


Matt Luther, MD MSCI
@drjmluther.bsky.social
Nephrologist, Hypertension specialist, Physician-scientist.
Yes, MRAs can cause mild hyponatremia. Usually not a major issue but can be a factor. I have not seen severe hyponatremia (eg <125) and use a lot.
Aldosterone deficient mice are mildly hyponatremic (inconsistently)
Primary aldosteronism is associated with mild hypernatremia
Aldosterone deficient mice are mildly hyponatremic (inconsistently)
Primary aldosteronism is associated with mild hypernatremia
October 16, 2025 at 5:54 PM
Yes, MRAs can cause mild hyponatremia. Usually not a major issue but can be a factor. I have not seen severe hyponatremia (eg <125) and use a lot.
Aldosterone deficient mice are mildly hyponatremic (inconsistently)
Primary aldosteronism is associated with mild hypernatremia
Aldosterone deficient mice are mildly hyponatremic (inconsistently)
Primary aldosteronism is associated with mild hypernatremia
Tolerate if really needed, but taper as BP falls after spironolactone takes effect- usually weeks to 3 months
September 28, 2025 at 4:37 AM
Tolerate if really needed, but taper as BP falls after spironolactone takes effect- usually weeks to 3 months
42% sensitivity is what you want in a screening test, right? [sarcasm]
September 24, 2025 at 3:03 PM
42% sensitivity is what you want in a screening test, right? [sarcasm]
almost always lower dose 12.5-25, occasionally higher 50-100mg.
hyperkalemia/CKD > gynecomastia > dysmenorrhea of course can be limiting
hyperkalemia/CKD > gynecomastia > dysmenorrhea of course can be limiting
July 15, 2025 at 4:45 PM
almost always lower dose 12.5-25, occasionally higher 50-100mg.
hyperkalemia/CKD > gynecomastia > dysmenorrhea of course can be limiting
hyperkalemia/CKD > gynecomastia > dysmenorrhea of course can be limiting
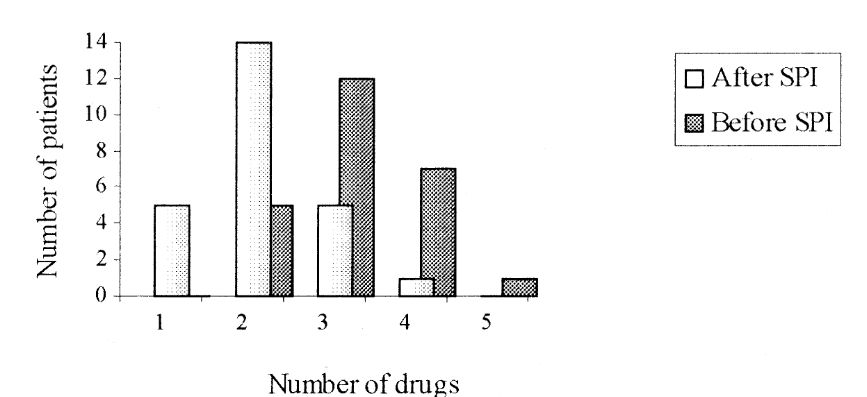
Yes you should be able to reduce medications after adding Spironolactone.
I withdraw based on other adverse med effects (edema = CCB; K = thiazide/RAASi)
I use this figure in my talks on Resistant HTN...(observational, but holds up imo)
pubmed.ncbi.nlm.nih.gov/11991219/
I withdraw based on other adverse med effects (edema = CCB; K = thiazide/RAASi)
I use this figure in my talks on Resistant HTN...(observational, but holds up imo)
pubmed.ncbi.nlm.nih.gov/11991219/
July 15, 2025 at 4:16 PM
Yes you should be able to reduce medications after adding Spironolactone.
I withdraw based on other adverse med effects (edema = CCB; K = thiazide/RAASi)
I use this figure in my talks on Resistant HTN...(observational, but holds up imo)
pubmed.ncbi.nlm.nih.gov/11991219/
I withdraw based on other adverse med effects (edema = CCB; K = thiazide/RAASi)
I use this figure in my talks on Resistant HTN...(observational, but holds up imo)
pubmed.ncbi.nlm.nih.gov/11991219/
Bring back methyldopa too!
May 30, 2025 at 2:41 AM
Bring back methyldopa too!
Standardized treatment in advance-HTN included thiazide + ARB for all.
Upcoming Launch-HTN uses standard background meds so will be a mix of real world regimens.
Longer term open label followup is ongoing too.
Upcoming Launch-HTN uses standard background meds so will be a mix of real world regimens.
Longer term open label followup is ongoing too.
May 30, 2025 at 2:40 AM
Standardized treatment in advance-HTN included thiazide + ARB for all.
Upcoming Launch-HTN uses standard background meds so will be a mix of real world regimens.
Longer term open label followup is ongoing too.
Upcoming Launch-HTN uses standard background meds so will be a mix of real world regimens.
Longer term open label followup is ongoing too.
I'm gonna guess Geriatrics
May 29, 2025 at 9:06 PM
I'm gonna guess Geriatrics
Hyponatremia define here as <135, and also while all patients on a thiazide. Suspect clinically significant hypoNa is much less common.
#NephJC
#NephJC
May 28, 2025 at 5:40 PM
Hyponatremia define here as <135, and also while all patients on a thiazide. Suspect clinically significant hypoNa is much less common.
#NephJC
#NephJC
I do not have any inside info- doesn't look like it is being studied in the US, likely due to lack of patent protection. But it appears much less selective than newer agents. It is just R-fadrazole.
May 28, 2025 at 3:38 AM
I do not have any inside info- doesn't look like it is being studied in the US, likely due to lack of patent protection. But it appears much less selective than newer agents. It is just R-fadrazole.
the bigger issue is - don't block cortisol synthesis, which ramps up ACTH and revs up the steroid pathway and further augments DOC accumulation.
#NephJC
btw @kidneyboy.bsky.social this pathway needs to be taught to our Neph fellows so they can think this problem out like you're doing
#NephJC
btw @kidneyboy.bsky.social this pathway needs to be taught to our Neph fellows so they can think this problem out like you're doing
May 28, 2025 at 2:11 AM
the bigger issue is - don't block cortisol synthesis, which ramps up ACTH and revs up the steroid pathway and further augments DOC accumulation.
#NephJC
btw @kidneyboy.bsky.social this pathway needs to be taught to our Neph fellows so they can think this problem out like you're doing
#NephJC
btw @kidneyboy.bsky.social this pathway needs to be taught to our Neph fellows so they can think this problem out like you're doing
Indapamide 2.5mg or if previously on HCTZ continue that dose (if I recall correctly).
Plus Olmesartan 40mg in all.
If previously on 3 drugs then Amlodipine 10mg or max tolerated dose used.
#NephJC
Plus Olmesartan 40mg in all.
If previously on 3 drugs then Amlodipine 10mg or max tolerated dose used.
#NephJC
May 28, 2025 at 2:08 AM
Indapamide 2.5mg or if previously on HCTZ continue that dose (if I recall correctly).
Plus Olmesartan 40mg in all.
If previously on 3 drugs then Amlodipine 10mg or max tolerated dose used.
#NephJC
Plus Olmesartan 40mg in all.
If previously on 3 drugs then Amlodipine 10mg or max tolerated dose used.
#NephJC
Not sure the numbers are sig different, but I think your rationale is correct. The dose would have been pushed up to 100mg only in the most resistant #NephJC
May 28, 2025 at 1:57 AM
Not sure the numbers are sig different, but I think your rationale is correct. The dose would have been pushed up to 100mg only in the most resistant #NephJC
Theoretically:
- it targets the primary issue in many patients- unregulated aldosterone production.
-avoid effect of further elevated Aldo during MRA treatment
Obvs -avoid gynecomastia and off-target effects of Spiro.
For other MRAs it has always been difficult to push dose high enough.
#NephJC
- it targets the primary issue in many patients- unregulated aldosterone production.
-avoid effect of further elevated Aldo during MRA treatment
Obvs -avoid gynecomastia and off-target effects of Spiro.
For other MRAs it has always been difficult to push dose high enough.
#NephJC
May 28, 2025 at 1:54 AM
Theoretically:
- it targets the primary issue in many patients- unregulated aldosterone production.
-avoid effect of further elevated Aldo during MRA treatment
Obvs -avoid gynecomastia and off-target effects of Spiro.
For other MRAs it has always been difficult to push dose high enough.
#NephJC
- it targets the primary issue in many patients- unregulated aldosterone production.
-avoid effect of further elevated Aldo during MRA treatment
Obvs -avoid gynecomastia and off-target effects of Spiro.
For other MRAs it has always been difficult to push dose high enough.
#NephJC