



Lorenzo Pinelli
@lorpin.bsky.social
Adult and pediatric neuroradiologist, lifelong learner, still on (what remains of) Twitter too, probably not for much time #MedSky
Well, it depends on the case 🤷🏼♂️
April 14, 2025 at 12:00 AM
Well, it depends on the case 🤷🏼♂️
Reposted by Lorenzo Pinelli
"This systematic review and meta-analysis evaluated the association between the presence of a vascular loop within the IAM (IVL) or contacting the vestibulocochlear nerve (CN VIII NVC) and audiovestibular symptoms. There was no statistically significant correlation."
March 7, 2025 at 8:29 PM
"This systematic review and meta-analysis evaluated the association between the presence of a vascular loop within the IAM (IVL) or contacting the vestibulocochlear nerve (CN VIII NVC) and audiovestibular symptoms. There was no statistically significant correlation."
Indeed, more precise and easily understandable 👏🏼
December 29, 2024 at 12:32 AM
Indeed, more precise and easily understandable 👏🏼
Glad to see I’m not the only one asking these questions to residents who use this pre-packaged phrase in the body of the report. Often when there are no abnormalities at all (which for me generates a one word report: “Normal”). 🤷🏼♂️
December 29, 2024 at 12:31 AM
Glad to see I’m not the only one asking these questions to residents who use this pre-packaged phrase in the body of the report. Often when there are no abnormalities at all (which for me generates a one word report: “Normal”). 🤷🏼♂️
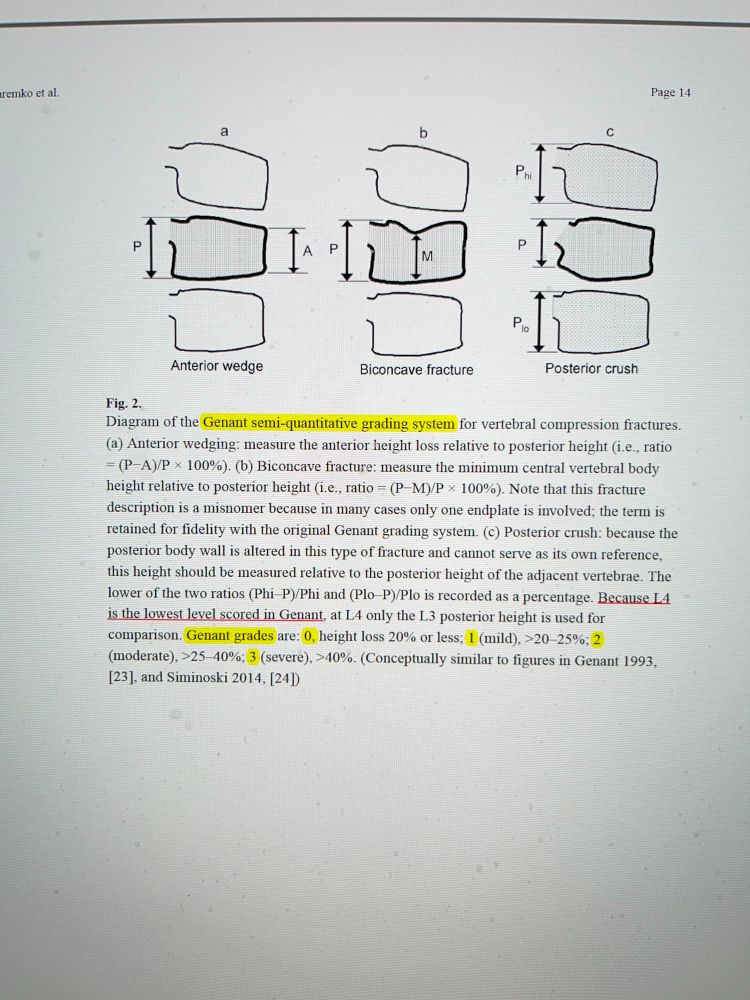
No idea.. btw, the original paper (I haven’t it here right now, I will post it) was about osteoporotic fractures in elderly people, so I think it’s not a good idea to apply Genant classification to post-traumatic vertebral fracture in healthy people (like I often read in reports from elsewhere)🤔
December 28, 2024 at 11:19 PM
No idea.. btw, the original paper (I haven’t it here right now, I will post it) was about osteoporotic fractures in elderly people, so I think it’s not a good idea to apply Genant classification to post-traumatic vertebral fracture in healthy people (like I often read in reports from elsewhere)🤔
I usually use the TLICS score, specifying I’m listing the radiological items only, and the AOSpine. TLICS is good, it was innovative, but later on some issues raised, especially for the evaluation of the integrity of the posterior ligamentous complex (discrepancies with surgical finding are common)🤓
December 28, 2024 at 11:14 PM
I usually use the TLICS score, specifying I’m listing the radiological items only, and the AOSpine. TLICS is good, it was innovative, but later on some issues raised, especially for the evaluation of the integrity of the posterior ligamentous complex (discrepancies with surgical finding are common)🤓
Personally I find l the Genant classification weird (only 5% range for grade 1) and difficult to apply reliably (btw: the original paper is based on few cases), especially with visual evaluation only. If used, the grade should be obtained measuring, not visually 🤓
December 28, 2024 at 11:08 PM
Personally I find l the Genant classification weird (only 5% range for grade 1) and difficult to apply reliably (btw: the original paper is based on few cases), especially with visual evaluation only. If used, the grade should be obtained measuring, not visually 🤓
In 1997 the American College of Physicians issued a position paper stating that in patients w/low pretest probability of Lyme disease, even positive test results do not increase the probability of Lyme disease, since they would have more chances of being a false positive than a true positive 🤦🏼♂️
December 18, 2024 at 7:51 PM
In 1997 the American College of Physicians issued a position paper stating that in patients w/low pretest probability of Lyme disease, even positive test results do not increase the probability of Lyme disease, since they would have more chances of being a false positive than a true positive 🤦🏼♂️
This has also to do with the prevalence of a disease (another rule of screening, btw), and reminds me what happened several years ago with the fake epidemic of Lyme disease, because of which almost any patient with myalgia was suggested to undergo ELISA test for Lyme disease…
December 18, 2024 at 7:49 PM
This has also to do with the prevalence of a disease (another rule of screening, btw), and reminds me what happened several years ago with the fake epidemic of Lyme disease, because of which almost any patient with myalgia was suggested to undergo ELISA test for Lyme disease…
Even talking about “simple” brain or spine MRI: my experience is that patients undergoing brain or spine MRI with 0.001% of chances of a significant finding (explaining the symptoms), “just to be sure and more relaxed”, are NEVER told that their fear can be even bigger after the MRI 🤦🏼♂️.
December 18, 2024 at 7:29 PM
Even talking about “simple” brain or spine MRI: my experience is that patients undergoing brain or spine MRI with 0.001% of chances of a significant finding (explaining the symptoms), “just to be sure and more relaxed”, are NEVER told that their fear can be even bigger after the MRI 🤦🏼♂️.
And, when we inform the patients about WBMRI, how many times do we inform them about the possible scenario of discovering an “unknown thing”, that will need further exams, maybe invasive/dangerous, provoking anxiety/fears/side effects, maybe for nothing? 🤷🏼♂️
December 18, 2024 at 7:25 PM
And, when we inform the patients about WBMRI, how many times do we inform them about the possible scenario of discovering an “unknown thing”, that will need further exams, maybe invasive/dangerous, provoking anxiety/fears/side effects, maybe for nothing? 🤷🏼♂️
I then tried to convince you that WBMRI can be even more dangerous than jumping from a skyscraper roof! 😅 Of course, mine was a provocation, to highlight that medical responsibility (in this and other scenarios) can’t be only “to inform”, letting the patients to get the decision by themselves.
December 18, 2024 at 7:21 PM
I then tried to convince you that WBMRI can be even more dangerous than jumping from a skyscraper roof! 😅 Of course, mine was a provocation, to highlight that medical responsibility (in this and other scenarios) can’t be only “to inform”, letting the patients to get the decision by themselves.
Examples showing why “screening (especially by imaging)” is not always a good thing, even when you find “something”, are endless. Especially when you look at the CNS, where you often can’t solve the diagnostic dilemma of an incidental finding by “biopsying” the brain of a healthy person 🤷🏼♂️
December 18, 2024 at 7:11 PM
Examples showing why “screening (especially by imaging)” is not always a good thing, even when you find “something”, are endless. Especially when you look at the CNS, where you often can’t solve the diagnostic dilemma of an incidental finding by “biopsying” the brain of a healthy person 🤷🏼♂️
Or, again: in the end the patient are so stressed by the idea of having a cerebral aneurysm, that they decide to undergo treatment, for an aneurysm that would never have ruptured, and suffers a complication with permanent neurological deficit, because of an operation they shouldn't have had …
December 18, 2024 at 7:05 PM
Or, again: in the end the patient are so stressed by the idea of having a cerebral aneurysm, that they decide to undergo treatment, for an aneurysm that would never have ruptured, and suffers a complication with permanent neurological deficit, because of an operation they shouldn't have had …
Or, again: incidental small cerebral aneurysm, the patient receives conflicting opinions on what to do (to treat/not to treat), maybe because both decisions can be correct, and they can’t solve the dilemma by themselves. Of course, follow-up will be suggested, but it does not guarantee anything 🤷🏼♂️
December 18, 2024 at 7:02 PM
Or, again: incidental small cerebral aneurysm, the patient receives conflicting opinions on what to do (to treat/not to treat), maybe because both decisions can be correct, and they can’t solve the dilemma by themselves. Of course, follow-up will be suggested, but it does not guarantee anything 🤷🏼♂️
Even worse with incidental aneurysms: are we sure that it is always 👍 to accidentally discover a cerebral aneurysm? Maybe so small that is not considered treatable. But now the patient knows they have it. So, while they had “screening” MRI/MRA done “to feel at ease”,in the end has their life ruined.
December 18, 2024 at 6:52 PM
Even worse with incidental aneurysms: are we sure that it is always 👍 to accidentally discover a cerebral aneurysm? Maybe so small that is not considered treatable. But now the patient knows they have it. So, while they had “screening” MRI/MRA done “to feel at ease”,in the end has their life ruined.
For several reasons, my friend. 1st: how you get a certain diagnosis of a malignant tumor? With further exams,some of them invasive/potentially dangerous. 2nd: does every “mass” we find must be removed?What do we know about the natural history of an incidentally discovered maybe millimetric lesion?
December 18, 2024 at 6:41 PM
For several reasons, my friend. 1st: how you get a certain diagnosis of a malignant tumor? With further exams,some of them invasive/potentially dangerous. 2nd: does every “mass” we find must be removed?What do we know about the natural history of an incidentally discovered maybe millimetric lesion?
“Can we deny someone the right to jump from a skyscraper roof, if they request it & are willing to cover the cost, once we inform them about pros/cons? Ultimately, the decision should rest in their hands”. 😉🙏🏼
December 18, 2024 at 3:12 PM
“Can we deny someone the right to jump from a skyscraper roof, if they request it & are willing to cover the cost, once we inform them about pros/cons? Ultimately, the decision should rest in their hands”. 😉🙏🏼
tough topic, as you obviously know, my friend…Unfortunately, information in this field inevitably suffers from a powerful bias, since it comes from the same side that offers the “screening”, and relies on the anxiety and fears of the people.Not everything that can be bought is also ethically correct
December 18, 2024 at 3:08 PM
tough topic, as you obviously know, my friend…Unfortunately, information in this field inevitably suffers from a powerful bias, since it comes from the same side that offers the “screening”, and relies on the anxiety and fears of the people.Not everything that can be bought is also ethically correct
🙂↔️Screening has got rules (among them, to know exactly in advance WHAT disease you are looking for, that is a treatable disease with proven benefit of early treatment).”Screening” healthy people by putting them into a magnet is indeed a huge business that would sky🚀 incidentalomas and health costs 🤷🏼♂️
December 18, 2024 at 9:32 AM
🙂↔️Screening has got rules (among them, to know exactly in advance WHAT disease you are looking for, that is a treatable disease with proven benefit of early treatment).”Screening” healthy people by putting them into a magnet is indeed a huge business that would sky🚀 incidentalomas and health costs 🤷🏼♂️