



Anish K Patel
@anishkpatel.bsky.social
‘Just a GP’ posting about general practice and healthcare
At lights out my son asked, “Why are you allowed to go on your phone?” The room was quiet. My screen wasn’t. Children copy what we do, not what we say. If I can’t hold the line against the attention economy, how can I expect his developing brain to?
typeshare.co/anishkpatel/...
typeshare.co/anishkpatel/...

November 7, 2025 at 2:33 PM
At lights out my son asked, “Why are you allowed to go on your phone?” The room was quiet. My screen wasn’t. Children copy what we do, not what we say. If I can’t hold the line against the attention economy, how can I expect his developing brain to?
typeshare.co/anishkpatel/...
typeshare.co/anishkpatel/...
Oct 1 contract changes: online REQUESTS not online BOOKING. Gov says one thing, media go off and writes what they want.
When headlines promise booking, GPs get the heat, patients feel misled, and the bar for Wes jumps higher than he intended. 😬
When headlines promise booking, GPs get the heat, patients feel misled, and the bar for Wes jumps higher than he intended. 😬



October 3, 2025 at 12:29 PM
Oct 1 contract changes: online REQUESTS not online BOOKING. Gov says one thing, media go off and writes what they want.
When headlines promise booking, GPs get the heat, patients feel misled, and the bar for Wes jumps higher than he intended. 😬
When headlines promise booking, GPs get the heat, patients feel misled, and the bar for Wes jumps higher than he intended. 😬
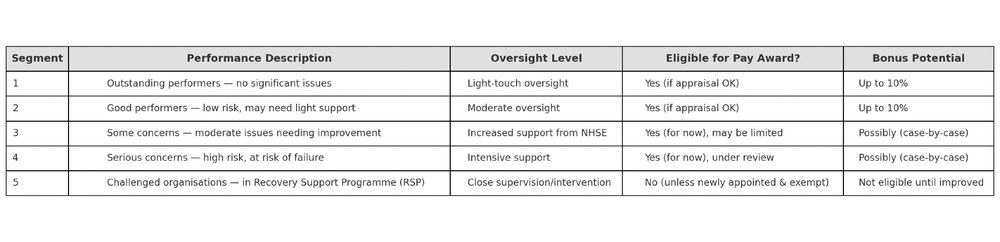
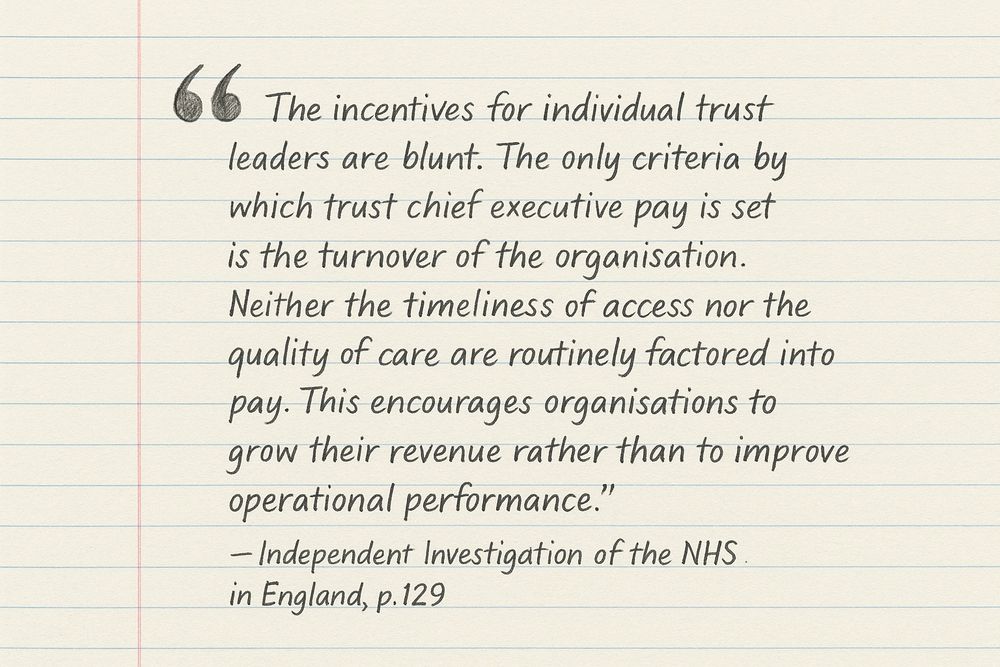
The new 2025 NHS very senior managers pay framework (yes it is called that) tries to shift that.
But it’s still layered on top of a structure that pays for scale, not sense.
Until that changes, the incentives won’t.
2/3
But it’s still layered on top of a structure that pays for scale, not sense.
Until that changes, the incentives won’t.
2/3
May 16, 2025 at 10:45 AM
The new 2025 NHS very senior managers pay framework (yes it is called that) tries to shift that.
But it’s still layered on top of a structure that pays for scale, not sense.
Until that changes, the incentives won’t.
2/3
But it’s still layered on top of a structure that pays for scale, not sense.
Until that changes, the incentives won’t.
2/3
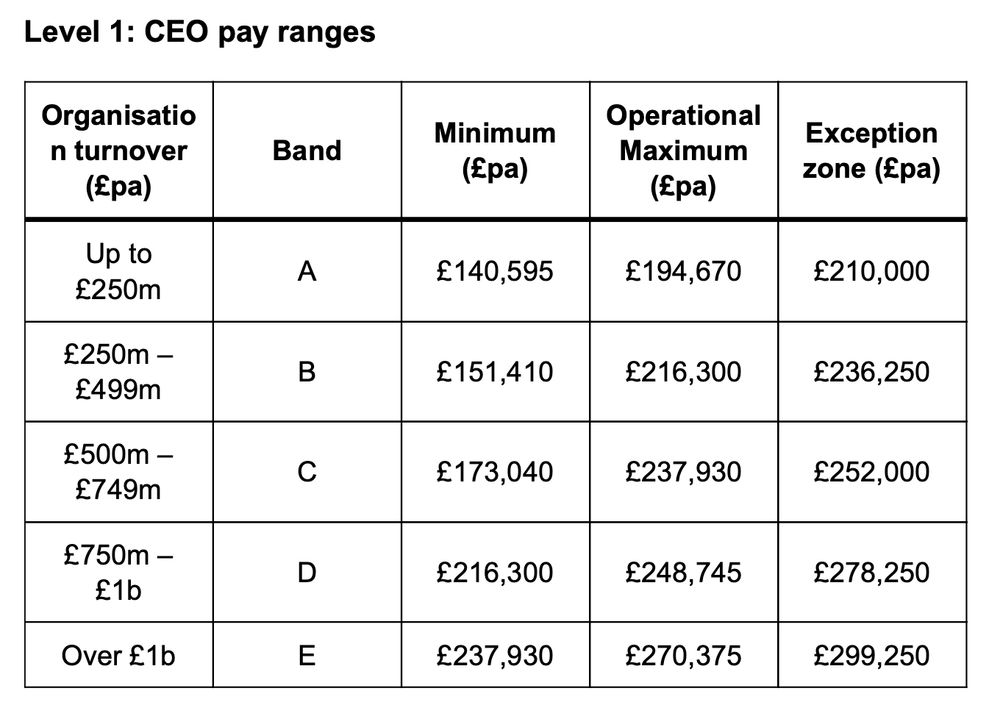
NHS Trust CEOs aren’t rewarded for collaboration.
They’re rewarded for control.
Bigger budget = bigger band = bigger pay.
Even if that means holding on when they should let go.
1/3
They’re rewarded for control.
Bigger budget = bigger band = bigger pay.
Even if that means holding on when they should let go.
1/3
May 16, 2025 at 10:45 AM
NHS Trust CEOs aren’t rewarded for collaboration.
They’re rewarded for control.
Bigger budget = bigger band = bigger pay.
Even if that means holding on when they should let go.
1/3
They’re rewarded for control.
Bigger budget = bigger band = bigger pay.
Even if that means holding on when they should let go.
1/3
I spoke with someone from the voluntary sector while at an ICB event this week. He saw firsthand the gaps in our health and social fabric.
I explained how GP practices in poorer areas actually receive less funding than those in richer ones. His eyes widened. 😳He had no idea.
I explained how GP practices in poorer areas actually receive less funding than those in richer ones. His eyes widened. 😳He had no idea.
May 15, 2025 at 1:45 PM
I spoke with someone from the voluntary sector while at an ICB event this week. He saw firsthand the gaps in our health and social fabric.
I explained how GP practices in poorer areas actually receive less funding than those in richer ones. His eyes widened. 😳He had no idea.
I explained how GP practices in poorer areas actually receive less funding than those in richer ones. His eyes widened. 😳He had no idea.
Psychologists call it the headwinds/tailwinds asymmetry.
We notice what holds us back more than what helps us forward.
A problem fixed is quickly forgotten.
We are experts as tracking hardship.
2/3
We notice what holds us back more than what helps us forward.
A problem fixed is quickly forgotten.
We are experts as tracking hardship.
2/3
May 9, 2025 at 1:44 PM
Psychologists call it the headwinds/tailwinds asymmetry.
We notice what holds us back more than what helps us forward.
A problem fixed is quickly forgotten.
We are experts as tracking hardship.
2/3
We notice what holds us back more than what helps us forward.
A problem fixed is quickly forgotten.
We are experts as tracking hardship.
2/3
It should be the most meaningful job in the world.
You help people when they’re scared, broken, or lost.
But instead of feeling fulfilled, you feel empty.
This is what burnout in the NHS really feels like.
And it’s not just happening.
It’s being designed into the system.
You help people when they’re scared, broken, or lost.
But instead of feeling fulfilled, you feel empty.
This is what burnout in the NHS really feels like.
And it’s not just happening.
It’s being designed into the system.
April 25, 2025 at 7:46 AM
It should be the most meaningful job in the world.
You help people when they’re scared, broken, or lost.
But instead of feeling fulfilled, you feel empty.
This is what burnout in the NHS really feels like.
And it’s not just happening.
It’s being designed into the system.
You help people when they’re scared, broken, or lost.
But instead of feeling fulfilled, you feel empty.
This is what burnout in the NHS really feels like.
And it’s not just happening.
It’s being designed into the system.
A Choice
This can be fixed
If we commit to funding new GP posts, we can:
✅ Make sure practices can afford to hire GPs
✅ Improve retention by spreading workload fairly
✅ Stop the brain drain to other countries
This is not a fantasy. The numbers do work.
This can be fixed
If we commit to funding new GP posts, we can:
✅ Make sure practices can afford to hire GPs
✅ Improve retention by spreading workload fairly
✅ Stop the brain drain to other countries
This is not a fantasy. The numbers do work.
February 7, 2025 at 1:14 PM
A Choice
This can be fixed
If we commit to funding new GP posts, we can:
✅ Make sure practices can afford to hire GPs
✅ Improve retention by spreading workload fairly
✅ Stop the brain drain to other countries
This is not a fantasy. The numbers do work.
This can be fixed
If we commit to funding new GP posts, we can:
✅ Make sure practices can afford to hire GPs
✅ Improve retention by spreading workload fairly
✅ Stop the brain drain to other countries
This is not a fantasy. The numbers do work.
The Global Competition
GPs are in demand worldwide. Canada, Australia, and New Zealand offer better pay, better working conditions, and a better work-life balance.
We are already training many of the world’s GPs. Do we want to keep them, or export them?
GPs are in demand worldwide. Canada, Australia, and New Zealand offer better pay, better working conditions, and a better work-life balance.
We are already training many of the world’s GPs. Do we want to keep them, or export them?
February 7, 2025 at 1:14 PM
The Global Competition
GPs are in demand worldwide. Canada, Australia, and New Zealand offer better pay, better working conditions, and a better work-life balance.
We are already training many of the world’s GPs. Do we want to keep them, or export them?
GPs are in demand worldwide. Canada, Australia, and New Zealand offer better pay, better working conditions, and a better work-life balance.
We are already training many of the world’s GPs. Do we want to keep them, or export them?
2️⃣ Hiring: A Funding Crisis
Another problem has emerged: qualified GPs can’t find jobs. It sounds absurd—we need more GPs, yet practices can’t afford to hire them. It is a failure to fund GP posts.
Another problem has emerged: qualified GPs can’t find jobs. It sounds absurd—we need more GPs, yet practices can’t afford to hire them. It is a failure to fund GP posts.
February 7, 2025 at 1:14 PM
2️⃣ Hiring: A Funding Crisis
Another problem has emerged: qualified GPs can’t find jobs. It sounds absurd—we need more GPs, yet practices can’t afford to hire them. It is a failure to fund GP posts.
Another problem has emerged: qualified GPs can’t find jobs. It sounds absurd—we need more GPs, yet practices can’t afford to hire them. It is a failure to fund GP posts.
1️⃣ Retention: The Leaky Bucket
Over the last decade, GPs have reduced hours, taken on non-traditional roles, or left the profession altogether.
Many have done this to avoid burnout.
Unless we fix retention, we’ll keep pouring new doctors into a leaky bucket.
Over the last decade, GPs have reduced hours, taken on non-traditional roles, or left the profession altogether.
Many have done this to avoid burnout.
Unless we fix retention, we’ll keep pouring new doctors into a leaky bucket.

February 7, 2025 at 1:14 PM
1️⃣ Retention: The Leaky Bucket
Over the last decade, GPs have reduced hours, taken on non-traditional roles, or left the profession altogether.
Many have done this to avoid burnout.
Unless we fix retention, we’ll keep pouring new doctors into a leaky bucket.
Over the last decade, GPs have reduced hours, taken on non-traditional roles, or left the profession altogether.
Many have done this to avoid burnout.
Unless we fix retention, we’ll keep pouring new doctors into a leaky bucket.
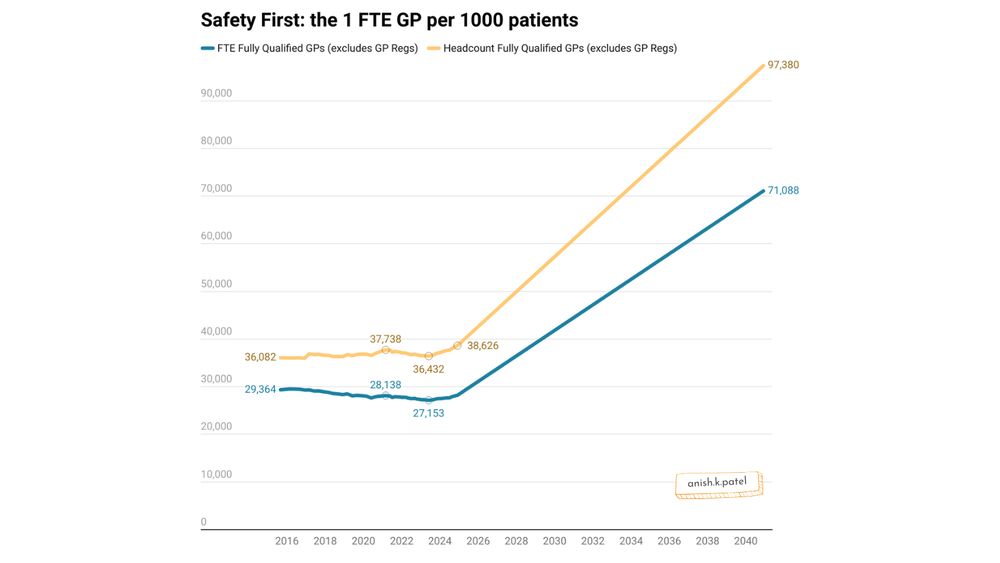
The GP Workforce: Past, Present, and Future
For over a decade, we’ve been losing GPs instead of gaining them. It's only recently stabilised.
Using ONS projected population growth and data on registered pts in England, I worked out what it would take to hit the 1:1000 target.
For over a decade, we’ve been losing GPs instead of gaining them. It's only recently stabilised.
Using ONS projected population growth and data on registered pts in England, I worked out what it would take to hit the 1:1000 target.
February 7, 2025 at 1:14 PM
The GP Workforce: Past, Present, and Future
For over a decade, we’ve been losing GPs instead of gaining them. It's only recently stabilised.
Using ONS projected population growth and data on registered pts in England, I worked out what it would take to hit the 1:1000 target.
For over a decade, we’ve been losing GPs instead of gaining them. It's only recently stabilised.
Using ONS projected population growth and data on registered pts in England, I worked out what it would take to hit the 1:1000 target.
Safety First: The Case for 1 GP per 1,000 Patients
GP numbers have not kept up with demand. But what would it take to fix this?
The BMA’s "gold standard" for safe general practice is 1 full-time GP per 1,000 patients. Ambitious? Yes. Impossible? Let’s break it down. 🧵
GP numbers have not kept up with demand. But what would it take to fix this?
The BMA’s "gold standard" for safe general practice is 1 full-time GP per 1,000 patients. Ambitious? Yes. Impossible? Let’s break it down. 🧵


February 7, 2025 at 1:14 PM
Safety First: The Case for 1 GP per 1,000 Patients
GP numbers have not kept up with demand. But what would it take to fix this?
The BMA’s "gold standard" for safe general practice is 1 full-time GP per 1,000 patients. Ambitious? Yes. Impossible? Let’s break it down. 🧵
GP numbers have not kept up with demand. But what would it take to fix this?
The BMA’s "gold standard" for safe general practice is 1 full-time GP per 1,000 patients. Ambitious? Yes. Impossible? Let’s break it down. 🧵
In the age of AI, PCSE can't get a form working on their online portal 🙃
God help us!
God help us!

February 6, 2025 at 6:09 PM
In the age of AI, PCSE can't get a form working on their online portal 🙃
God help us!
God help us!
This isn’t about becoming doctors who only review others’ work, give opinions, or handle the most complex cases. Instead, it’s about being approachable, building strong relationships, and earning trust with patients.

January 30, 2025 at 12:46 PM
This isn’t about becoming doctors who only review others’ work, give opinions, or handle the most complex cases. Instead, it’s about being approachable, building strong relationships, and earning trust with patients.
“Just a GP” – a phrase once wielded to belittle, now one I use with pride in my bio. The debate about the GP title continues. Does it still work? Is it holding us back?
🧵
🧵

January 30, 2025 at 12:46 PM
“Just a GP” – a phrase once wielded to belittle, now one I use with pride in my bio. The debate about the GP title continues. Does it still work? Is it holding us back?
🧵
🧵
The 4th shift to add to the NHS 10-Year Plan:
From sad, burnt-out staff → to happy, energised ones
As James Timpson says: 'At the heart of every successful venture lies a remarkable, happy team.'
From sad, burnt-out staff → to happy, energised ones
As James Timpson says: 'At the heart of every successful venture lies a remarkable, happy team.'

January 26, 2025 at 10:57 AM
The 4th shift to add to the NHS 10-Year Plan:
From sad, burnt-out staff → to happy, energised ones
As James Timpson says: 'At the heart of every successful venture lies a remarkable, happy team.'
From sad, burnt-out staff → to happy, energised ones
As James Timpson says: 'At the heart of every successful venture lies a remarkable, happy team.'
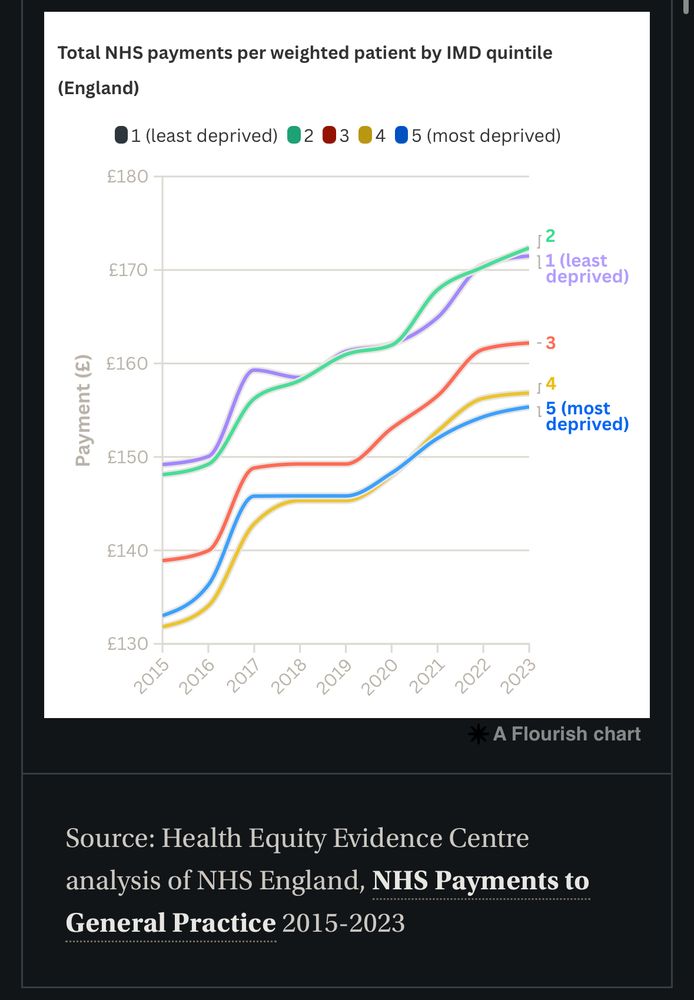
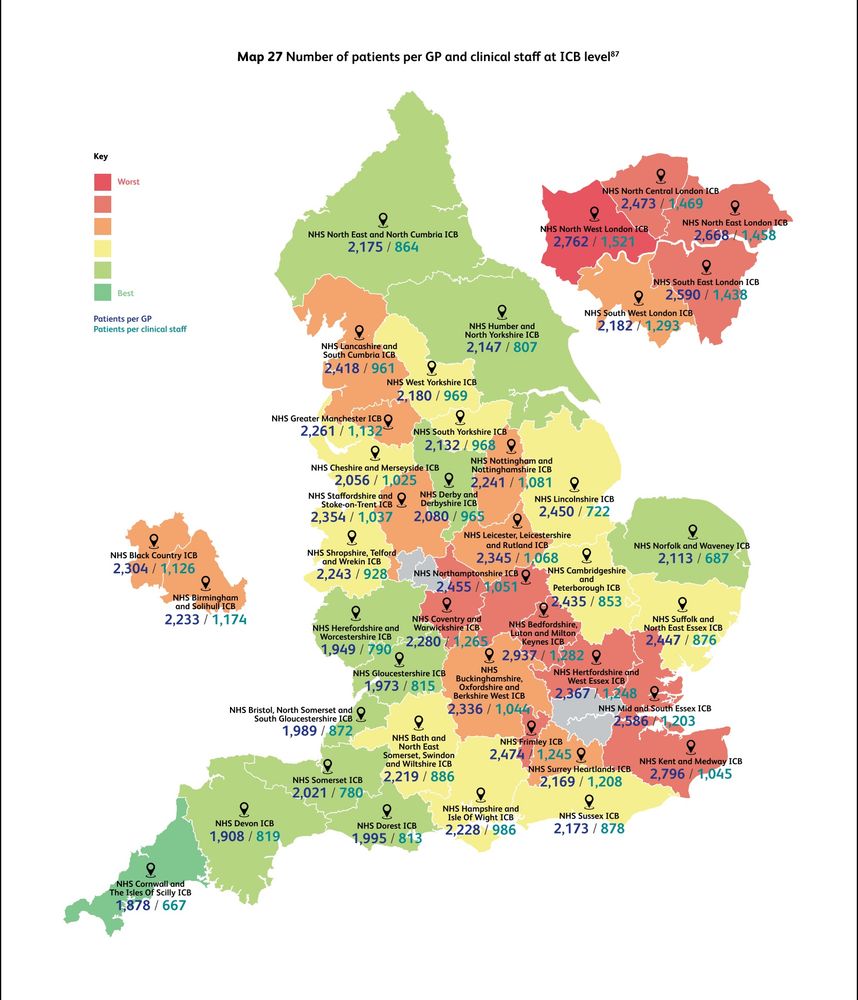
Is this the modern-day NHS postcode lottery?
Where you live determines your access to General Practice—if not the access itself, then the type of access.
Can’t help thinking part of this is driven by inequitable funding via Carr-Hill formula.
Where you live determines your access to General Practice—if not the access itself, then the type of access.
Can’t help thinking part of this is driven by inequitable funding via Carr-Hill formula.
January 24, 2025 at 1:56 PM
Is this the modern-day NHS postcode lottery?
Where you live determines your access to General Practice—if not the access itself, then the type of access.
Can’t help thinking part of this is driven by inequitable funding via Carr-Hill formula.
Where you live determines your access to General Practice—if not the access itself, then the type of access.
Can’t help thinking part of this is driven by inequitable funding via Carr-Hill formula.
There’s a better way forward, even if we’re unlikely to take it:
- Limit mandatory training to the most critical topics.
- Deliver engaging content designed for real learning.
- Move beyond a fear-driven, compliance-first mindset.
- Limit mandatory training to the most critical topics.
- Deliver engaging content designed for real learning.
- Move beyond a fear-driven, compliance-first mindset.

January 17, 2025 at 11:17 AM
There’s a better way forward, even if we’re unlikely to take it:
- Limit mandatory training to the most critical topics.
- Deliver engaging content designed for real learning.
- Move beyond a fear-driven, compliance-first mindset.
- Limit mandatory training to the most critical topics.
- Deliver engaging content designed for real learning.
- Move beyond a fear-driven, compliance-first mindset.
This obsession with ticking boxes creates a bigger problem.
The more we add to mandatory training, the less meaningful it becomes. The most important lessons get lost beneath “nice-to-know” material. We get overloaded.
The more we add to mandatory training, the less meaningful it becomes. The most important lessons get lost beneath “nice-to-know” material. We get overloaded.

January 17, 2025 at 11:17 AM
This obsession with ticking boxes creates a bigger problem.
The more we add to mandatory training, the less meaningful it becomes. The most important lessons get lost beneath “nice-to-know” material. We get overloaded.
The more we add to mandatory training, the less meaningful it becomes. The most important lessons get lost beneath “nice-to-know” material. We get overloaded.
So, why stick with ineffective methods?
Simple: organisations fear the CQC. It’s all about ticking the cheapest, easiest boxes to prove compliance, not about meaningful learning.
Simple: organisations fear the CQC. It’s all about ticking the cheapest, easiest boxes to prove compliance, not about meaningful learning.

January 17, 2025 at 11:17 AM
So, why stick with ineffective methods?
Simple: organisations fear the CQC. It’s all about ticking the cheapest, easiest boxes to prove compliance, not about meaningful learning.
Simple: organisations fear the CQC. It’s all about ticking the cheapest, easiest boxes to prove compliance, not about meaningful learning.
If training is mandatory, it must also be high quality.
Most GP practices use platforms like Bluestream—slide decks pretending to be interactive. They’re dry, disengaging, and feel like a chore.
Most GP practices use platforms like Bluestream—slide decks pretending to be interactive. They’re dry, disengaging, and feel like a chore.

January 17, 2025 at 11:17 AM
If training is mandatory, it must also be high quality.
Most GP practices use platforms like Bluestream—slide decks pretending to be interactive. They’re dry, disengaging, and feel like a chore.
Most GP practices use platforms like Bluestream—slide decks pretending to be interactive. They’re dry, disengaging, and feel like a chore.
What makes something mandatory?
Some topics are no-brainers: fire safety and basic life support. But every year, new items are added to the list, and nothing is removed. Where does it stop?
Some topics are no-brainers: fire safety and basic life support. But every year, new items are added to the list, and nothing is removed. Where does it stop?

January 17, 2025 at 11:17 AM
What makes something mandatory?
Some topics are no-brainers: fire safety and basic life support. But every year, new items are added to the list, and nothing is removed. Where does it stop?
Some topics are no-brainers: fire safety and basic life support. But every year, new items are added to the list, and nothing is removed. Where does it stop?
Mandatory training has lost its way.
Once a tool for learning critical skills, it's now a growing list of endless requirements. If everything is mandatory, is anything truly essential?
🧵
Once a tool for learning critical skills, it's now a growing list of endless requirements. If everything is mandatory, is anything truly essential?
🧵

January 17, 2025 at 11:17 AM
Mandatory training has lost its way.
Once a tool for learning critical skills, it's now a growing list of endless requirements. If everything is mandatory, is anything truly essential?
🧵
Once a tool for learning critical skills, it's now a growing list of endless requirements. If everything is mandatory, is anything truly essential?
🧵
That said, if you find someone who 1. understands your original intent, 2. adapts to new information, and 3. takes the time to support you—hold on to them. They’re rare and invaluable.

January 9, 2025 at 12:13 PM
That said, if you find someone who 1. understands your original intent, 2. adapts to new information, and 3. takes the time to support you—hold on to them. They’re rare and invaluable.