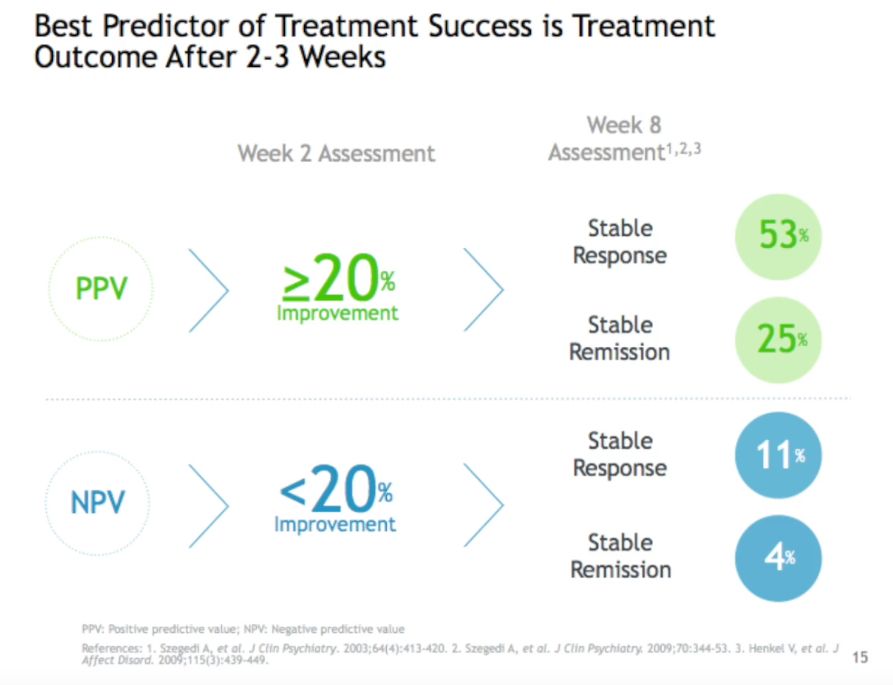
📌 Treatment success prediction:
best available evidence points to a period of around 2-4 weeks (3 on average).
be vigilant in non-responders as the longer they remain on current medication the less likelihood that they will respond to other agents.
best available evidence points to a period of around 2-4 weeks (3 on average).
be vigilant in non-responders as the longer they remain on current medication the less likelihood that they will respond to other agents.
January 21, 2025 at 10:07 AM
📌 Treatment success prediction:
best available evidence points to a period of around 2-4 weeks (3 on average).
be vigilant in non-responders as the longer they remain on current medication the less likelihood that they will respond to other agents.
best available evidence points to a period of around 2-4 weeks (3 on average).
be vigilant in non-responders as the longer they remain on current medication the less likelihood that they will respond to other agents.
STAR-D trial outcome- see second picture)


January 21, 2025 at 10:05 AM
STAR-D trial outcome- see second picture)
📌first off, some bullet points
1) Duration of Episode is strongly correlated with treatment response.
2) Treatment selection is the most important step in the management of any psychiatric patient, as this will determine the future tolerance and response to other mediactions (as evidenced by…
1) Duration of Episode is strongly correlated with treatment response.
2) Treatment selection is the most important step in the management of any psychiatric patient, as this will determine the future tolerance and response to other mediactions (as evidenced by…
January 21, 2025 at 10:05 AM
📌first off, some bullet points
1) Duration of Episode is strongly correlated with treatment response.
2) Treatment selection is the most important step in the management of any psychiatric patient, as this will determine the future tolerance and response to other mediactions (as evidenced by…
1) Duration of Episode is strongly correlated with treatment response.
2) Treatment selection is the most important step in the management of any psychiatric patient, as this will determine the future tolerance and response to other mediactions (as evidenced by…
🧠Management Of Mood Disorders (Based on the 2017 Florida Medicaid guideline as expounded on by Prof @rogersmcintyre)
I have updated the changes within above mentioned guidelines with their 2019-2020 update.
I have updated the changes within above mentioned guidelines with their 2019-2020 update.

January 21, 2025 at 10:04 AM
🧠Management Of Mood Disorders (Based on the 2017 Florida Medicaid guideline as expounded on by Prof @rogersmcintyre)
I have updated the changes within above mentioned guidelines with their 2019-2020 update.
I have updated the changes within above mentioned guidelines with their 2019-2020 update.
and dishonest – but the myth – persistent, persuasive and unrealistic. Too often we hold fast to the cliches of our forebears. We subject all facts to a prefabricated set of interpretations. We enjoy the comfort of opinion without the discomfort of thought.
(Commencement address at Yale Uni,1962)
(Commencement address at Yale Uni,1962)
January 21, 2025 at 10:03 AM
and dishonest – but the myth – persistent, persuasive and unrealistic. Too often we hold fast to the cliches of our forebears. We subject all facts to a prefabricated set of interpretations. We enjoy the comfort of opinion without the discomfort of thought.
(Commencement address at Yale Uni,1962)
(Commencement address at Yale Uni,1962)
👴🏼 Professor Gin Malhi Stance
“Professor Malhi’s 2021 editorial on lithium mythology opens with a quote from former US President John F. Kennedy that aptly describes why certain ideas take root and are difficult to eradicate:
The great enemy of truth is very often not the lie - deliberate, contrived
“Professor Malhi’s 2021 editorial on lithium mythology opens with a quote from former US President John F. Kennedy that aptly describes why certain ideas take root and are difficult to eradicate:
The great enemy of truth is very often not the lie - deliberate, contrived
January 21, 2025 at 10:02 AM
👴🏼 Professor Gin Malhi Stance
“Professor Malhi’s 2021 editorial on lithium mythology opens with a quote from former US President John F. Kennedy that aptly describes why certain ideas take root and are difficult to eradicate:
The great enemy of truth is very often not the lie - deliberate, contrived
“Professor Malhi’s 2021 editorial on lithium mythology opens with a quote from former US President John F. Kennedy that aptly describes why certain ideas take root and are difficult to eradicate:
The great enemy of truth is very often not the lie - deliberate, contrived


episodes.
As of 2022, leading BD experts comment about lithium: “It is equally efficacious in rapid and non-rapid cycling patients”
#Lithium #Psychopharmacology #Psychiatry
As of 2022, leading BD experts comment about lithium: “It is equally efficacious in rapid and non-rapid cycling patients”
#Lithium #Psychopharmacology #Psychiatry
January 21, 2025 at 10:00 AM
episodes.
As of 2022, leading BD experts comment about lithium: “It is equally efficacious in rapid and non-rapid cycling patients”
#Lithium #Psychopharmacology #Psychiatry
As of 2022, leading BD experts comment about lithium: “It is equally efficacious in rapid and non-rapid cycling patients”
#Lithium #Psychopharmacology #Psychiatry
examine this issue.
The current impression that lithium is not inferior to other mood stabilizers for RC-BD maintenance therapy is based on almost 50 years of research that characterized RC-BD as a difficult group to treat with any mood stabilizer monotherapy due to the frequency of depressive…
The current impression that lithium is not inferior to other mood stabilizers for RC-BD maintenance therapy is based on almost 50 years of research that characterized RC-BD as a difficult group to treat with any mood stabilizer monotherapy due to the frequency of depressive…
January 21, 2025 at 9:59 AM
examine this issue.
The current impression that lithium is not inferior to other mood stabilizers for RC-BD maintenance therapy is based on almost 50 years of research that characterized RC-BD as a difficult group to treat with any mood stabilizer monotherapy due to the frequency of depressive…
The current impression that lithium is not inferior to other mood stabilizers for RC-BD maintenance therapy is based on almost 50 years of research that characterized RC-BD as a difficult group to treat with any mood stabilizer monotherapy due to the frequency of depressive…
👁️ Excerpt from Stahl’s The Lithium Handbook:
As noted in the 2022 meta-analysis of adult lithium BD trials, “the widely believed concept among clinicians that divalproex is more effective than lithium in the long-term management of rapid-cycling BD was not supported” by the only clinical trial to
As noted in the 2022 meta-analysis of adult lithium BD trials, “the widely believed concept among clinicians that divalproex is more effective than lithium in the long-term management of rapid-cycling BD was not supported” by the only clinical trial to
January 21, 2025 at 9:59 AM
👁️ Excerpt from Stahl’s The Lithium Handbook:
As noted in the 2022 meta-analysis of adult lithium BD trials, “the widely believed concept among clinicians that divalproex is more effective than lithium in the long-term management of rapid-cycling BD was not supported” by the only clinical trial to
As noted in the 2022 meta-analysis of adult lithium BD trials, “the widely believed concept among clinicians that divalproex is more effective than lithium in the long-term management of rapid-cycling BD was not supported” by the only clinical trial to
“The refined message from two decades
of research is that the limitations of lithium relate to the neurobiology of RC-BD itself and not a failure of lithium per se, and that no mood stabilizer monotherapy will be sufficient to manage mood recurrence in many of these individuals.”
*Stahl (LHB,2024)
of research is that the limitations of lithium relate to the neurobiology of RC-BD itself and not a failure of lithium per se, and that no mood stabilizer monotherapy will be sufficient to manage mood recurrence in many of these individuals.”
*Stahl (LHB,2024)
January 21, 2025 at 9:56 AM
“The refined message from two decades
of research is that the limitations of lithium relate to the neurobiology of RC-BD itself and not a failure of lithium per se, and that no mood stabilizer monotherapy will be sufficient to manage mood recurrence in many of these individuals.”
*Stahl (LHB,2024)
of research is that the limitations of lithium relate to the neurobiology of RC-BD itself and not a failure of lithium per se, and that no mood stabilizer monotherapy will be sufficient to manage mood recurrence in many of these individuals.”
*Stahl (LHB,2024)
👁️👁️ However, when the analysis was confined to data from high-quality studies (11 trials out of 31 trials originally included)
Only Higher lifetime number of hospitalization admissions remained.
Only Higher lifetime number of hospitalization admissions remained.
January 21, 2025 at 9:55 AM
👁️👁️ However, when the analysis was confined to data from high-quality studies (11 trials out of 31 trials originally included)
Only Higher lifetime number of hospitalization admissions remained.
Only Higher lifetime number of hospitalization admissions remained.