




Alexandre Bolze
@alexbolze.bsky.social
Human Geneticist. Principal scientist and PI at Helix.
All of the Helix presentations at
@theacmg.bsky.social #ACMGMtg25 today
👇
Come see me at poster 101 to discuss PMS2, lower penetrance and NCCN guidelines.
And at poster 217 on how we are helping variant interpretation with a resource for the PS4 criteria.
@theacmg.bsky.social #ACMGMtg25 today
👇
Come see me at poster 101 to discuss PMS2, lower penetrance and NCCN guidelines.
And at poster 217 on how we are helping variant interpretation with a resource for the PS4 criteria.

March 20, 2025 at 3:48 PM
All of the Helix presentations at
@theacmg.bsky.social #ACMGMtg25 today
👇
Come see me at poster 101 to discuss PMS2, lower penetrance and NCCN guidelines.
And at poster 217 on how we are helping variant interpretation with a resource for the PS4 criteria.
@theacmg.bsky.social #ACMGMtg25 today
👇
Come see me at poster 101 to discuss PMS2, lower penetrance and NCCN guidelines.
And at poster 217 on how we are helping variant interpretation with a resource for the PS4 criteria.
Great talk by Dr. Chad Haldeman-Englert @theacmg.bsky.social #ACMGMtg25
discussing @conehealth.bsky.social GeneConnect program & the Helix Research Network.
He calls every participant with a positive genetic finding.
=> it leads to a very high genetic counseling uptake after ~90%.
discussing @conehealth.bsky.social GeneConnect program & the Helix Research Network.
He calls every participant with a positive genetic finding.
=> it leads to a very high genetic counseling uptake after ~90%.


March 19, 2025 at 5:54 AM
Great talk by Dr. Chad Haldeman-Englert @theacmg.bsky.social #ACMGMtg25
discussing @conehealth.bsky.social GeneConnect program & the Helix Research Network.
He calls every participant with a positive genetic finding.
=> it leads to a very high genetic counseling uptake after ~90%.
discussing @conehealth.bsky.social GeneConnect program & the Helix Research Network.
He calls every participant with a positive genetic finding.
=> it leads to a very high genetic counseling uptake after ~90%.
6/
This study shows that clinical actions were taken for individuals with a FH pathogenic variant + it leads to lower LDL-C.
It also shows some of the care gaps.
Great foundation to increase use of genetics in healthcare. Need more of these.
👏 authors & 8 health systems 👇
This study shows that clinical actions were taken for individuals with a FH pathogenic variant + it leads to lower LDL-C.
It also shows some of the care gaps.
Great foundation to increase use of genetics in healthcare. Need more of these.
👏 authors & 8 health systems 👇

March 17, 2025 at 7:15 PM
6/
This study shows that clinical actions were taken for individuals with a FH pathogenic variant + it leads to lower LDL-C.
It also shows some of the care gaps.
Great foundation to increase use of genetics in healthcare. Need more of these.
👏 authors & 8 health systems 👇
This study shows that clinical actions were taken for individuals with a FH pathogenic variant + it leads to lower LDL-C.
It also shows some of the care gaps.
Great foundation to increase use of genetics in healthcare. Need more of these.
👏 authors & 8 health systems 👇
5/
Patients with new/modified therapies had a mean LDL-C reduction of 59mg/dL and 42.0% achieved the hard goal of ≥50% LDL-C reduction or LDL-C ≤70mg/dL.
Patients with new/modified therapies had a mean LDL-C reduction of 59mg/dL and 42.0% achieved the hard goal of ≥50% LDL-C reduction or LDL-C ≤70mg/dL.

March 17, 2025 at 7:15 PM
5/
Patients with new/modified therapies had a mean LDL-C reduction of 59mg/dL and 42.0% achieved the hard goal of ≥50% LDL-C reduction or LDL-C ≤70mg/dL.
Patients with new/modified therapies had a mean LDL-C reduction of 59mg/dL and 42.0% achieved the hard goal of ≥50% LDL-C reduction or LDL-C ≤70mg/dL.
4/
Overall, 33% received new/modified lipid-lowering therapy within up to 3 years. Rate was 55% for those with a newly documented FH diagnosis code.
See below the new LDL-lowering agents and therapeutic changes stratified by pre-screening treatment status
Overall, 33% received new/modified lipid-lowering therapy within up to 3 years. Rate was 55% for those with a newly documented FH diagnosis code.
See below the new LDL-lowering agents and therapeutic changes stratified by pre-screening treatment status

March 17, 2025 at 7:15 PM
4/
Overall, 33% received new/modified lipid-lowering therapy within up to 3 years. Rate was 55% for those with a newly documented FH diagnosis code.
See below the new LDL-lowering agents and therapeutic changes stratified by pre-screening treatment status
Overall, 33% received new/modified lipid-lowering therapy within up to 3 years. Rate was 55% for those with a newly documented FH diagnosis code.
See below the new LDL-lowering agents and therapeutic changes stratified by pre-screening treatment status
3/
Aim: to evaluate changes in clinical management and LDL-C levels among patients we identified with FH.
We studied 453 participants who had enough retrospective and prospective EHR data available.
Among those, 85% (n=384) did not have a prior clinical FH diagnosis.
Aim: to evaluate changes in clinical management and LDL-C levels among patients we identified with FH.
We studied 453 participants who had enough retrospective and prospective EHR data available.
Among those, 85% (n=384) did not have a prior clinical FH diagnosis.

March 17, 2025 at 7:15 PM
3/
Aim: to evaluate changes in clinical management and LDL-C levels among patients we identified with FH.
We studied 453 participants who had enough retrospective and prospective EHR data available.
Among those, 85% (n=384) did not have a prior clinical FH diagnosis.
Aim: to evaluate changes in clinical management and LDL-C levels among patients we identified with FH.
We studied 453 participants who had enough retrospective and prospective EHR data available.
Among those, 85% (n=384) did not have a prior clinical FH diagnosis.
2/
FH is part of the CDC-Tier 1 conditions because it is very high penetrance & actionable
FH is caused by variants in APOB, PCSK9, and LDLR.
Among 211,263 adults participating in The Helix Research Network,
1,020 had FH. That is 1 in 207.
=> more than 1.5 millions in USA with FH.
FH is part of the CDC-Tier 1 conditions because it is very high penetrance & actionable
FH is caused by variants in APOB, PCSK9, and LDLR.
Among 211,263 adults participating in The Helix Research Network,
1,020 had FH. That is 1 in 207.
=> more than 1.5 millions in USA with FH.

March 17, 2025 at 7:15 PM
2/
FH is part of the CDC-Tier 1 conditions because it is very high penetrance & actionable
FH is caused by variants in APOB, PCSK9, and LDLR.
Among 211,263 adults participating in The Helix Research Network,
1,020 had FH. That is 1 in 207.
=> more than 1.5 millions in USA with FH.
FH is part of the CDC-Tier 1 conditions because it is very high penetrance & actionable
FH is caused by variants in APOB, PCSK9, and LDLR.
Among 211,263 adults participating in The Helix Research Network,
1,020 had FH. That is 1 in 207.
=> more than 1.5 millions in USA with FH.
Lastly, a huge thanks to all of the participants in the Helix Research Network and all health systems, PIs, and collaborators involved.
Happy to discuss with anyone interested in this topic.
Happy to discuss with anyone interested in this topic.

November 18, 2024 at 5:28 PM
Lastly, a huge thanks to all of the participants in the Helix Research Network and all health systems, PIs, and collaborators involved.
Happy to discuss with anyone interested in this topic.
Happy to discuss with anyone interested in this topic.
Many many questions need to be answered. This was one way to start tackling the problem. Because we need to start putting more effort to figure out the 'low' part of the risk scale.

November 18, 2024 at 5:28 PM
Many many questions need to be answered. This was one way to start tackling the problem. Because we need to start putting more effort to figure out the 'low' part of the risk scale.
USPSTF now recommends that all women start biennial mammogram screening at age 40.
Taking a 'risk equivalent' approach, women in the 'low risk' group could delay start of mammogram screening by ~5 years.
Taking a 'risk equivalent' approach, women in the 'low risk' group could delay start of mammogram screening by ~5 years.

November 18, 2024 at 5:28 PM
USPSTF now recommends that all women start biennial mammogram screening at age 40.
Taking a 'risk equivalent' approach, women in the 'low risk' group could delay start of mammogram screening by ~5 years.
Taking a 'risk equivalent' approach, women in the 'low risk' group could delay start of mammogram screening by ~5 years.
Based on these results, we decided that for breast cancer, the only group of variants that meet our initial def of variants of potential risk would be the
pLOF vars with AF<0.001% in BARD1, CDH1, MAP3K1, RAD51C,RAD51D and TP53.
We can now risk stratify the entire pop.
pLOF vars with AF<0.001% in BARD1, CDH1, MAP3K1, RAD51C,RAD51D and TP53.
We can now risk stratify the entire pop.

November 18, 2024 at 5:28 PM
Based on these results, we decided that for breast cancer, the only group of variants that meet our initial def of variants of potential risk would be the
pLOF vars with AF<0.001% in BARD1, CDH1, MAP3K1, RAD51C,RAD51D and TP53.
We can now risk stratify the entire pop.
pLOF vars with AF<0.001% in BARD1, CDH1, MAP3K1, RAD51C,RAD51D and TP53.
We can now risk stratify the entire pop.
Looking at the hazard ratio compared to the avg pop for each group
- Path vars in BRCA1/2 or PALB2,ATM,CHEK2 had high risk (pos contrl)
- Coding vars <0.001% AF (many are VUS) have no impact
- only 1 group had a HR > 2: very rare pLOF in the additional set of genes (ex: rare nonsense in TP53)
- Path vars in BRCA1/2 or PALB2,ATM,CHEK2 had high risk (pos contrl)
- Coding vars <0.001% AF (many are VUS) have no impact
- only 1 group had a HR > 2: very rare pLOF in the additional set of genes (ex: rare nonsense in TP53)

November 18, 2024 at 5:28 PM
Looking at the hazard ratio compared to the avg pop for each group
- Path vars in BRCA1/2 or PALB2,ATM,CHEK2 had high risk (pos contrl)
- Coding vars <0.001% AF (many are VUS) have no impact
- only 1 group had a HR > 2: very rare pLOF in the additional set of genes (ex: rare nonsense in TP53)
- Path vars in BRCA1/2 or PALB2,ATM,CHEK2 had high risk (pos contrl)
- Coding vars <0.001% AF (many are VUS) have no impact
- only 1 group had a HR > 2: very rare pLOF in the additional set of genes (ex: rare nonsense in TP53)
We defined 8 exclusive categories of Variants of Potential Risks
(6 after removing the 2 where >90% of the vars are called Pathogenic).
For each, we identified the carriers, and then did a time to event analysis.
(6 after removing the 2 where >90% of the vars are called Pathogenic).
For each, we identified the carriers, and then did a time to event analysis.

November 18, 2024 at 5:28 PM
We defined 8 exclusive categories of Variants of Potential Risks
(6 after removing the 2 where >90% of the vars are called Pathogenic).
For each, we identified the carriers, and then did a time to event analysis.
(6 after removing the 2 where >90% of the vars are called Pathogenic).
For each, we identified the carriers, and then did a time to event analysis.
So we tried this approach in the Helix Research Network.
It is a fantastic emerging network of health systems in US (& Canada now) with a single research protocol, Exome+ seq for all participants, and nice EHR data.
First experiment was on breast cancer.
It is a fantastic emerging network of health systems in US (& Canada now) with a single research protocol, Exome+ seq for all participants, and nice EHR data.
First experiment was on breast cancer.

November 18, 2024 at 5:28 PM
So we tried this approach in the Helix Research Network.
It is a fantastic emerging network of health systems in US (& Canada now) with a single research protocol, Exome+ seq for all participants, and nice EHR data.
First experiment was on breast cancer.
It is a fantastic emerging network of health systems in US (& Canada now) with a single research protocol, Exome+ seq for all participants, and nice EHR data.
First experiment was on breast cancer.
But how do you define those variants of potential risks?
Could be VUSs, or VUS high. But in our hands, aggregate effect of these are close to zero. Maybe we can narrow down AND make interpretation automatic. This is key because one goal is to lower overall burden on healthcare enterprise.
Could be VUSs, or VUS high. But in our hands, aggregate effect of these are close to zero. Maybe we can narrow down AND make interpretation automatic. This is key because one goal is to lower overall burden on healthcare enterprise.

November 18, 2024 at 5:28 PM
But how do you define those variants of potential risks?
Could be VUSs, or VUS high. But in our hands, aggregate effect of these are close to zero. Maybe we can narrow down AND make interpretation automatic. This is key because one goal is to lower overall burden on healthcare enterprise.
Could be VUSs, or VUS high. But in our hands, aggregate effect of these are close to zero. Maybe we can narrow down AND make interpretation automatic. This is key because one goal is to lower overall burden on healthcare enterprise.
This is how we think about risk stratification using both rare variants and common variants.
We added an intermediate level looking at rare variants of potential risk.
Variants that don't meet Pathogenic criteria. But that are suspicious enough to exclude a person from 'low risk' category.
We added an intermediate level looking at rare variants of potential risk.
Variants that don't meet Pathogenic criteria. But that are suspicious enough to exclude a person from 'low risk' category.

November 18, 2024 at 5:28 PM
This is how we think about risk stratification using both rare variants and common variants.
We added an intermediate level looking at rare variants of potential risk.
Variants that don't meet Pathogenic criteria. But that are suspicious enough to exclude a person from 'low risk' category.
We added an intermediate level looking at rare variants of potential risk.
Variants that don't meet Pathogenic criteria. But that are suspicious enough to exclude a person from 'low risk' category.
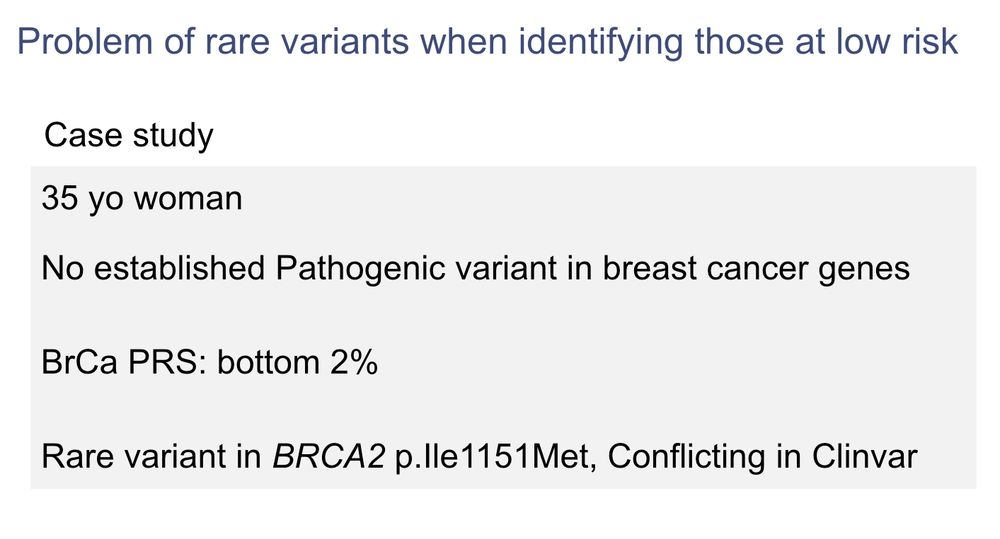
So why don't we return these results for lower risk of disease to people?
- no guidelines currently
- perception that it is riskier to make the recommendation to not follow standard guidelines and screen less.
Is it ok to tell the person 👇 she is at low risk of breast cancer ??
- no guidelines currently
- perception that it is riskier to make the recommendation to not follow standard guidelines and screen less.
Is it ok to tell the person 👇 she is at low risk of breast cancer ??
November 18, 2024 at 5:28 PM
So why don't we return these results for lower risk of disease to people?
- no guidelines currently
- perception that it is riskier to make the recommendation to not follow standard guidelines and screen less.
Is it ok to tell the person 👇 she is at low risk of breast cancer ??
- no guidelines currently
- perception that it is riskier to make the recommendation to not follow standard guidelines and screen less.
Is it ok to tell the person 👇 she is at low risk of breast cancer ??
Genetics can be used to identify those at higher risk, or those at lower risk of disease. It usually requires looking at both rare variants with potential large effects and common variants in the form of a polygenic risk score.
Example of breast cancer 👇
Example of breast cancer 👇

November 18, 2024 at 5:28 PM
Genetics can be used to identify those at higher risk, or those at lower risk of disease. It usually requires looking at both rare variants with potential large effects and common variants in the form of a polygenic risk score.
Example of breast cancer 👇
Example of breast cancer 👇
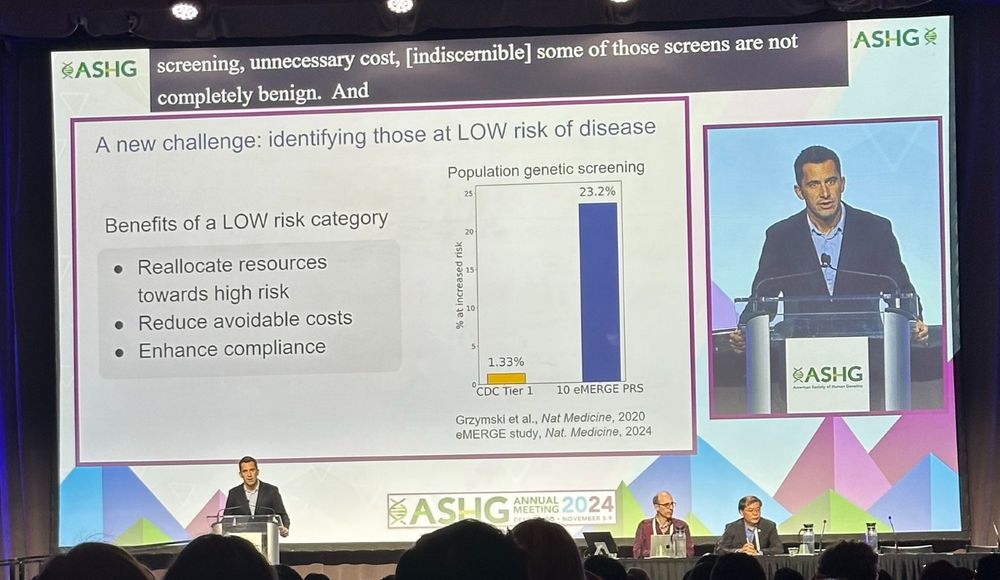
It was great to present our work on the genetics of resistance to disease & how to return results of low disease risk to people at #ASHG24
Why a focus on low risk?
- can't only do high risk, high risk, high risk
- clear benefits to patients
- maybe easier to explain avg risk
🧵 with slides
Why a focus on low risk?
- can't only do high risk, high risk, high risk
- clear benefits to patients
- maybe easier to explain avg risk
🧵 with slides
November 18, 2024 at 5:28 PM
It was great to present our work on the genetics of resistance to disease & how to return results of low disease risk to people at #ASHG24
Why a focus on low risk?
- can't only do high risk, high risk, high risk
- clear benefits to patients
- maybe easier to explain avg risk
🧵 with slides
Why a focus on low risk?
- can't only do high risk, high risk, high risk
- clear benefits to patients
- maybe easier to explain avg risk
🧵 with slides