



Abhinav Anand
@docabhinavheart.bsky.social
#cardiologist #electrophysiologist #Epeeps #cardiosky
Assistant Professor at @ ltmgh cardiology and @ Seth GSMC and Kem hospital, Mumbai
Assistant Professor at @ ltmgh cardiology and @ Seth GSMC and Kem hospital, Mumbai
Tagging the masters.. @narrowqrs.bsky.social @jeffreyvinocur.bsky.social @shah.md @prashsanders.bsky.social @jkhmd.bsky.social @epsri.bsky.social @wsauer.bsky.social @sivamulpurumd.bsky.social
March 30, 2025 at 6:15 AM
We hope that you enjoy reading this!!
March 30, 2025 at 6:04 AM
We hope that you enjoy reading this!!
Even though we ended up referencing Prof. Nagashima's another tour de force in the bibliography "SVT quest: The adventure diagnosing narrow QRS tachycardia" doi.org/10.1002/joa3... .
Both of these are excellent papers and should be read by everyone, I feel.
Both of these are excellent papers and should be read by everyone, I feel.
SVT quest: The adventure diagnosing narrow QRS tachycardia
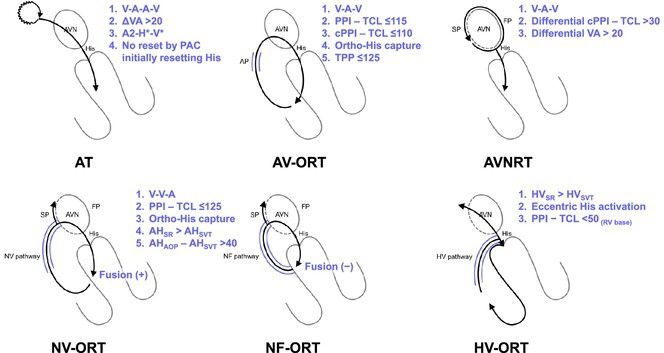
The SVT mechanism includes atrial tachycardia (AT), orthodromic reciprocating tachycardia (ORT) via an atrioventricular accessory pathway (AP), nodoventricular pathway (NVP), nodofascicular pathway (...
doi.org
March 30, 2025 at 6:04 AM
Even though we ended up referencing Prof. Nagashima's another tour de force in the bibliography "SVT quest: The adventure diagnosing narrow QRS tachycardia" doi.org/10.1002/joa3... .
Both of these are excellent papers and should be read by everyone, I feel.
Both of these are excellent papers and should be read by everyone, I feel.
This is an excellent paper for understanding antegrade His capture and it's difference from retrograde His capture.
March 30, 2025 at 6:04 AM
This is an excellent paper for understanding antegrade His capture and it's difference from retrograde His capture.
2. Novel Diagnostic Observations of Nodoventricular/Nodofascicular Pathway-Related Orthodromic Reciprocating Tachycardia Differentiating From Atrioventricular Nodal Re-Entrant Tachycardia by nagashima et al. (Doi: 10.1016/j.jacep.2020.07.007)
March 30, 2025 at 6:03 AM
2. Novel Diagnostic Observations of Nodoventricular/Nodofascicular Pathway-Related Orthodromic Reciprocating Tachycardia Differentiating From Atrioventricular Nodal Re-Entrant Tachycardia by nagashima et al. (Doi: 10.1016/j.jacep.2020.07.007)
The proximal pivot is same in both the tachycardias (av node : nh cells). How our case differed was because of the distal pivot proximal to the bifurcation of the bundle branches resulting in a narrow complex tachycardia. ( doi.org/10.1111/j.15...)
AV Nodal‐His‐Purkinje Reentry: A Novel Form of Tachycardia
AV Nodal-His-Purkinje Reentry. Introduction: Bundle branch reentry (BBR) typically occurs in patients with dilated cardiomyopathy and infra-Hisian conduction system disease. The macroreentrant circui...
doi.org
March 30, 2025 at 6:02 AM
The proximal pivot is same in both the tachycardias (av node : nh cells). How our case differed was because of the distal pivot proximal to the bifurcation of the bundle branches resulting in a narrow complex tachycardia. ( doi.org/10.1111/j.15...)
1. A novel form of tachycardia: av node - his purkinje reentry tachycardia by markowitz et al. in 1995.
March 30, 2025 at 6:02 AM
1. A novel form of tachycardia: av node - his purkinje reentry tachycardia by markowitz et al. in 1995.
Finally two papers that were indispensable to writing this report.
March 30, 2025 at 6:02 AM
Finally two papers that were indispensable to writing this report.
A lot of the egms had to be shifted to the supplementary material due to journal restrictions.
March 30, 2025 at 6:01 AM
A lot of the egms had to be shifted to the supplementary material due to journal restrictions.
We describe a case with longitudinal dissociation in the His bundle and how various maneuvers/ adenosine were used to make a diagnosis of av node-intrahisian reentry tachycardia.
March 30, 2025 at 6:01 AM
We describe a case with longitudinal dissociation in the His bundle and how various maneuvers/ adenosine were used to make a diagnosis of av node-intrahisian reentry tachycardia.
Looking forward to. Great tracing.
Thanks for posting. ❤️
Thanks for posting. ❤️
March 19, 2025 at 12:02 PM
Looking forward to. Great tracing.
Thanks for posting. ❤️
Thanks for posting. ❤️
Yes!!!
Was this patient taken for ep study?
Was this patient taken for ep study?
March 19, 2025 at 11:43 AM
Yes!!!
Was this patient taken for ep study?
Was this patient taken for ep study?
So... during the double fire, the slow pathway causes concealed conduction in the fast pathway leading to blocked p wave (yellow)?
March 19, 2025 at 11:38 AM
So... during the double fire, the slow pathway causes concealed conduction in the fast pathway leading to blocked p wave (yellow)?
SR, 1:1 avc
Pvc, parahisian(Narrow, 2,3 discordance)
PR suddenly prolongs. Likely due to a premature His complex causing concealed conduction and shift in the conduction from the fast to the slow pathway.
Conduction continues through the slow pathway due to retrograde fast pathway invasion.
Pvc, parahisian(Narrow, 2,3 discordance)
PR suddenly prolongs. Likely due to a premature His complex causing concealed conduction and shift in the conduction from the fast to the slow pathway.
Conduction continues through the slow pathway due to retrograde fast pathway invasion.
March 19, 2025 at 7:57 AM
SR, 1:1 avc
Pvc, parahisian(Narrow, 2,3 discordance)
PR suddenly prolongs. Likely due to a premature His complex causing concealed conduction and shift in the conduction from the fast to the slow pathway.
Conduction continues through the slow pathway due to retrograde fast pathway invasion.
Pvc, parahisian(Narrow, 2,3 discordance)
PR suddenly prolongs. Likely due to a premature His complex causing concealed conduction and shift in the conduction from the fast to the slow pathway.
Conduction continues through the slow pathway due to retrograde fast pathway invasion.
That being said.
A few q.
1. Did you map retrograde through the aorta at the ncc also?
2. What is the risk of pacemaker that you explained for this pt?
A few q.
1. Did you map retrograde through the aorta at the ncc also?
2. What is the risk of pacemaker that you explained for this pt?
December 20, 2024 at 4:15 PM
That being said.
A few q.
1. Did you map retrograde through the aorta at the ncc also?
2. What is the risk of pacemaker that you explained for this pt?
A few q.
1. Did you map retrograde through the aorta at the ncc also?
2. What is the risk of pacemaker that you explained for this pt?
Nice case!
I was thinking more lateral of the tricuspid annulus because of 2, 3 discordance. But just realised on reviewing the sinus ecg that the same discordance is present in the sinus rhythm as well.
I was thinking more lateral of the tricuspid annulus because of 2, 3 discordance. But just realised on reviewing the sinus ecg that the same discordance is present in the sinus rhythm as well.
December 20, 2024 at 4:13 PM
Nice case!
I was thinking more lateral of the tricuspid annulus because of 2, 3 discordance. But just realised on reviewing the sinus ecg that the same discordance is present in the sinus rhythm as well.
I was thinking more lateral of the tricuspid annulus because of 2, 3 discordance. But just realised on reviewing the sinus ecg that the same discordance is present in the sinus rhythm as well.
This is brilliant!
May I ask what is the software you use for making these?
May I ask what is the software you use for making these?
November 27, 2024 at 3:50 AM
This is brilliant!
May I ask what is the software you use for making these?
May I ask what is the software you use for making these?
Great case!
Thanks for sharing.
Thanks for sharing.
November 22, 2024 at 3:04 AM
Great case!
Thanks for sharing.
Thanks for sharing.
That being said.. most of the flecainide toxicity that I have seen have presented with qrs widening/ mmvt. So I may be biased that way.
Thank you for your comments.
Thank you for your comments.
November 21, 2024 at 2:22 PM
That being said.. most of the flecainide toxicity that I have seen have presented with qrs widening/ mmvt. So I may be biased that way.
Thank you for your comments.
Thank you for your comments.
This ecg has a few other differentials.
1.Hyperkalemia (addition of aldactone/aki)
2. Drug interaction causing increase in antiarrhythmic concentration.
3. Induction of epicardial vt due to biv pacing (less likely because of the spikes followed by qrs)
1.Hyperkalemia (addition of aldactone/aki)
2. Drug interaction causing increase in antiarrhythmic concentration.
3. Induction of epicardial vt due to biv pacing (less likely because of the spikes followed by qrs)
November 21, 2024 at 2:19 PM
This ecg has a few other differentials.
1.Hyperkalemia (addition of aldactone/aki)
2. Drug interaction causing increase in antiarrhythmic concentration.
3. Induction of epicardial vt due to biv pacing (less likely because of the spikes followed by qrs)
1.Hyperkalemia (addition of aldactone/aki)
2. Drug interaction causing increase in antiarrhythmic concentration.
3. Induction of epicardial vt due to biv pacing (less likely because of the spikes followed by qrs)
I think it's more appropriate to say that flecainide is contraindicated in patients with past mi rather than structural heart disease, since we have reports of the use of drugs in MVP with good results.
There's a spike followed by qrs, so this is still a paced rhythm rather than mmvt (1/2)
There's a spike followed by qrs, so this is still a paced rhythm rather than mmvt (1/2)
November 21, 2024 at 2:17 PM
I think it's more appropriate to say that flecainide is contraindicated in patients with past mi rather than structural heart disease, since we have reports of the use of drugs in MVP with good results.
There's a spike followed by qrs, so this is still a paced rhythm rather than mmvt (1/2)
There's a spike followed by qrs, so this is still a paced rhythm rather than mmvt (1/2)