




GoggleDocs
@goggledocs.bsky.social
Docs/nurses/pharmacists from U.K. Talking CardioRenoMetabolic (#CaReMe) & more Catch us on YouTube http://youtube.com/c/GoggleDocs |Educate, Motivate, Activate!
📢 TyG-BMI: a new vital sign in #MASLD?
🔹 NHANES study: TyG-BMI ⤴️ = ⤴️ all-cause ☠️ & 💔☠️
🔸 U-shaped risk curve—both high & low TyG-BMI = ⤴️ risk
🔹 HbA1c mediated most of the effect
👉 For MASLD, insulin resistance isn’t just present—it’s predictive❗️
🔗 ggdocs.co/9cu63n
@pharmrj.pharmsky.app
🔹 NHANES study: TyG-BMI ⤴️ = ⤴️ all-cause ☠️ & 💔☠️
🔸 U-shaped risk curve—both high & low TyG-BMI = ⤴️ risk
🔹 HbA1c mediated most of the effect
👉 For MASLD, insulin resistance isn’t just present—it’s predictive❗️
🔗 ggdocs.co/9cu63n
@pharmrj.pharmsky.app


May 10, 2025 at 10:01 AM
📢 TyG-BMI: a new vital sign in #MASLD?
🔹 NHANES study: TyG-BMI ⤴️ = ⤴️ all-cause ☠️ & 💔☠️
🔸 U-shaped risk curve—both high & low TyG-BMI = ⤴️ risk
🔹 HbA1c mediated most of the effect
👉 For MASLD, insulin resistance isn’t just present—it’s predictive❗️
🔗 ggdocs.co/9cu63n
@pharmrj.pharmsky.app
🔹 NHANES study: TyG-BMI ⤴️ = ⤴️ all-cause ☠️ & 💔☠️
🔸 U-shaped risk curve—both high & low TyG-BMI = ⤴️ risk
🔹 HbA1c mediated most of the effect
👉 For MASLD, insulin resistance isn’t just present—it’s predictive❗️
🔗 ggdocs.co/9cu63n
@pharmrj.pharmsky.app
📢 Can LFTs track liver fat loss after weight loss in #T2D❓
🔹 DiRECT sub-study: 74% achieved MASLD remission with ~12kg wt loss
🔸 ⤵️ ALT & GGT= predictors of liver fat ⤵️ (ALT >40 = PPV 100%)
🔹 ALT change most closely linked to liver fat ⤵️
👉LFTs = simple tool to track remission
🔗 ggdocs.co/9g8ffo
🔹 DiRECT sub-study: 74% achieved MASLD remission with ~12kg wt loss
🔸 ⤵️ ALT & GGT= predictors of liver fat ⤵️ (ALT >40 = PPV 100%)
🔹 ALT change most closely linked to liver fat ⤵️
👉LFTs = simple tool to track remission
🔗 ggdocs.co/9g8ffo

May 2, 2025 at 3:36 PM
📢 Can LFTs track liver fat loss after weight loss in #T2D❓
🔹 DiRECT sub-study: 74% achieved MASLD remission with ~12kg wt loss
🔸 ⤵️ ALT & GGT= predictors of liver fat ⤵️ (ALT >40 = PPV 100%)
🔹 ALT change most closely linked to liver fat ⤵️
👉LFTs = simple tool to track remission
🔗 ggdocs.co/9g8ffo
🔹 DiRECT sub-study: 74% achieved MASLD remission with ~12kg wt loss
🔸 ⤵️ ALT & GGT= predictors of liver fat ⤵️ (ALT >40 = PPV 100%)
🔹 ALT change most closely linked to liver fat ⤵️
👉LFTs = simple tool to track remission
🔗 ggdocs.co/9g8ffo
Who’s getting #GLP1 for #obesity 🇺🇸❓
🔹 <3% of 39M eligible pts got Sema/tirz
🔸 ⚫️⚪️ ⚠️ Px lower in ♂️, ⚫️/Asian/Hispanic pts, high SVI & rural area
🔹 Uptake ⤴️ overall, but disparities persist
🔸 Reflects system-level barriers
👉 #ObesityCare evolving—equity must catch up❗️
🔗 ggdocs.co/ao046p
🔹 <3% of 39M eligible pts got Sema/tirz
🔸 ⚫️⚪️ ⚠️ Px lower in ♂️, ⚫️/Asian/Hispanic pts, high SVI & rural area
🔹 Uptake ⤴️ overall, but disparities persist
🔸 Reflects system-level barriers
👉 #ObesityCare evolving—equity must catch up❗️
🔗 ggdocs.co/ao046p



April 30, 2025 at 12:52 PM
Who’s getting #GLP1 for #obesity 🇺🇸❓
🔹 <3% of 39M eligible pts got Sema/tirz
🔸 ⚫️⚪️ ⚠️ Px lower in ♂️, ⚫️/Asian/Hispanic pts, high SVI & rural area
🔹 Uptake ⤴️ overall, but disparities persist
🔸 Reflects system-level barriers
👉 #ObesityCare evolving—equity must catch up❗️
🔗 ggdocs.co/ao046p
🔹 <3% of 39M eligible pts got Sema/tirz
🔸 ⚫️⚪️ ⚠️ Px lower in ♂️, ⚫️/Asian/Hispanic pts, high SVI & rural area
🔹 Uptake ⤴️ overall, but disparities persist
🔸 Reflects system-level barriers
👉 #ObesityCare evolving—equity must catch up❗️
🔗 ggdocs.co/ao046p
📢 #GLP1 ⤵️ kidney decline, CV events & mortality in CKD❗️
🔹 Meta-analysis of 18K pts w/ eGFR <60:
⤵️ eGFR decline ≥50% (OR 0.72)
⤵️ 💔 (OR 0.86)
⤵️ ☠️ (OR 0.77)
🔸 ⤵️⤵️ with human GLP-1 backbone
🥇Evidence across CKD stages—not just macroalbuminuria
👉 GLP-1 now a key 🎯 in CKD + #T2D
🔗 ggdocs.co/tnqomz
🔹 Meta-analysis of 18K pts w/ eGFR <60:
⤵️ eGFR decline ≥50% (OR 0.72)
⤵️ 💔 (OR 0.86)
⤵️ ☠️ (OR 0.77)
🔸 ⤵️⤵️ with human GLP-1 backbone
🥇Evidence across CKD stages—not just macroalbuminuria
👉 GLP-1 now a key 🎯 in CKD + #T2D
🔗 ggdocs.co/tnqomz

March 22, 2025 at 11:54 AM
📢 #GLP1 ⤵️ kidney decline, CV events & mortality in CKD❗️
🔹 Meta-analysis of 18K pts w/ eGFR <60:
⤵️ eGFR decline ≥50% (OR 0.72)
⤵️ 💔 (OR 0.86)
⤵️ ☠️ (OR 0.77)
🔸 ⤵️⤵️ with human GLP-1 backbone
🥇Evidence across CKD stages—not just macroalbuminuria
👉 GLP-1 now a key 🎯 in CKD + #T2D
🔗 ggdocs.co/tnqomz
🔹 Meta-analysis of 18K pts w/ eGFR <60:
⤵️ eGFR decline ≥50% (OR 0.72)
⤵️ 💔 (OR 0.86)
⤵️ ☠️ (OR 0.77)
🔸 ⤵️⤵️ with human GLP-1 backbone
🥇Evidence across CKD stages—not just macroalbuminuria
👉 GLP-1 now a key 🎯 in CKD + #T2D
🔗 ggdocs.co/tnqomz
Oral semaglutide cost-effective vs. liraglutide—even at 50% ⤵️ price
🔹 🇬🇧 modelled data: ⤴️ QALYs (+0.18) & ⤵️ comp.
🔸 💊 = ⤵️ Rx burden vs. daily 💉
🔹 Results robust across sensitivity analyses
⚠️ funded by NovoNordisk
👉 Challenges low-cost liraglutide, supports 🎯 oral GLP-1 use
🔗 ggdocs.co/9h0bz1
🔹 🇬🇧 modelled data: ⤴️ QALYs (+0.18) & ⤵️ comp.
🔸 💊 = ⤵️ Rx burden vs. daily 💉
🔹 Results robust across sensitivity analyses
⚠️ funded by NovoNordisk
👉 Challenges low-cost liraglutide, supports 🎯 oral GLP-1 use
🔗 ggdocs.co/9h0bz1



March 21, 2025 at 12:45 PM
Oral semaglutide cost-effective vs. liraglutide—even at 50% ⤵️ price
🔹 🇬🇧 modelled data: ⤴️ QALYs (+0.18) & ⤵️ comp.
🔸 💊 = ⤵️ Rx burden vs. daily 💉
🔹 Results robust across sensitivity analyses
⚠️ funded by NovoNordisk
👉 Challenges low-cost liraglutide, supports 🎯 oral GLP-1 use
🔗 ggdocs.co/9h0bz1
🔹 🇬🇧 modelled data: ⤴️ QALYs (+0.18) & ⤵️ comp.
🔸 💊 = ⤵️ Rx burden vs. daily 💉
🔹 Results robust across sensitivity analyses
⚠️ funded by NovoNordisk
👉 Challenges low-cost liraglutide, supports 🎯 oral GLP-1 use
🔗 ggdocs.co/9h0bz1
Albuminuria: The CKM biomarker we’re overlooking❗️
🥇 risk biomarker
🔹 Even UACR <3.4 mg/mmol = ⤴️ #CVD, #CKD & ☠️ risk
🔸 Signals early endothelial dysfunc. in HTN, #T2D, #HF & #MASLD
🔹 Yet 💧screening rates low
🔸 Newer Rx (SGLT2i, #GLP1 , nsMRA) = 🎯
⌛detect, disclose & treat❗️
🔗 ggdocs.co/hot30b
🥇 risk biomarker
🔹 Even UACR <3.4 mg/mmol = ⤴️ #CVD, #CKD & ☠️ risk
🔸 Signals early endothelial dysfunc. in HTN, #T2D, #HF & #MASLD
🔹 Yet 💧screening rates low
🔸 Newer Rx (SGLT2i, #GLP1 , nsMRA) = 🎯
⌛detect, disclose & treat❗️
🔗 ggdocs.co/hot30b

March 14, 2025 at 10:36 AM
GLP-1 & blood cancer risk: Encouraging signal in cohort study
🔹 #T2D patients on GLP-1 ⤵️ risk vs. insulin for hematological cancers (HR 0.46)
🔸 ⤵️ risk of MDS, MPN, leukaemia, lymphoma & myeloma
🔹 No benefit vs. met
🔸 ⚠️ RWD = unresolved bias
👉 Supports 🎯 trials ⤵️cancer
🔗 ggdocs.co/3yosuj
🔹 #T2D patients on GLP-1 ⤵️ risk vs. insulin for hematological cancers (HR 0.46)
🔸 ⤵️ risk of MDS, MPN, leukaemia, lymphoma & myeloma
🔹 No benefit vs. met
🔸 ⚠️ RWD = unresolved bias
👉 Supports 🎯 trials ⤵️cancer
🔗 ggdocs.co/3yosuj

March 12, 2025 at 5:51 PM
GLP-1 & blood cancer risk: Encouraging signal in cohort study
🔹 #T2D patients on GLP-1 ⤵️ risk vs. insulin for hematological cancers (HR 0.46)
🔸 ⤵️ risk of MDS, MPN, leukaemia, lymphoma & myeloma
🔹 No benefit vs. met
🔸 ⚠️ RWD = unresolved bias
👉 Supports 🎯 trials ⤵️cancer
🔗 ggdocs.co/3yosuj
🔹 #T2D patients on GLP-1 ⤵️ risk vs. insulin for hematological cancers (HR 0.46)
🔸 ⤵️ risk of MDS, MPN, leukaemia, lymphoma & myeloma
🔹 No benefit vs. met
🔸 ⚠️ RWD = unresolved bias
👉 Supports 🎯 trials ⤵️cancer
🔗 ggdocs.co/3yosuj
#Finerenone: CV & renal protection across all #T2D therapies❗️
🔹 Pooled analysis: 15,365 pts w/ T2D + CKD or CV
🔸 Consistent benefit on 💔☠️, 🏥💔& kidney outcomes
🔹 ⤴️K+ ⤵️ with SGLT2i use
🔸 Benefit independent of SGLT2i/GLP-1 use
👉 Supports finerenone as a 🎯 in high-risk #T2D❗️
🔗 ggdocs.co/tx2a5r
🔹 Pooled analysis: 15,365 pts w/ T2D + CKD or CV
🔸 Consistent benefit on 💔☠️, 🏥💔& kidney outcomes
🔹 ⤴️K+ ⤵️ with SGLT2i use
🔸 Benefit independent of SGLT2i/GLP-1 use
👉 Supports finerenone as a 🎯 in high-risk #T2D❗️
🔗 ggdocs.co/tx2a5r

March 5, 2025 at 7:54 PM
#Finerenone: CV & renal protection across all #T2D therapies❗️
🔹 Pooled analysis: 15,365 pts w/ T2D + CKD or CV
🔸 Consistent benefit on 💔☠️, 🏥💔& kidney outcomes
🔹 ⤴️K+ ⤵️ with SGLT2i use
🔸 Benefit independent of SGLT2i/GLP-1 use
👉 Supports finerenone as a 🎯 in high-risk #T2D❗️
🔗 ggdocs.co/tx2a5r
🔹 Pooled analysis: 15,365 pts w/ T2D + CKD or CV
🔸 Consistent benefit on 💔☠️, 🏥💔& kidney outcomes
🔹 ⤴️K+ ⤵️ with SGLT2i use
🔸 Benefit independent of SGLT2i/GLP-1 use
👉 Supports finerenone as a 🎯 in high-risk #T2D❗️
🔗 ggdocs.co/tx2a5r
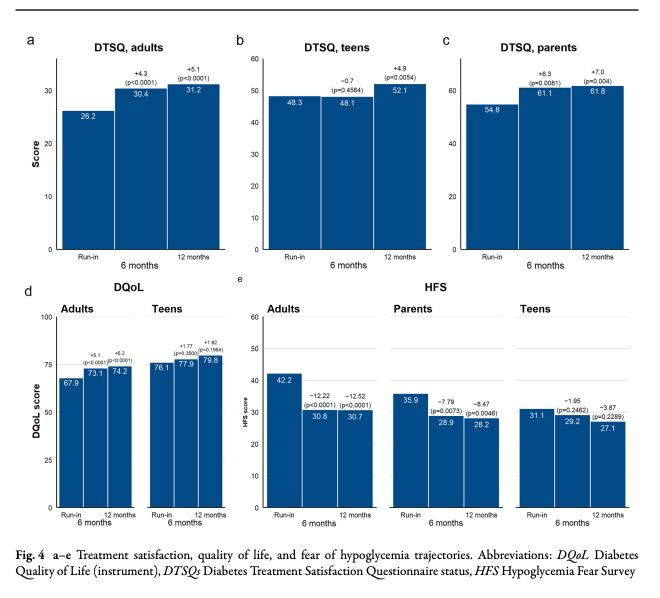
📢 #T1D Closed-Loop: MiniMed™ 780G in Real-World France
🔹 TIR ⤴️ 11.8% (2.8h/day) at 6m, HbA1c ⤵️ 0.52%
🔸 Hypoglycemia risk ⤵️, zero severe hypos @ 12m
🔹 Diabetes distress ⤵️ & QoL ⤴️ in adults & teens
🔸 Fear of hypos ⤵️ in adults & children
👉 HCL the new standard in #DiabetesCare❗️
🔗 ggdocs.co/pwpsiu
🔹 TIR ⤴️ 11.8% (2.8h/day) at 6m, HbA1c ⤵️ 0.52%
🔸 Hypoglycemia risk ⤵️, zero severe hypos @ 12m
🔹 Diabetes distress ⤵️ & QoL ⤴️ in adults & teens
🔸 Fear of hypos ⤵️ in adults & children
👉 HCL the new standard in #DiabetesCare❗️
🔗 ggdocs.co/pwpsiu

February 28, 2025 at 11:15 AM
📢 #T1D Closed-Loop: MiniMed™ 780G in Real-World France
🔹 TIR ⤴️ 11.8% (2.8h/day) at 6m, HbA1c ⤵️ 0.52%
🔸 Hypoglycemia risk ⤵️, zero severe hypos @ 12m
🔹 Diabetes distress ⤵️ & QoL ⤴️ in adults & teens
🔸 Fear of hypos ⤵️ in adults & children
👉 HCL the new standard in #DiabetesCare❗️
🔗 ggdocs.co/pwpsiu
🔹 TIR ⤴️ 11.8% (2.8h/day) at 6m, HbA1c ⤵️ 0.52%
🔸 Hypoglycemia risk ⤵️, zero severe hypos @ 12m
🔹 Diabetes distress ⤵️ & QoL ⤴️ in adults & teens
🔸 Fear of hypos ⤵️ in adults & children
👉 HCL the new standard in #DiabetesCare❗️
🔗 ggdocs.co/pwpsiu
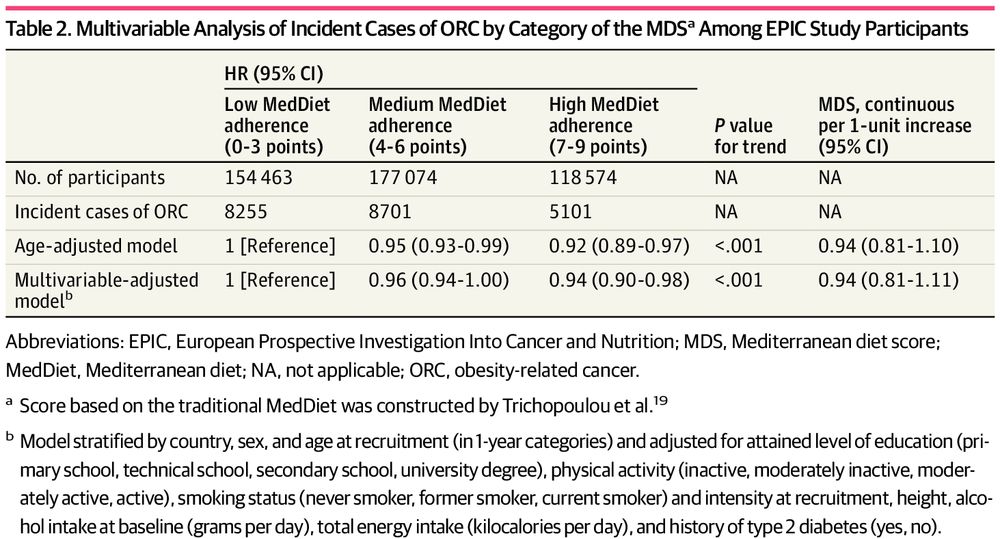
📢 Mediterranean Diet: A Recipe for Cancer Prevention?
🇬🇧1 in 10 cancers - Obesity related (ORC)
🔹 n450,111, 15y follow-up in EPIC study
🔸 6% ⤵️ risk ORC withMedDiet adherence (HR 0.94)
🔹 Colorectal, liver, kidney cancer ⤵️
🔸 Not weight—no mediation via BMI/waist-to-hip ratio
🔗 ggdocs.co/7larkw
🇬🇧1 in 10 cancers - Obesity related (ORC)
🔹 n450,111, 15y follow-up in EPIC study
🔸 6% ⤵️ risk ORC withMedDiet adherence (HR 0.94)
🔹 Colorectal, liver, kidney cancer ⤵️
🔸 Not weight—no mediation via BMI/waist-to-hip ratio
🔗 ggdocs.co/7larkw

February 27, 2025 at 8:31 PM
📢 Mediterranean Diet: A Recipe for Cancer Prevention?
🇬🇧1 in 10 cancers - Obesity related (ORC)
🔹 n450,111, 15y follow-up in EPIC study
🔸 6% ⤵️ risk ORC withMedDiet adherence (HR 0.94)
🔹 Colorectal, liver, kidney cancer ⤵️
🔸 Not weight—no mediation via BMI/waist-to-hip ratio
🔗 ggdocs.co/7larkw
🇬🇧1 in 10 cancers - Obesity related (ORC)
🔹 n450,111, 15y follow-up in EPIC study
🔸 6% ⤵️ risk ORC withMedDiet adherence (HR 0.94)
🔹 Colorectal, liver, kidney cancer ⤵️
🔸 Not weight—no mediation via BMI/waist-to-hip ratio
🔗 ggdocs.co/7larkw
MASLD: ‘Elephant in the Room’ of #CKM
🔹 🌍 crisis: 1/3 adults affected, 65% in #T2D
🔸 Liver fibrosis=predictor of ☠️ & #CVD, #CKD,&HCC
🔹 No approved Rx – 🎯 lifestyle, ⤵️weight & multi-specialty care
🔸 Future hope: GLP-1s, PPAR, THR-β agonists
👉 Access the full paper via link
🔗 ggdocs.co/dz0kai
🔹 🌍 crisis: 1/3 adults affected, 65% in #T2D
🔸 Liver fibrosis=predictor of ☠️ & #CVD, #CKD,&HCC
🔹 No approved Rx – 🎯 lifestyle, ⤵️weight & multi-specialty care
🔸 Future hope: GLP-1s, PPAR, THR-β agonists
👉 Access the full paper via link
🔗 ggdocs.co/dz0kai



February 27, 2025 at 3:00 PM
MASLD: ‘Elephant in the Room’ of #CKM
🔹 🌍 crisis: 1/3 adults affected, 65% in #T2D
🔸 Liver fibrosis=predictor of ☠️ & #CVD, #CKD,&HCC
🔹 No approved Rx – 🎯 lifestyle, ⤵️weight & multi-specialty care
🔸 Future hope: GLP-1s, PPAR, THR-β agonists
👉 Access the full paper via link
🔗 ggdocs.co/dz0kai
🔹 🌍 crisis: 1/3 adults affected, 65% in #T2D
🔸 Liver fibrosis=predictor of ☠️ & #CVD, #CKD,&HCC
🔹 No approved Rx – 🎯 lifestyle, ⤵️weight & multi-specialty care
🔸 Future hope: GLP-1s, PPAR, THR-β agonists
👉 Access the full paper via link
🔗 ggdocs.co/dz0kai
📢 Beyond GLP-1: The next wave ...
🔹 GIP/GLP-1 dual agonists (e.g., #Tirzepatide) ⤴️ wt loss vs. GLP-1
🔸 3x agonists (GIP/GLP-1/Glucagon) aim for >25% wt loss
🔹 Emerging 💉💊: Amylin + GLP-1 combos, FGF21 analogs, oral non-peptides
👉 Will the next-gen 💉 ⤴️ wt loss beyond 30%❓
🔗 ggdocs.co/hefyaj
🔹 GIP/GLP-1 dual agonists (e.g., #Tirzepatide) ⤴️ wt loss vs. GLP-1
🔸 3x agonists (GIP/GLP-1/Glucagon) aim for >25% wt loss
🔹 Emerging 💉💊: Amylin + GLP-1 combos, FGF21 analogs, oral non-peptides
👉 Will the next-gen 💉 ⤴️ wt loss beyond 30%❓
🔗 ggdocs.co/hefyaj

February 24, 2025 at 4:30 PM
📢 Beyond GLP-1: The next wave ...
🔹 GIP/GLP-1 dual agonists (e.g., #Tirzepatide) ⤴️ wt loss vs. GLP-1
🔸 3x agonists (GIP/GLP-1/Glucagon) aim for >25% wt loss
🔹 Emerging 💉💊: Amylin + GLP-1 combos, FGF21 analogs, oral non-peptides
👉 Will the next-gen 💉 ⤴️ wt loss beyond 30%❓
🔗 ggdocs.co/hefyaj
🔹 GIP/GLP-1 dual agonists (e.g., #Tirzepatide) ⤴️ wt loss vs. GLP-1
🔸 3x agonists (GIP/GLP-1/Glucagon) aim for >25% wt loss
🔹 Emerging 💉💊: Amylin + GLP-1 combos, FGF21 analogs, oral non-peptides
👉 Will the next-gen 💉 ⤴️ wt loss beyond 30%❓
🔗 ggdocs.co/hefyaj
Can resistance exercise reverse frailty in #T2D ❓
🔹 Frailty ⤵️ in 36% of intervention group vs. 17% usual care (OR 2.6, p=0.009)
🔸 SPPB ⤴️ by 1+ point in 47.8% vs. 35.3% (p=0.034)
🔹 Early intervention key❗️
👉 Time to rethink exercise as standard Rx for frailty in #T2D
🔗 ggdocs.co/zvm0cn
🔹 Frailty ⤵️ in 36% of intervention group vs. 17% usual care (OR 2.6, p=0.009)
🔸 SPPB ⤴️ by 1+ point in 47.8% vs. 35.3% (p=0.034)
🔹 Early intervention key❗️
👉 Time to rethink exercise as standard Rx for frailty in #T2D
🔗 ggdocs.co/zvm0cn


February 23, 2025 at 12:01 PM
Can resistance exercise reverse frailty in #T2D ❓
🔹 Frailty ⤵️ in 36% of intervention group vs. 17% usual care (OR 2.6, p=0.009)
🔸 SPPB ⤴️ by 1+ point in 47.8% vs. 35.3% (p=0.034)
🔹 Early intervention key❗️
👉 Time to rethink exercise as standard Rx for frailty in #T2D
🔗 ggdocs.co/zvm0cn
🔹 Frailty ⤵️ in 36% of intervention group vs. 17% usual care (OR 2.6, p=0.009)
🔸 SPPB ⤴️ by 1+ point in 47.8% vs. 35.3% (p=0.034)
🔹 Early intervention key❗️
👉 Time to rethink exercise as standard Rx for frailty in #T2D
🔗 ggdocs.co/zvm0cn
📢 Cardiac, Renal & Metabolic (CRM) Overlap: A Public Health Crisis?
🔹 CRM multimorbidity ⤴️ in 20 yrs (1 CRM: 21% → 26%, all 3: 0.7% → 1.5%)
🔸 ⚫️ & low SES = ⤴️ risk but ⤵️treatment❗️
🔹 Statins underused in 1/3 CRM pts, ACEi/ARB in 40-50%, SGLT2i/GLP1 <5%
👉 MDT + 🎯 therapy= key❗️
🔗 ggdocs.co/enhs7v
🔹 CRM multimorbidity ⤴️ in 20 yrs (1 CRM: 21% → 26%, all 3: 0.7% → 1.5%)
🔸 ⚫️ & low SES = ⤴️ risk but ⤵️treatment❗️
🔹 Statins underused in 1/3 CRM pts, ACEi/ARB in 40-50%, SGLT2i/GLP1 <5%
👉 MDT + 🎯 therapy= key❗️
🔗 ggdocs.co/enhs7v

February 21, 2025 at 12:05 PM
📢 Cardiac, Renal & Metabolic (CRM) Overlap: A Public Health Crisis?
🔹 CRM multimorbidity ⤴️ in 20 yrs (1 CRM: 21% → 26%, all 3: 0.7% → 1.5%)
🔸 ⚫️ & low SES = ⤴️ risk but ⤵️treatment❗️
🔹 Statins underused in 1/3 CRM pts, ACEi/ARB in 40-50%, SGLT2i/GLP1 <5%
👉 MDT + 🎯 therapy= key❗️
🔗 ggdocs.co/enhs7v
🔹 CRM multimorbidity ⤴️ in 20 yrs (1 CRM: 21% → 26%, all 3: 0.7% → 1.5%)
🔸 ⚫️ & low SES = ⤴️ risk but ⤵️treatment❗️
🔹 Statins underused in 1/3 CRM pts, ACEi/ARB in 40-50%, SGLT2i/GLP1 <5%
👉 MDT + 🎯 therapy= key❗️
🔗 ggdocs.co/enhs7v
Real-world tirzepatide use in #T2D in 🇺🇸
🔹 Initiation: 84% start at ≤5 mg, 69.6% ⤴️ dose within 6m
🔸 Dosing at 6m: 56.5% remain <10 mg
🔹 Persistence: 73.3% still on treatment at 6m
🔸 Discontinuation: 26.7% stopped, 29.1% restarted
👉 Persistence high, slower titration the norm
🔗 ggdocs.co/0z0q43
🔹 Initiation: 84% start at ≤5 mg, 69.6% ⤴️ dose within 6m
🔸 Dosing at 6m: 56.5% remain <10 mg
🔹 Persistence: 73.3% still on treatment at 6m
🔸 Discontinuation: 26.7% stopped, 29.1% restarted
👉 Persistence high, slower titration the norm
🔗 ggdocs.co/0z0q43

February 5, 2025 at 4:51 PM
Real-world tirzepatide use in #T2D in 🇺🇸
🔹 Initiation: 84% start at ≤5 mg, 69.6% ⤴️ dose within 6m
🔸 Dosing at 6m: 56.5% remain <10 mg
🔹 Persistence: 73.3% still on treatment at 6m
🔸 Discontinuation: 26.7% stopped, 29.1% restarted
👉 Persistence high, slower titration the norm
🔗 ggdocs.co/0z0q43
🔹 Initiation: 84% start at ≤5 mg, 69.6% ⤴️ dose within 6m
🔸 Dosing at 6m: 56.5% remain <10 mg
🔹 Persistence: 73.3% still on treatment at 6m
🔸 Discontinuation: 26.7% stopped, 29.1% restarted
👉 Persistence high, slower titration the norm
🔗 ggdocs.co/0z0q43
📢 #GLP1 in overweight/obesity—who stops & who restarts?
🔹 1-year disc.: #T2D 46.5% ⤵️ vs. no T2D 64.8% ⤴️
🔸 1-year reinitiation: #T2D 47.3% ⤴️ vs. no T2D 36.3% ⤵️
🔹 ⤴️Wt loss ⤵️disc. risk
🔸 GI AEs ⤴️ disc. risk (HR 1.38 in T2D, 1.19 no T2D)
👉 💰& 🤢 drive inequities in long-term❗️
🔗 ggdocs.co/456b83
🔹 1-year disc.: #T2D 46.5% ⤵️ vs. no T2D 64.8% ⤴️
🔸 1-year reinitiation: #T2D 47.3% ⤴️ vs. no T2D 36.3% ⤵️
🔹 ⤴️Wt loss ⤵️disc. risk
🔸 GI AEs ⤴️ disc. risk (HR 1.38 in T2D, 1.19 no T2D)
👉 💰& 🤢 drive inequities in long-term❗️
🔗 ggdocs.co/456b83



February 3, 2025 at 12:03 PM
📢 #GLP1 in overweight/obesity—who stops & who restarts?
🔹 1-year disc.: #T2D 46.5% ⤵️ vs. no T2D 64.8% ⤴️
🔸 1-year reinitiation: #T2D 47.3% ⤴️ vs. no T2D 36.3% ⤵️
🔹 ⤴️Wt loss ⤵️disc. risk
🔸 GI AEs ⤴️ disc. risk (HR 1.38 in T2D, 1.19 no T2D)
👉 💰& 🤢 drive inequities in long-term❗️
🔗 ggdocs.co/456b83
🔹 1-year disc.: #T2D 46.5% ⤵️ vs. no T2D 64.8% ⤴️
🔸 1-year reinitiation: #T2D 47.3% ⤴️ vs. no T2D 36.3% ⤵️
🔹 ⤴️Wt loss ⤵️disc. risk
🔸 GI AEs ⤴️ disc. risk (HR 1.38 in T2D, 1.19 no T2D)
👉 💰& 🤢 drive inequities in long-term❗️
🔗 ggdocs.co/456b83
EASO 🔥 Critiques Lancet’s #Obesity Framework 🇪🇺
🔹“Preclinical obesity” = delayed care 🚨
🔸Ignores T2D evidence (treatment ⤵️ complications)
🔹Flawed metrics: BMI focus ❌, misses root causes
👉 EASO’s fix:
✅ Early intervention
✅ WtHR + biology
✅ Equity > BMI
🔗 ggdocs.co/u5d8il
🔹“Preclinical obesity” = delayed care 🚨
🔸Ignores T2D evidence (treatment ⤵️ complications)
🔹Flawed metrics: BMI focus ❌, misses root causes
👉 EASO’s fix:
✅ Early intervention
✅ WtHR + biology
✅ Equity > BMI
🔗 ggdocs.co/u5d8il

January 26, 2025 at 11:03 AM
EASO 🔥 Critiques Lancet’s #Obesity Framework 🇪🇺
🔹“Preclinical obesity” = delayed care 🚨
🔸Ignores T2D evidence (treatment ⤵️ complications)
🔹Flawed metrics: BMI focus ❌, misses root causes
👉 EASO’s fix:
✅ Early intervention
✅ WtHR + biology
✅ Equity > BMI
🔗 ggdocs.co/u5d8il
🔹“Preclinical obesity” = delayed care 🚨
🔸Ignores T2D evidence (treatment ⤵️ complications)
🔹Flawed metrics: BMI focus ❌, misses root causes
👉 EASO’s fix:
✅ Early intervention
✅ WtHR + biology
✅ Equity > BMI
🔗 ggdocs.co/u5d8il
Finerenone in HFpEF/HFmrEF ❗️
🔹 Early eGFR declines (≥15%) with finerenone are common (23% vs. 13% placebo).
🔸 Unlike placebo, these declines were not associated with worse outcomes.
🔹 Finerenone ⤵️ 💔 & CV ☠️across eGFR changes.
❗️Don’t stop finerenone due to early eGFR dips❗️
🔗 ggdocs.co/3w7mim
🔹 Early eGFR declines (≥15%) with finerenone are common (23% vs. 13% placebo).
🔸 Unlike placebo, these declines were not associated with worse outcomes.
🔹 Finerenone ⤵️ 💔 & CV ☠️across eGFR changes.
❗️Don’t stop finerenone due to early eGFR dips❗️
🔗 ggdocs.co/3w7mim

January 25, 2025 at 8:05 AM
Finerenone in HFpEF/HFmrEF ❗️
🔹 Early eGFR declines (≥15%) with finerenone are common (23% vs. 13% placebo).
🔸 Unlike placebo, these declines were not associated with worse outcomes.
🔹 Finerenone ⤵️ 💔 & CV ☠️across eGFR changes.
❗️Don’t stop finerenone due to early eGFR dips❗️
🔗 ggdocs.co/3w7mim
🔹 Early eGFR declines (≥15%) with finerenone are common (23% vs. 13% placebo).
🔸 Unlike placebo, these declines were not associated with worse outcomes.
🔹 Finerenone ⤵️ 💔 & CV ☠️across eGFR changes.
❗️Don’t stop finerenone due to early eGFR dips❗️
🔗 ggdocs.co/3w7mim
Finerenone: Do we need another treatment for #CKD in #T2D ❓
🔹 Reduces CKD progression by 23% & CV events by 14% (FIDELITY analysis).
🔸 Complements RASi & SGLT2i therapies, offering comprehensive cardio-renal protection.
❗️A new pillar in T2D & CKD Mx #CombinationTherapy.
🔗 ggdocs.co/nqip3c
🔹 Reduces CKD progression by 23% & CV events by 14% (FIDELITY analysis).
🔸 Complements RASi & SGLT2i therapies, offering comprehensive cardio-renal protection.
❗️A new pillar in T2D & CKD Mx #CombinationTherapy.
🔗 ggdocs.co/nqip3c

January 21, 2025 at 3:00 PM
Finerenone: Do we need another treatment for #CKD in #T2D ❓
🔹 Reduces CKD progression by 23% & CV events by 14% (FIDELITY analysis).
🔸 Complements RASi & SGLT2i therapies, offering comprehensive cardio-renal protection.
❗️A new pillar in T2D & CKD Mx #CombinationTherapy.
🔗 ggdocs.co/nqip3c
🔹 Reduces CKD progression by 23% & CV events by 14% (FIDELITY analysis).
🔸 Complements RASi & SGLT2i therapies, offering comprehensive cardio-renal protection.
❗️A new pillar in T2D & CKD Mx #CombinationTherapy.
🔗 ggdocs.co/nqip3c
Does remission of #T2D matter❓
🔹 Study: GPs & nurses view remission as a motivational tool but not a clinical priority.
🔸 Concerns: transient nature of remission, coding reluctance, and risk of health inequities.
🔹 Need: Clearer guidance & resources for follow-up care.
🔗 ggdocs.co/isz5cs
🔹 Study: GPs & nurses view remission as a motivational tool but not a clinical priority.
🔸 Concerns: transient nature of remission, coding reluctance, and risk of health inequities.
🔹 Need: Clearer guidance & resources for follow-up care.
🔗 ggdocs.co/isz5cs

January 19, 2025 at 6:48 PM
Does remission of #T2D matter❓
🔹 Study: GPs & nurses view remission as a motivational tool but not a clinical priority.
🔸 Concerns: transient nature of remission, coding reluctance, and risk of health inequities.
🔹 Need: Clearer guidance & resources for follow-up care.
🔗 ggdocs.co/isz5cs
🔹 Study: GPs & nurses view remission as a motivational tool but not a clinical priority.
🔸 Concerns: transient nature of remission, coding reluctance, and risk of health inequities.
🔹 Need: Clearer guidance & resources for follow-up care.
🔗 ggdocs.co/isz5cs
Statin use ⤵️ insulin sensitivity & beta-cell function over 9 years❗️
🔹 9y PROMISE cohort study
🔸⤵️ insulin sensitivity 6%
🔹 ⤵️ beta-cell function 5-8%
🔸Greater effects in females
👉 consider when making informed decisions
🔗 ggdocs.co/isz5cs
@pharmrj.pharmsky.app @hpillminster.pharmsky.app
🔹 9y PROMISE cohort study
🔸⤵️ insulin sensitivity 6%
🔹 ⤵️ beta-cell function 5-8%
🔸Greater effects in females
👉 consider when making informed decisions
🔗 ggdocs.co/isz5cs
@pharmrj.pharmsky.app @hpillminster.pharmsky.app


January 19, 2025 at 10:44 AM
Statin use ⤵️ insulin sensitivity & beta-cell function over 9 years❗️
🔹 9y PROMISE cohort study
🔸⤵️ insulin sensitivity 6%
🔹 ⤵️ beta-cell function 5-8%
🔸Greater effects in females
👉 consider when making informed decisions
🔗 ggdocs.co/isz5cs
@pharmrj.pharmsky.app @hpillminster.pharmsky.app
🔹 9y PROMISE cohort study
🔸⤵️ insulin sensitivity 6%
🔹 ⤵️ beta-cell function 5-8%
🔸Greater effects in females
👉 consider when making informed decisions
🔗 ggdocs.co/isz5cs
@pharmrj.pharmsky.app @hpillminster.pharmsky.app
Peri-operative management of GLP-1 RAs & SGLT2 inhibitors❗️
🔹 New 🇬🇧 consensus: GLP-1 RAs can continue, but risks of aspiration must be assessed.
🔸SGLT2i should be stopped 1 day pre-op to avoid euglycemic DKA.
❗️shared decision-making & tailored approaches to optimise safety.
🔗 ggdocs.co/4r995z
🔹 New 🇬🇧 consensus: GLP-1 RAs can continue, but risks of aspiration must be assessed.
🔸SGLT2i should be stopped 1 day pre-op to avoid euglycemic DKA.
❗️shared decision-making & tailored approaches to optimise safety.
🔗 ggdocs.co/4r995z

January 18, 2025 at 2:30 PM
Peri-operative management of GLP-1 RAs & SGLT2 inhibitors❗️
🔹 New 🇬🇧 consensus: GLP-1 RAs can continue, but risks of aspiration must be assessed.
🔸SGLT2i should be stopped 1 day pre-op to avoid euglycemic DKA.
❗️shared decision-making & tailored approaches to optimise safety.
🔗 ggdocs.co/4r995z
🔹 New 🇬🇧 consensus: GLP-1 RAs can continue, but risks of aspiration must be assessed.
🔸SGLT2i should be stopped 1 day pre-op to avoid euglycemic DKA.
❗️shared decision-making & tailored approaches to optimise safety.
🔗 ggdocs.co/4r995z
Statins ⤵️ CVD risk & cost-effectively improve QALYs in older adults❗️
🔹 UK study: Statins ⤵️ CVD events by ~24% & CV deaths by ~12%.
🔸Cost-effective for those ≥70 years, regardless of LDL levels or prior CVD.
❗️statins important in preventive care for aging populations.
🔗 ggdocs.co/zcu36j
🔹 UK study: Statins ⤵️ CVD events by ~24% & CV deaths by ~12%.
🔸Cost-effective for those ≥70 years, regardless of LDL levels or prior CVD.
❗️statins important in preventive care for aging populations.
🔗 ggdocs.co/zcu36j

January 17, 2025 at 12:19 PM
Statins ⤵️ CVD risk & cost-effectively improve QALYs in older adults❗️
🔹 UK study: Statins ⤵️ CVD events by ~24% & CV deaths by ~12%.
🔸Cost-effective for those ≥70 years, regardless of LDL levels or prior CVD.
❗️statins important in preventive care for aging populations.
🔗 ggdocs.co/zcu36j
🔹 UK study: Statins ⤵️ CVD events by ~24% & CV deaths by ~12%.
🔸Cost-effective for those ≥70 years, regardless of LDL levels or prior CVD.
❗️statins important in preventive care for aging populations.
🔗 ggdocs.co/zcu36j
Microdosing semaglutide ⤵️ GI side effects etc...
🔹 Tailored dosing via multidose pens allows for gradual escalation to improve tolerability.
🔸 Useful in acute care settings or for cost-saving
👉Off-label but a promising option in specific clinical scenarios.
#Diabetes #GLP1
🔗 ggdocs.co/nwlkyc
🔹 Tailored dosing via multidose pens allows for gradual escalation to improve tolerability.
🔸 Useful in acute care settings or for cost-saving
👉Off-label but a promising option in specific clinical scenarios.
#Diabetes #GLP1
🔗 ggdocs.co/nwlkyc

January 16, 2025 at 10:36 AM
Microdosing semaglutide ⤵️ GI side effects etc...
🔹 Tailored dosing via multidose pens allows for gradual escalation to improve tolerability.
🔸 Useful in acute care settings or for cost-saving
👉Off-label but a promising option in specific clinical scenarios.
#Diabetes #GLP1
🔗 ggdocs.co/nwlkyc
🔹 Tailored dosing via multidose pens allows for gradual escalation to improve tolerability.
🔸 Useful in acute care settings or for cost-saving
👉Off-label but a promising option in specific clinical scenarios.
#Diabetes #GLP1
🔗 ggdocs.co/nwlkyc
SGLT-2 inhibitors ⤵️ cirrhosis risk in #T2D❗️
🔹 🇬🇧 cohort study: SGLT-2 inhibitors ⤵️cirrhosis incidence by 36% (HR 0.64) & decompensated cirrhosis by 26% (HR 0.74) vs. DPP-4i's.
🔹 No similar benefit seen with #GLP1
👉Highlights potential liver benefits of SGLT-2 inhibitors
🔗ggdocs.co/crpvon
🔹 🇬🇧 cohort study: SGLT-2 inhibitors ⤵️cirrhosis incidence by 36% (HR 0.64) & decompensated cirrhosis by 26% (HR 0.74) vs. DPP-4i's.
🔹 No similar benefit seen with #GLP1
👉Highlights potential liver benefits of SGLT-2 inhibitors
🔗ggdocs.co/crpvon

January 13, 2025 at 7:10 PM