



@elvinwag.bsky.social
Interesting thought!
April 9, 2025 at 12:59 AM
Interesting thought!
Thank you to all the contributors in the Wagenblast lab (especially Ke Wang, Shayan Saniei and Nikita Poddar), all our collaborators and funding mechanisms. @eirinipapapetrou.bsky.social
April 8, 2025 at 2:32 PM
Thank you to all the contributors in the Wagenblast lab (especially Ke Wang, Shayan Saniei and Nikita Poddar), all our collaborators and funding mechanisms. @eirinipapapetrou.bsky.social
Key takeaway: WHEN mutations arise profoundly impacts leukemia aggressiveness & treatment responses. Targeting fetal-specific vulnerabilities holds exciting potential for pediatric AML. Read the full pre-print here: www.biorxiv.org/content/10.1... 13/13

Ontogeny Dictates Oncogenic Potential, Lineage Hierarchy, and Therapy Response in Pediatric Leukemia
Accumulating evidence links pediatric cancers to prenatal transformation events, yet the influence of the developmental stage on oncogenesis remains elusive. We investigated how hematopoietic stem cel...
www.biorxiv.org
April 8, 2025 at 2:32 PM
Key takeaway: WHEN mutations arise profoundly impacts leukemia aggressiveness & treatment responses. Targeting fetal-specific vulnerabilities holds exciting potential for pediatric AML. Read the full pre-print here: www.biorxiv.org/content/10.1... 13/13
Leveraging fetal NUP98::NSD1’s reliance on BCL2 & oxidative phosphorylation, we tested Venetoclax combinations (with Ara-C or Revumenib). Result: dramatically reduced leukemia in mice. Could this combo redefine pediatric AML therapy? 12/13

April 8, 2025 at 2:32 PM
Leveraging fetal NUP98::NSD1’s reliance on BCL2 & oxidative phosphorylation, we tested Venetoclax combinations (with Ara-C or Revumenib). Result: dramatically reduced leukemia in mice. Could this combo redefine pediatric AML therapy? 12/13
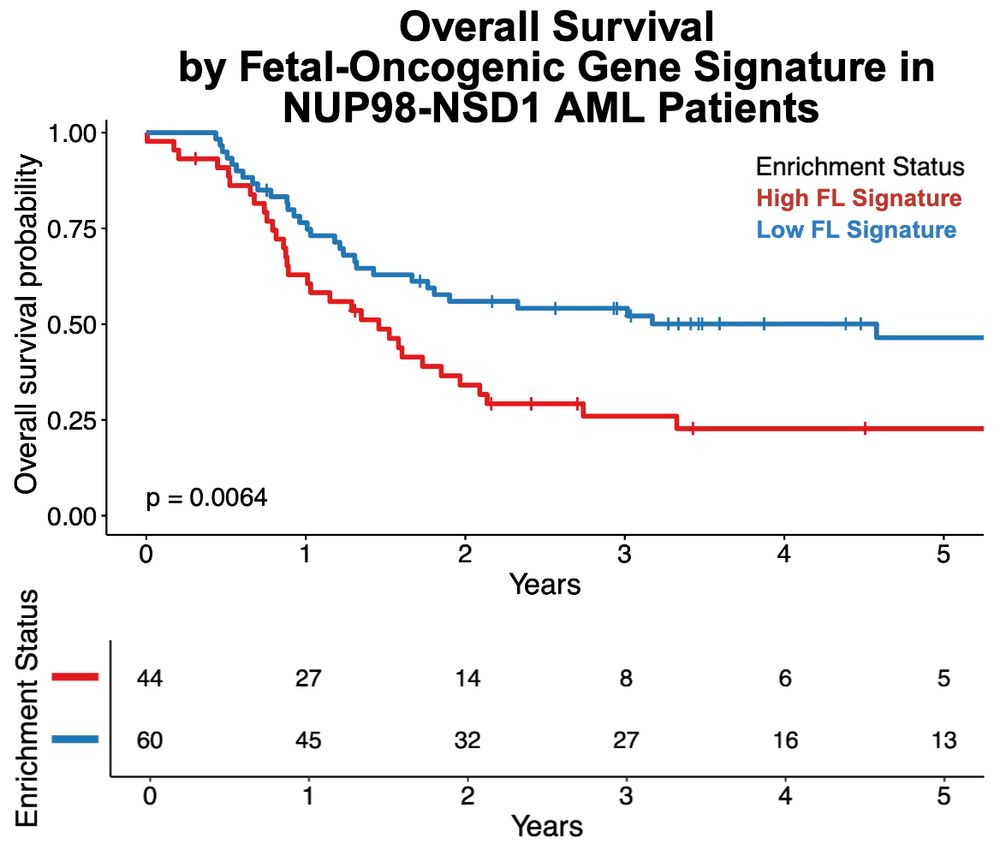
Clinically, pediatric AML patients with our fetal-oncogenic signatures had significantly worse outcomes. This signature could help identify high-risk patients, highlighting opportunities to personalize therapies early. 11/13
April 8, 2025 at 2:32 PM
Clinically, pediatric AML patients with our fetal-oncogenic signatures had significantly worse outcomes. This signature could help identify high-risk patients, highlighting opportunities to personalize therapies early. 11/13
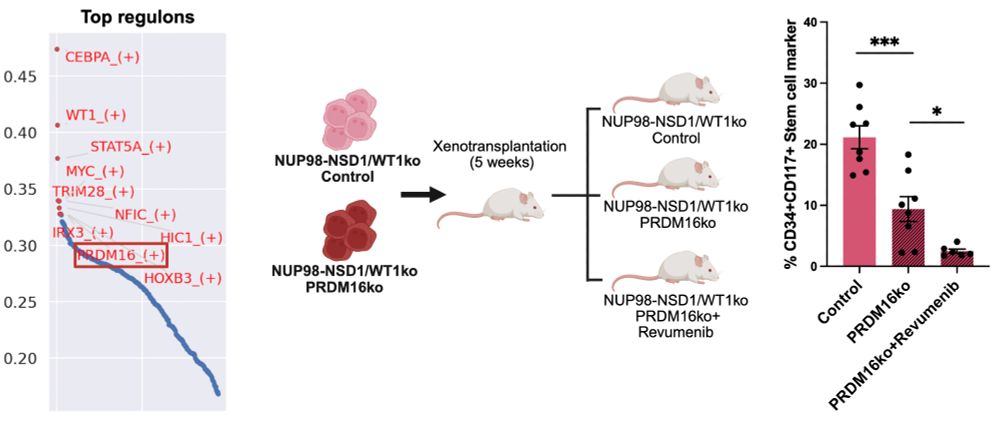
PRDM16 emerged as a master regulator in fetal-origin NUP98::NSD1 AML. Knocking out PRDM16 halted leukemia growth and overcame therapy resistance, spotlighting PRDM16 as an exciting therapeutic target. 10/13
April 8, 2025 at 2:32 PM
PRDM16 emerged as a master regulator in fetal-origin NUP98::NSD1 AML. Knocking out PRDM16 halted leukemia growth and overcame therapy resistance, spotlighting PRDM16 as an exciting therapeutic target. 10/13
Fetal-origin leukemia stem cells uniquely rely on oxidative phosphorylation & fatty acid oxidation, driven by the transcription factor PRDM16. PRDM16 also enhances anti-apoptotic BCL2, creating powerful therapy resistance. 9/13

April 8, 2025 at 2:32 PM
Fetal-origin leukemia stem cells uniquely rely on oxidative phosphorylation & fatty acid oxidation, driven by the transcription factor PRDM16. PRDM16 also enhances anti-apoptotic BCL2, creating powerful therapy resistance. 9/13
Leukemias responded differently to chemotherapy (Ara-C) & menin inhibition (Revumenib) based on developmental origin. Postnatal cord blood-derived AML responded better to Revumenib; fetal-origin AML was more resistant. Why this difference? 8/13

April 8, 2025 at 2:32 PM
Leukemias responded differently to chemotherapy (Ara-C) & menin inhibition (Revumenib) based on developmental origin. Postnatal cord blood-derived AML responded better to Revumenib; fetal-origin AML was more resistant. Why this difference? 8/13
Indeed, fetal-origin LMPP/early GMP cells were highly enriched for the leukemia stem and progenitor (LSPC) QUIESCENT signature, while cord blood-derived AML was enriched for the LSPC CYCLING signature. 7/13

April 8, 2025 at 2:32 PM
Indeed, fetal-origin LMPP/early GMP cells were highly enriched for the leukemia stem and progenitor (LSPC) QUIESCENT signature, while cord blood-derived AML was enriched for the LSPC CYCLING signature. 7/13
Single-cell RNA & chromatin accessibility profiling revealed WT1 loss expands early progenitors (LMPP/early GMP), enriched for quiescence (high EGR1) & high MYC expression. Could this explain increased leukemia aggressiveness? 6/13

April 8, 2025 at 2:32 PM
Single-cell RNA & chromatin accessibility profiling revealed WT1 loss expands early progenitors (LMPP/early GMP), enriched for quiescence (high EGR1) & high MYC expression. Could this explain increased leukemia aggressiveness? 6/13
In mice, these engineered cells formed aggressive AML. Adding WT1 loss-of-function intensified disease severity, boosting leukemia stem cell traits and therapy resistance. WT1 loss marks exceptionally aggressive AML subsets. 5/13

April 8, 2025 at 2:32 PM
In mice, these engineered cells formed aggressive AML. Adding WT1 loss-of-function intensified disease severity, boosting leukemia stem cell traits and therapy resistance. WT1 loss marks exceptionally aggressive AML subsets. 5/13
With GoT-ChA (single-cell ATAC-seq + genotyping), fetal-derived NUP98::NSD1 cells revealed strong enrichment for HOX genes, MLL, & STAT pathways. But how does this epigenetic and transcriptional state behave in vivo? Let's transplant and see! 4/13

April 8, 2025 at 2:32 PM
With GoT-ChA (single-cell ATAC-seq + genotyping), fetal-derived NUP98::NSD1 cells revealed strong enrichment for HOX genes, MLL, & STAT pathways. But how does this epigenetic and transcriptional state behave in vivo? Let's transplant and see! 4/13
We engineered NUP98::NSD1 fusion using CRISPR/Cas9 in human blood stem cells. Fetal-derived cells rapidly became leukemic; postnatal cells less so; pediatric/adult cells showed resistance. Why are fetal cells uniquely vulnerable to leukemia initiation? 3/13

April 8, 2025 at 2:32 PM
We engineered NUP98::NSD1 fusion using CRISPR/Cas9 in human blood stem cells. Fetal-derived cells rapidly became leukemic; postnatal cells less so; pediatric/adult cells showed resistance. Why are fetal cells uniquely vulnerable to leukemia initiation? 3/13
NUP98-rearranged AML in children is aggressive with poor survival. Using human stem cells across fetal, postnatal, pediatric, & adult stages, we found leukemia initiation strongly depends on developmental timing – it's all about WHEN mutations arise. 2/13

April 8, 2025 at 2:32 PM
NUP98-rearranged AML in children is aggressive with poor survival. Using human stem cells across fetal, postnatal, pediatric, & adult stages, we found leukemia initiation strongly depends on developmental timing – it's all about WHEN mutations arise. 2/13