


Prof Jeffrey S Morris
@jsm2334.bsky.social
George S Pepper Professor of Public Health & Preventative Medicine; Biostats, Stats & Data Science, Lifelong learner & truth seeker; Views my own & not employer’s
You are correct.
But the encephaly also tends to occur very early so likely occurred long before vaccination
But the encephaly also tends to occur very early so likely occurred long before vaccination
October 2, 2025 at 9:49 PM
You are correct.
But the encephaly also tends to occur very early so likely occurred long before vaccination
But the encephaly also tends to occur very early so likely occurred long before vaccination
You can ask but since they are medical records data and they did not even want this paper getting out, I wouldn’t be optimistic
September 27, 2025 at 6:48 PM
You can ask but since they are medical records data and they did not even want this paper getting out, I wouldn’t be optimistic
Promise! Tell me how successful I was in my attempts to make it accessible, and (mostly) jargon-free
September 26, 2025 at 7:31 PM
Promise! Tell me how successful I was in my attempts to make it accessible, and (mostly) jargon-free
My article is aimed at the general public, so it explains these three statistical issues in accessible language while showing why they matter for interpreting the study’s conclusions.
The link to my full article follows:
theconversation.com/why-a-study-...
The link to my full article follows:
theconversation.com/why-a-study-...

Why a study claiming vaccines cause chronic illness is severely flawed – a biostatistician explains the biases and unsupported conclusions
The main comparisons in the unpublished report are skewed, and it is being presented as stronger evidence than its design really allows.
theconversation.com
September 26, 2025 at 7:19 PM
My article is aimed at the general public, so it explains these three statistical issues in accessible language while showing why they matter for interpreting the study’s conclusions.
The link to my full article follows:
theconversation.com/why-a-study-...
The link to my full article follows:
theconversation.com/why-a-study-...
3. Unadjusted confounders: key factors like urban/rural setting, socioeconomic status/insurance, and air/water pollution weren’t accounted for. These influence both vaccination likelihood and disease risk, as well as how often families use Henry Ford clinics, shaping what shows up in the records
September 26, 2025 at 7:19 PM
3. Unadjusted confounders: key factors like urban/rural setting, socioeconomic status/insurance, and air/water pollution weren’t accounted for. These influence both vaccination likelihood and disease risk, as well as how often families use Henry Ford clinics, shaping what shows up in the records
2. Detection bias – vaccinated children had far more interactions with the Henry Ford health system, giving them more chances to have conditions diagnosed and recorded.
September 26, 2025 at 7:19 PM
2. Detection bias – vaccinated children had far more interactions with the Henry Ford health system, giving them more chances to have conditions diagnosed and recorded.
In short, the study suffers from:
1. Surveillance bias – most children, especially the unvaccinated, weren’t followed long enough to reach the ages when chronic diseases are usually diagnosed.
1. Surveillance bias – most children, especially the unvaccinated, weren’t followed long enough to reach the ages when chronic diseases are usually diagnosed.
September 26, 2025 at 7:19 PM
In short, the study suffers from:
1. Surveillance bias – most children, especially the unvaccinated, weren’t followed long enough to reach the ages when chronic diseases are usually diagnosed.
1. Surveillance bias – most children, especially the unvaccinated, weren’t followed long enough to reach the ages when chronic diseases are usually diagnosed.
Yes.
It just eliminated the choice of getting them together.
Doesn't make much of a difference, but then that begs the question why they spent half a day on it.
Performative, not substantive.
It just eliminated the choice of getting them together.
Doesn't make much of a difference, but then that begs the question why they spent half a day on it.
Performative, not substantive.
September 19, 2025 at 7:28 PM
Yes.
It just eliminated the choice of getting them together.
Doesn't make much of a difference, but then that begs the question why they spent half a day on it.
Performative, not substantive.
It just eliminated the choice of getting them together.
Doesn't make much of a difference, but then that begs the question why they spent half a day on it.
Performative, not substantive.
They noticed the logical inconsistency of their vote yesterday and redid the vote to remove the choice of a single combination shot for ALL children less than 4 years for parents who want them, not just an arbitrary subset of them.
September 19, 2025 at 1:29 PM
They noticed the logical inconsistency of their vote yesterday and redid the vote to remove the choice of a single combination shot for ALL children less than 4 years for parents who want them, not just an arbitrary subset of them.
Outside of that, other children are covered by private insurance, CHIP Medicaid, Indian health service, tricare, and other programs
With ACIP recommending against combined shot for <4yrs, these programs are not guaranteed to cover it anymore.
But they voted to keep covering it for VFC kids only.
With ACIP recommending against combined shot for <4yrs, these programs are not guaranteed to cover it anymore.
But they voted to keep covering it for VFC kids only.
September 19, 2025 at 11:41 AM
Outside of that, other children are covered by private insurance, CHIP Medicaid, Indian health service, tricare, and other programs
With ACIP recommending against combined shot for <4yrs, these programs are not guaranteed to cover it anymore.
But they voted to keep covering it for VFC kids only.
With ACIP recommending against combined shot for <4yrs, these programs are not guaranteed to cover it anymore.
But they voted to keep covering it for VFC kids only.
Yes — the VFC program covers cost of vaccines for children Medicaid-eligible, Uninsured, Underinsured (when vaccines are given at federally qualified health centers or rural health clinics), or American Indian or Alaska Native.
September 19, 2025 at 11:41 AM
Yes — the VFC program covers cost of vaccines for children Medicaid-eligible, Uninsured, Underinsured (when vaccines are given at federally qualified health centers or rural health clinics), or American Indian or Alaska Native.
Ooh! I had that model!
First big purchase after starting to work and saving my own money!
First big purchase after starting to work and saving my own money!
September 13, 2025 at 6:50 PM
Ooh! I had that model!
First big purchase after starting to work and saving my own money!
First big purchase after starting to work and saving my own money!
12/12
Bottom line: Valuable data, but big baseline imbalances, large utilization gaps, and unequal follow-up/age distributions severely limit causal interpretation and are potentially fatal design flaws.
Better design would match on birth year/confounders and censor pairs at the shorter follow-up.
Bottom line: Valuable data, but big baseline imbalances, large utilization gaps, and unequal follow-up/age distributions severely limit causal interpretation and are potentially fatal design flaws.
Better design would match on birth year/confounders and censor pairs at the shorter follow-up.
September 12, 2025 at 3:31 PM
12/12
Bottom line: Valuable data, but big baseline imbalances, large utilization gaps, and unequal follow-up/age distributions severely limit causal interpretation and are potentially fatal design flaws.
Better design would match on birth year/confounders and censor pairs at the shorter follow-up.
Bottom line: Valuable data, but big baseline imbalances, large utilization gaps, and unequal follow-up/age distributions severely limit causal interpretation and are potentially fatal design flaws.
Better design would match on birth year/confounders and censor pairs at the shorter follow-up.
11/12
Sensitivity checks don’t fix it.
Restricting to ≥1/3/5y follow-up yields higher IRRs (2.48 main → 2.75, 3.38, 4.09).
But this doesn't fix the bias:
≥5y still skews older toward vax: ~13.7% of ~1,957 unvax (~268 kids) vs ~29.5% of ~18,468 vax (~5,448). >20× more vax beyond 5y.
Sensitivity checks don’t fix it.
Restricting to ≥1/3/5y follow-up yields higher IRRs (2.48 main → 2.75, 3.38, 4.09).
But this doesn't fix the bias:
≥5y still skews older toward vax: ~13.7% of ~1,957 unvax (~268 kids) vs ~29.5% of ~18,468 vax (~5,448). >20× more vax beyond 5y.

September 12, 2025 at 3:31 PM
11/12
Sensitivity checks don’t fix it.
Restricting to ≥1/3/5y follow-up yields higher IRRs (2.48 main → 2.75, 3.38, 4.09).
But this doesn't fix the bias:
≥5y still skews older toward vax: ~13.7% of ~1,957 unvax (~268 kids) vs ~29.5% of ~18,468 vax (~5,448). >20× more vax beyond 5y.
Sensitivity checks don’t fix it.
Restricting to ≥1/3/5y follow-up yields higher IRRs (2.48 main → 2.75, 3.38, 4.09).
But this doesn't fix the bias:
≥5y still skews older toward vax: ~13.7% of ~1,957 unvax (~268 kids) vs ~29.5% of ~18,468 vax (~5,448). >20× more vax beyond 5y.
10/12
Many conditions are typically diagnosed later:
behavioral 7–12y, learning ~8.4y, autoimmune ~5.5–8y, asthma ~6.6y, ADHD ~6y, autism ~4y, speech/dev delay ~3–4y.
More vax kids age into these windows; vast majority of unvax cases aren’t captured yet.
Many conditions are typically diagnosed later:
behavioral 7–12y, learning ~8.4y, autoimmune ~5.5–8y, asthma ~6.6y, ADHD ~6y, autism ~4y, speech/dev delay ~3–4y.
More vax kids age into these windows; vast majority of unvax cases aren’t captured yet.
September 12, 2025 at 3:31 PM
10/12
Many conditions are typically diagnosed later:
behavioral 7–12y, learning ~8.4y, autoimmune ~5.5–8y, asthma ~6.6y, ADHD ~6y, autism ~4y, speech/dev delay ~3–4y.
More vax kids age into these windows; vast majority of unvax cases aren’t captured yet.
Many conditions are typically diagnosed later:
behavioral 7–12y, learning ~8.4y, autoimmune ~5.5–8y, asthma ~6.6y, ADHD ~6y, autism ~4y, speech/dev delay ~3–4y.
More vax kids age into these windows; vast majority of unvax cases aren’t captured yet.
9/12
Concern #3: unequal follow-up/age
Median follow-up: ~2.7y (vax) vs ~1.3y (unvax).
IQR: 1.3–5.7y vs 0.5–3.0y
This means unvaccinated have 25% with <0.5y follow up, 50% with <1.3y, only 25% >3.0y
Vax: 25% <1.3y, 50% <2.7y, 25% >5.7y
Here is lognormal fit estimating follow-up distribution
Concern #3: unequal follow-up/age
Median follow-up: ~2.7y (vax) vs ~1.3y (unvax).
IQR: 1.3–5.7y vs 0.5–3.0y
This means unvaccinated have 25% with <0.5y follow up, 50% with <1.3y, only 25% >3.0y
Vax: 25% <1.3y, 50% <2.7y, 25% >5.7y
Here is lognormal fit estimating follow-up distribution
September 12, 2025 at 3:31 PM
9/12
Concern #3: unequal follow-up/age
Median follow-up: ~2.7y (vax) vs ~1.3y (unvax).
IQR: 1.3–5.7y vs 0.5–3.0y
This means unvaccinated have 25% with <0.5y follow up, 50% with <1.3y, only 25% >3.0y
Vax: 25% <1.3y, 50% <2.7y, 25% >5.7y
Here is lognormal fit estimating follow-up distribution
Concern #3: unequal follow-up/age
Median follow-up: ~2.7y (vax) vs ~1.3y (unvax).
IQR: 1.3–5.7y vs 0.5–3.0y
This means unvaccinated have 25% with <0.5y follow up, 50% with <1.3y, only 25% >3.0y
Vax: 25% <1.3y, 50% <2.7y, 25% >5.7y
Here is lognormal fit estimating follow-up distribution
8/12
Concern #2: utilization/ascertainment bias.
Many diagnoses need multiple visits (ADHD ~3–4).
Visits/yr: ~7 (vax) vs ~2 (unvax) → ~3.5× more chance to detect/capture codes.
Sensitivity analysis excluding zero-visit kids reduces effects but doesn’t fix the disparity.
Concern #2: utilization/ascertainment bias.
Many diagnoses need multiple visits (ADHD ~3–4).
Visits/yr: ~7 (vax) vs ~2 (unvax) → ~3.5× more chance to detect/capture codes.
Sensitivity analysis excluding zero-visit kids reduces effects but doesn’t fix the disparity.
September 12, 2025 at 3:31 PM
8/12
Concern #2: utilization/ascertainment bias.
Many diagnoses need multiple visits (ADHD ~3–4).
Visits/yr: ~7 (vax) vs ~2 (unvax) → ~3.5× more chance to detect/capture codes.
Sensitivity analysis excluding zero-visit kids reduces effects but doesn’t fix the disparity.
Concern #2: utilization/ascertainment bias.
Many diagnoses need multiple visits (ADHD ~3–4).
Visits/yr: ~7 (vax) vs ~2 (unvax) → ~3.5× more chance to detect/capture codes.
Sensitivity analysis excluding zero-visit kids reduces effects but doesn’t fix the disparity.
7/12
Massive differencs suggest potential for unmeasured confounding (SES, prenatal exposures, parental age, pollution exposure, urban/rural).
If birth years differ, birth cohort effects can confound (diagnostics, coding, vaccine schedules).
IRRs/“raw” HRs are unadjusted → interpret cautiously.
Massive differencs suggest potential for unmeasured confounding (SES, prenatal exposures, parental age, pollution exposure, urban/rural).
If birth years differ, birth cohort effects can confound (diagnostics, coding, vaccine schedules).
IRRs/“raw” HRs are unadjusted → interpret cautiously.

September 12, 2025 at 3:31 PM
7/12
Massive differencs suggest potential for unmeasured confounding (SES, prenatal exposures, parental age, pollution exposure, urban/rural).
If birth years differ, birth cohort effects can confound (diagnostics, coding, vaccine schedules).
IRRs/“raw” HRs are unadjusted → interpret cautiously.
Massive differencs suggest potential for unmeasured confounding (SES, prenatal exposures, parental age, pollution exposure, urban/rural).
If birth years differ, birth cohort effects can confound (diagnostics, coding, vaccine schedules).
IRRs/“raw” HRs are unadjusted → interpret cautiously.
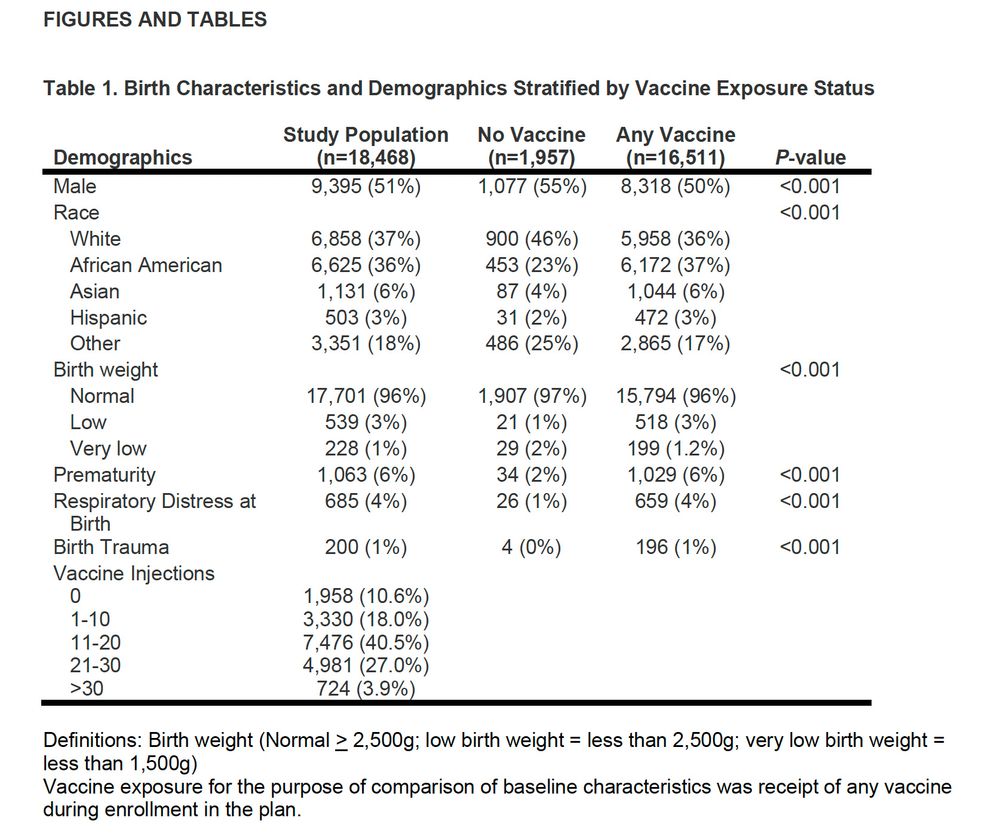
6/12
Concern #1: non-comparable groups.
Baseline table: every variable differs (P<0.0001)—sex, race, birthweight, prematurity, respiratory distress, birth trauma. Crude ORs (vax vs unvax): prematurity 3.8×; resp. distress 3.2×; low BW 1.7×; birth trauma 5.9×.
Concern #1: non-comparable groups.
Baseline table: every variable differs (P<0.0001)—sex, race, birthweight, prematurity, respiratory distress, birth trauma. Crude ORs (vax vs unvax): prematurity 3.8×; resp. distress 3.2×; low BW 1.7×; birth trauma 5.9×.
September 12, 2025 at 3:31 PM
6/12
Concern #1: non-comparable groups.
Baseline table: every variable differs (P<0.0001)—sex, race, birthweight, prematurity, respiratory distress, birth trauma. Crude ORs (vax vs unvax): prematurity 3.8×; resp. distress 3.2×; low BW 1.7×; birth trauma 5.9×.
Concern #1: non-comparable groups.
Baseline table: every variable differs (P<0.0001)—sex, race, birthweight, prematurity, respiratory distress, birth trauma. Crude ORs (vax vs unvax): prematurity 3.8×; resp. distress 3.2×; low BW 1.7×; birth trauma 5.9×.
5/12
Autism is the outlier: adjusted HR ≈ 0.6 (no increase). Few autism diagnoses—unsurprising given short follow-up.
Not discussed or highlighted -- Aaron Siri claims this result is from ADHD misclassification but this is speculative and not supported by the presented results.
Autism is the outlier: adjusted HR ≈ 0.6 (no increase). Few autism diagnoses—unsurprising given short follow-up.
Not discussed or highlighted -- Aaron Siri claims this result is from ADHD misclassification but this is speculative and not supported by the presented results.
September 12, 2025 at 3:31 PM
5/12
Autism is the outlier: adjusted HR ≈ 0.6 (no increase). Few autism diagnoses—unsurprising given short follow-up.
Not discussed or highlighted -- Aaron Siri claims this result is from ADHD misclassification but this is speculative and not supported by the presented results.
Autism is the outlier: adjusted HR ≈ 0.6 (no increase). Few autism diagnoses—unsurprising given short follow-up.
Not discussed or highlighted -- Aaron Siri claims this result is from ADHD misclassification but this is speculative and not supported by the presented results.
4/12
No clear differences reported for eczema, peanut allergy, overall food allergy, cancer, mental health disorders, seizures, motor disability.
Neurodevelopmental (composite) found increase of ~5.5×
specific categories within this include: developmental delay ~3.3×, motor ~2.9×, speech ~4.5×.
No clear differences reported for eczema, peanut allergy, overall food allergy, cancer, mental health disorders, seizures, motor disability.
Neurodevelopmental (composite) found increase of ~5.5×
specific categories within this include: developmental delay ~3.3×, motor ~2.9×, speech ~4.5×.
September 12, 2025 at 3:31 PM
4/12
No clear differences reported for eczema, peanut allergy, overall food allergy, cancer, mental health disorders, seizures, motor disability.
Neurodevelopmental (composite) found increase of ~5.5×
specific categories within this include: developmental delay ~3.3×, motor ~2.9×, speech ~4.5×.
No clear differences reported for eczema, peanut allergy, overall food allergy, cancer, mental health disorders, seizures, motor disability.
Neurodevelopmental (composite) found increase of ~5.5×
specific categories within this include: developmental delay ~3.3×, motor ~2.9×, speech ~4.5×.