


Pete Hart
@intensiveperson.bsky.social
Not generalisable from Aus/NZ. We have very different incidence rates from NAP6 in the UK

November 13, 2025 at 8:34 AM
Not generalisable from Aus/NZ. We have very different incidence rates from NAP6 in the UK
There are still plenty of arterial trauma incidents from CVCs now - mixture of all ages of dogs and all ages of trick! tiny.cc/hartcvc again

September 4, 2025 at 1:36 PM
There are still plenty of arterial trauma incidents from CVCs now - mixture of all ages of dogs and all ages of trick! tiny.cc/hartcvc again
Have you read my paper? Lots of strokes and deaths in there from arterial trauma, many of whom befell operators who had never had a prior major complication. It only takes one... tiny.cc/hartcvc
September 4, 2025 at 8:44 AM
Have you read my paper? Lots of strokes and deaths in there from arterial trauma, many of whom befell operators who had never had a prior major complication. It only takes one... tiny.cc/hartcvc
Specifically for exsanguinating haemorrhage - I'm surprised some people aren't aware of the debate on this. Discussed briefly here, for example:
www.surgjournal.com/article/S003...
www.surgjournal.com/article/S003...

September 3, 2025 at 8:53 PM
Specifically for exsanguinating haemorrhage - I'm surprised some people aren't aware of the debate on this. Discussed briefly here, for example:
www.surgjournal.com/article/S003...
www.surgjournal.com/article/S003...
Awful. I'm just going to leave this here: yes, bronchospasm can account for a flat capnograph, but no, you can't assume that's the reason and you must take the tube out or (if that's genuinely dangerous) exclude oesophageal intubation using a bronchoscope.
onlinelibrary.wiley.com/share/author...
onlinelibrary.wiley.com/share/author...

September 1, 2025 at 11:22 AM
Awful. I'm just going to leave this here: yes, bronchospasm can account for a flat capnograph, but no, you can't assume that's the reason and you must take the tube out or (if that's genuinely dangerous) exclude oesophageal intubation using a bronchoscope.
onlinelibrary.wiley.com/share/author...
onlinelibrary.wiley.com/share/author...

Finally, a special mention for this wonderful example: class 2 = horrifically elongated uvula. (www.mediconotebook.com/2012/11/mall...)

August 1, 2025 at 1:12 PM
Finally, a special mention for this wonderful example: class 2 = horrifically elongated uvula. (www.mediconotebook.com/2012/11/mall...)
Let's nip back to a random website (mobile.fpnotebook.com/ENT/Exam/Mlm...) who have a diagram with an indistinguishable Class 1 and Class 2 - oh, wait, something about 50% of the tonsil being visible? That's new. Do I have to go in there and measure it to be sure?

August 1, 2025 at 1:12 PM
Let's nip back to a random website (mobile.fpnotebook.com/ENT/Exam/Mlm...) who have a diagram with an indistinguishable Class 1 and Class 2 - oh, wait, something about 50% of the tonsil being visible? That's new. Do I have to go in there and measure it to be sure?
OK, I hear you: using diagrams from private OSA clinics might be considered a straw man argument. So here's a peer-reviewed paper with a Class 3 which is again just a slightly worse Class 2 (diagram reproduced from UpToDate). pubmed.ncbi.nlm.nih.gov/29560077/

August 1, 2025 at 1:12 PM
OK, I hear you: using diagrams from private OSA clinics might be considered a straw man argument. So here's a peer-reviewed paper with a Class 3 which is again just a slightly worse Class 2 (diagram reproduced from UpToDate). pubmed.ncbi.nlm.nih.gov/29560077/
For a bit of variety, this time Class 3 and 4 are indistinguishable. www.sleepfoundation.org/sleep-apnea/...

August 1, 2025 at 1:12 PM
For a bit of variety, this time Class 3 and 4 are indistinguishable. www.sleepfoundation.org/sleep-apnea/...
This is a common option. Class 2 and 3 are essentially identical (same structures visible), but Class 3 is just marginally worse. Meanwhile, the descriptions don't match the diagrams for Class 1 or 2. www.clinicaladvisor.com/features/und...

August 1, 2025 at 1:12 PM
This is a common option. Class 2 and 3 are essentially identical (same structures visible), but Class 3 is just marginally worse. Meanwhile, the descriptions don't match the diagrams for Class 1 or 2. www.clinicaladvisor.com/features/und...
This is a classic case of the disappearing uvula: the illustrator knows there has to be a difference between class 2 and 3 but isn't sure what it is, so the uvula is just... stumpy?? Or obscured by a mysterious shadow? jamanetwork.com/journals/jam...

August 1, 2025 at 1:12 PM
This is a classic case of the disappearing uvula: the illustrator knows there has to be a difference between class 2 and 3 but isn't sure what it is, so the uvula is just... stumpy?? Or obscured by a mysterious shadow? jamanetwork.com/journals/jam...
The Mallampati score is probably only marginally better; and as with the ASA score, the information you gather to decide the score is far more useful than the score itself.

July 31, 2025 at 10:51 PM
The Mallampati score is probably only marginally better; and as with the ASA score, the information you gather to decide the score is far more useful than the score itself.
CVCs are drug-delivery devices. Both absolute values and trends of CVP have been demonstrated to correlate poorly with volume status/fluid-responsiveness, although it remains useful to assess right heart status in the absence of echocardiography skills. Peripheral NA is great - up to a point.

June 27, 2025 at 2:26 PM
CVCs are drug-delivery devices. Both absolute values and trends of CVP have been demonstrated to correlate poorly with volume status/fluid-responsiveness, although it remains useful to assess right heart status in the absence of echocardiography skills. Peripheral NA is great - up to a point.
These are both "ramped". This is problematic because (like RSI) people aren't paying attention to what the useful components are actually doing.


June 8, 2025 at 2:11 PM
These are both "ramped". This is problematic because (like RSI) people aren't paying attention to what the useful components are actually doing.
Out of 241 reported incidents of arterial trauma from CVC insertion, in 75 cases initial confirmatory checks (if any) failed to identify arterial cannulation. CXR most commonly implicated in this, with blood gas/transduction failing for mostly predictable reasons. What's your department's practice?

February 24, 2025 at 11:50 AM
Out of 241 reported incidents of arterial trauma from CVC insertion, in 75 cases initial confirmatory checks (if any) failed to identify arterial cannulation. CXR most commonly implicated in this, with blood gas/transduction failing for mostly predictable reasons. What's your department's practice?
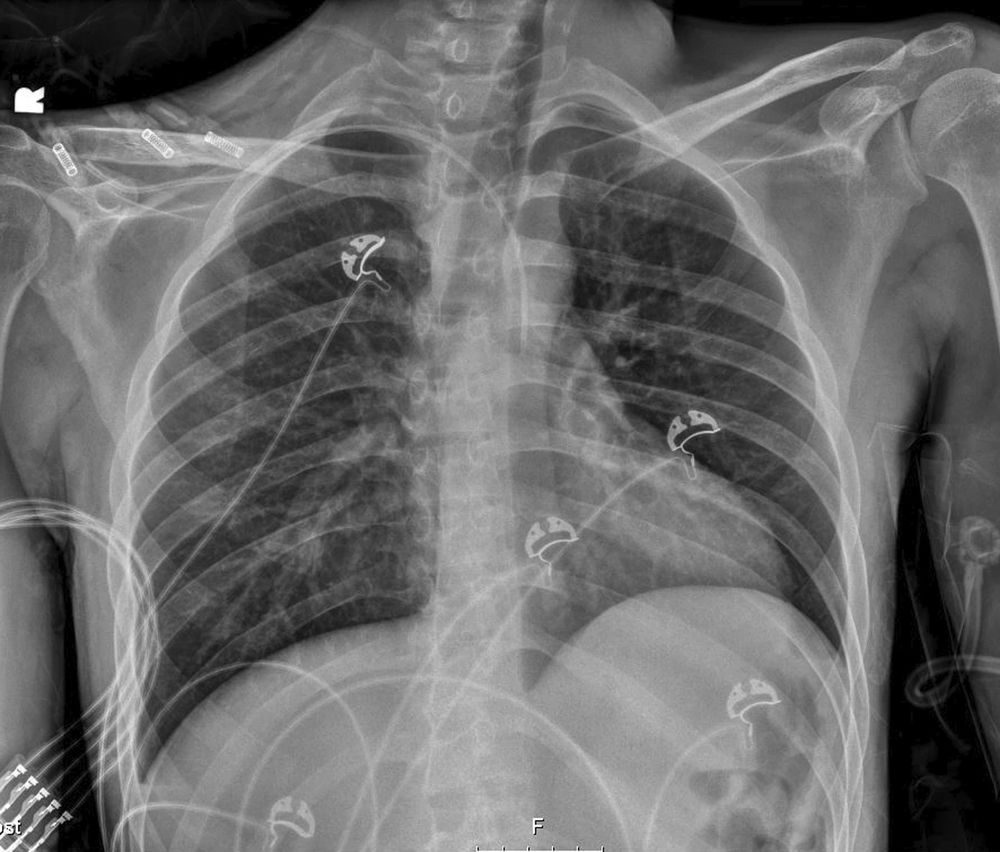
You'll have a better chance if you've seen them before. Suspect any line which doesn't follow the normal course (tip in lower half of right mediastinum, pointing caudally; L line crosses midline, R doesn't). But it's basically the wrong test for this question; confirm a venous pressure waveform!
February 23, 2025 at 7:28 AM
You'll have a better chance if you've seen them before. Suspect any line which doesn't follow the normal course (tip in lower half of right mediastinum, pointing caudally; L line crosses midline, R doesn't). But it's basically the wrong test for this question; confirm a venous pressure waveform!