




Christoffer Baustad Nilsen 🐈
@christofferbn.bsky.social
Sisyphus? Give the man a hoop and a winch! // Substack: https://christofferbn.substack.com
This was also published on Substack: christofferbn.substack.com/p/coronary-a...

Coronary Atherosclerosis in Metabolically Healthy Individuals with High LDL-C – Insights from the KETO-CTA Study
New from International Research: Coronary Atherosclerosis in Metabolically Healthy Individuals with High LDL-C – Insights from the KETO-CTA Study Abstract
christofferbn.substack.com
June 20, 2025 at 12:21 PM
This was also published on Substack: christofferbn.substack.com/p/coronary-a...
We wrote this critique to clarify the actual findings, correct misleading claims, and re-center the discussion on the data.
You can read our full article (in Norwegian) here: www.scup.com/doi/10.18261...
Or read it translated (Google translate): www-scup-com.translate.goog/doi/10.18261...
14/14
You can read our full article (in Norwegian) here: www.scup.com/doi/10.18261...
Or read it translated (Google translate): www-scup-com.translate.goog/doi/10.18261...
14/14

Nytt fra internasjonal forskning: Koronar aterosklerose hos metabolsk friske med høyt LDL-C – innsikt fra KETO-CTA-studien
Enkelte som følger et ketogent kosthold opplever dramatisk økning i LDL-kolesterolet
tross ellers god metabolsk helse, såkalte Lean Mass Hyper-Responders (LMHR). Bekymringen
har vært knyttet til om de...
www.scup.com
June 18, 2025 at 5:18 AM
We wrote this critique to clarify the actual findings, correct misleading claims, and re-center the discussion on the data.
You can read our full article (in Norwegian) here: www.scup.com/doi/10.18261...
Or read it translated (Google translate): www-scup-com.translate.goog/doi/10.18261...
14/14
You can read our full article (in Norwegian) here: www.scup.com/doi/10.18261...
Or read it translated (Google translate): www-scup-com.translate.goog/doi/10.18261...
14/14
Our takeaway is that the LMHR profile does not appear protective. Plaque grew fast—even with low inflammation, low TG, high HDL, and no metabolic syndrome.
13/14
13/14

June 18, 2025 at 5:18 AM
Our takeaway is that the LMHR profile does not appear protective. Plaque grew fast—even with low inflammation, low TG, high HDL, and no metabolic syndrome.
13/14
13/14
In short, the KETO-CTA study raises several ethical concerns:
🔹 The primary outcome was never reported
🔹 Median change was shared on Twitter, not in the paper
🔹 Focus shifted to post hoc analyses
🔹 The study is called a "trial"—but it’s not
12/14
🔹 The primary outcome was never reported
🔹 Median change was shared on Twitter, not in the paper
🔹 Focus shifted to post hoc analyses
🔹 The study is called a "trial"—but it’s not
12/14

June 18, 2025 at 5:18 AM
In short, the KETO-CTA study raises several ethical concerns:
🔹 The primary outcome was never reported
🔹 Median change was shared on Twitter, not in the paper
🔹 Focus shifted to post hoc analyses
🔹 The study is called a "trial"—but it’s not
12/14
🔹 The primary outcome was never reported
🔹 Median change was shared on Twitter, not in the paper
🔹 Focus shifted to post hoc analyses
🔹 The study is called a "trial"—but it’s not
12/14
Moreover, increases in PAV can’t simply be blamed on statins.
Statins shift plaque toward calcification—they don’t raise unstable plaque.
Yet LMHRs (on no meds) had a PAV increase of 0.8%.
That’s not a statin artifact.
11/14
Statins shift plaque toward calcification—they don’t raise unstable plaque.
Yet LMHRs (on no meds) had a PAV increase of 0.8%.
That’s not a statin artifact.
11/14

June 18, 2025 at 5:18 AM
Moreover, increases in PAV can’t simply be blamed on statins.
Statins shift plaque toward calcification—they don’t raise unstable plaque.
Yet LMHRs (on no meds) had a PAV increase of 0.8%.
That’s not a statin artifact.
11/14
Statins shift plaque toward calcification—they don’t raise unstable plaque.
Yet LMHRs (on no meds) had a PAV increase of 0.8%.
That’s not a statin artifact.
11/14
Some argue it’s unfair to compare LMHRs to high-risk groups—because those were often on statins. But LMHRs are often viewed as being “too healthy” to need meds.
10/14
10/14

June 18, 2025 at 5:18 AM
Some argue it’s unfair to compare LMHRs to high-risk groups—because those were often on statins. But LMHRs are often viewed as being “too healthy” to need meds.
10/14
10/14
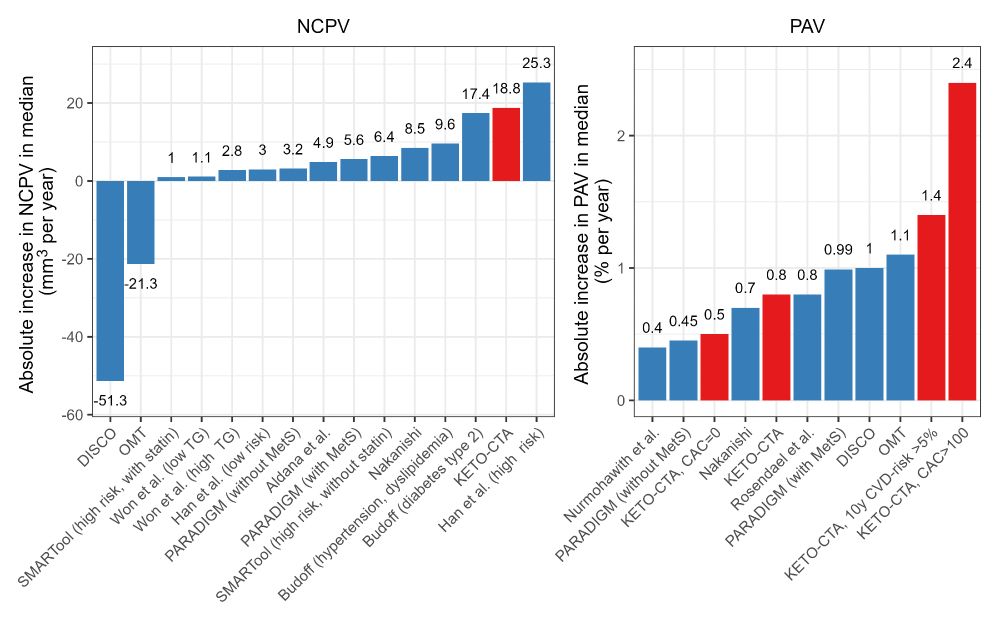
PAV (Percentage Atheroma Volume) also increased by 0.8%.
This is:
– Higher than in many statin-treated patients
– Double the increase seen in low-risk untreated cohorts
– Close to the 0.93% threshold for increased CV risk
9/14
This is:
– Higher than in many statin-treated patients
– Double the increase seen in low-risk untreated cohorts
– Close to the 0.93% threshold for increased CV risk
9/14
June 18, 2025 at 5:18 AM
PAV (Percentage Atheroma Volume) also increased by 0.8%.
This is:
– Higher than in many statin-treated patients
– Double the increase seen in low-risk untreated cohorts
– Close to the 0.93% threshold for increased CV risk
9/14
This is:
– Higher than in many statin-treated patients
– Double the increase seen in low-risk untreated cohorts
– Close to the 0.93% threshold for increased CV risk
9/14
We eventually got one of the missing numbers via social media: A median increase in NCPV of 18.8 mm³ (~44% increase).
This is as fast or faster than what we see in diabetic and/or high-risk groups. That's despite these participants being “metabolically perfect”!
8/14
This is as fast or faster than what we see in diabetic and/or high-risk groups. That's despite these participants being “metabolically perfect”!
8/14

June 18, 2025 at 5:18 AM
We eventually got one of the missing numbers via social media: A median increase in NCPV of 18.8 mm³ (~44% increase).
This is as fast or faster than what we see in diabetic and/or high-risk groups. That's despite these participants being “metabolically perfect”!
8/14
This is as fast or faster than what we see in diabetic and/or high-risk groups. That's despite these participants being “metabolically perfect”!
8/14
So what did the authors report instead? A post hoc analyses showing that ApoB did not correlate with plaque growth.
This is misuse of the data—and it's not acceptable in scientific publishing.
7/14
This is misuse of the data—and it's not acceptable in scientific publishing.
7/14

June 18, 2025 at 5:18 AM
So what did the authors report instead? A post hoc analyses showing that ApoB did not correlate with plaque growth.
This is misuse of the data—and it's not acceptable in scientific publishing.
7/14
This is misuse of the data—and it's not acceptable in scientific publishing.
7/14
The primary outcome was not reported.
❌ No data in results
❌ Not in the abstract
❌ No statistical tests
6/14
❌ No data in results
❌ Not in the abstract
❌ No statistical tests
6/14

June 18, 2025 at 5:18 AM
The primary outcome was not reported.
❌ No data in results
❌ Not in the abstract
❌ No statistical tests
6/14
❌ No data in results
❌ Not in the abstract
❌ No statistical tests
6/14
The pre-registered primary outcome was a change in non-calcified coronary plaque volume (NCPV) over 1 year.
This type of plaque is soft and rupture-prone—the kind that causes heart attacks.
Here’s the problem 👇
5/14
This type of plaque is soft and rupture-prone—the kind that causes heart attacks.
Here’s the problem 👇
5/14

June 18, 2025 at 5:18 AM
The pre-registered primary outcome was a change in non-calcified coronary plaque volume (NCPV) over 1 year.
This type of plaque is soft and rupture-prone—the kind that causes heart attacks.
Here’s the problem 👇
5/14
This type of plaque is soft and rupture-prone—the kind that causes heart attacks.
Here’s the problem 👇
5/14
The study enrolled 100 LMHRs who had:
– ≥2 years on keto
– No meds
– No smoking
– Normal HbA1c, glucose, BP, hsCRP
– LDL-C increase of ≥50% from baseline
A highly selected group—probably the “best case scenario” for testing this hypothesis.
4/14
– ≥2 years on keto
– No meds
– No smoking
– Normal HbA1c, glucose, BP, hsCRP
– LDL-C increase of ≥50% from baseline
A highly selected group—probably the “best case scenario” for testing this hypothesis.
4/14

June 18, 2025 at 5:18 AM
The study enrolled 100 LMHRs who had:
– ≥2 years on keto
– No meds
– No smoking
– Normal HbA1c, glucose, BP, hsCRP
– LDL-C increase of ≥50% from baseline
A highly selected group—probably the “best case scenario” for testing this hypothesis.
4/14
– ≥2 years on keto
– No meds
– No smoking
– Normal HbA1c, glucose, BP, hsCRP
– LDL-C increase of ≥50% from baseline
A highly selected group—probably the “best case scenario” for testing this hypothesis.
4/14
LMHRs are defined by:
🔸 LDL-C ≥190 mg/dL
🔸 HDL-C ≥60 mg/dL
🔸 TG ≤80 mg/dL
They’re lean, insulin-sensitive, and otherwise healthy.
Many claim their LDL-C increase on keto is harmless or even protective of atherosclerosis. KETO-CTA was supposed to test that.
3/14
🔸 LDL-C ≥190 mg/dL
🔸 HDL-C ≥60 mg/dL
🔸 TG ≤80 mg/dL
They’re lean, insulin-sensitive, and otherwise healthy.
Many claim their LDL-C increase on keto is harmless or even protective of atherosclerosis. KETO-CTA was supposed to test that.
3/14

June 18, 2025 at 5:18 AM
LMHRs are defined by:
🔸 LDL-C ≥190 mg/dL
🔸 HDL-C ≥60 mg/dL
🔸 TG ≤80 mg/dL
They’re lean, insulin-sensitive, and otherwise healthy.
Many claim their LDL-C increase on keto is harmless or even protective of atherosclerosis. KETO-CTA was supposed to test that.
3/14
🔸 LDL-C ≥190 mg/dL
🔸 HDL-C ≥60 mg/dL
🔸 TG ≤80 mg/dL
They’re lean, insulin-sensitive, and otherwise healthy.
Many claim their LDL-C increase on keto is harmless or even protective of atherosclerosis. KETO-CTA was supposed to test that.
3/14
The study asked a good research question: Can extremely high LDL-C in healthy, keto-adapted people still promote atherosclerosis?
The lead author of the study is Adrian Soto-Mota, with co-authors Dave Feldman, Nick Norwitz, and Dr. Matthew Budoff.
2/14
The lead author of the study is Adrian Soto-Mota, with co-authors Dave Feldman, Nick Norwitz, and Dr. Matthew Budoff.
2/14

June 18, 2025 at 5:18 AM
The study asked a good research question: Can extremely high LDL-C in healthy, keto-adapted people still promote atherosclerosis?
The lead author of the study is Adrian Soto-Mota, with co-authors Dave Feldman, Nick Norwitz, and Dr. Matthew Budoff.
2/14
The lead author of the study is Adrian Soto-Mota, with co-authors Dave Feldman, Nick Norwitz, and Dr. Matthew Budoff.
2/14
Another social media account. Exactly what I need.
November 27, 2024 at 7:19 PM
Another social media account. Exactly what I need.