




Alberto Espay
@albertoespay.bsky.social
Neurology professor at the University of Cincinnati, an advocate of precision and rescue medicines for Parkinson's & Alzheimer's. Author #BrainFables.
(4/9) Why does lecanemab look better? It is compared to a steeper-than-modeled slope from ADNI. Whereas the newly modeled decline is 0.05/mo ((1.5-0.6)/18), the observed decline is 0.07/mo ((1.8-0.5)/18), which means an actual 40% acceleration of decline ((0.07-0.05)/0.05)* 100).


September 5, 2025 at 9:01 PM
(4/9) Why does lecanemab look better? It is compared to a steeper-than-modeled slope from ADNI. Whereas the newly modeled decline is 0.05/mo ((1.5-0.6)/18), the observed decline is 0.07/mo ((1.8-0.5)/18), which means an actual 40% acceleration of decline ((0.07-0.05)/0.05)* 100).
(3/9) 2025 𝐥𝐞𝐜𝐚𝐧𝐞𝐦𝐚𝐛 𝐝𝐚𝐭𝐚: At 18 months (0.8-0.5 = 0.3) and 36 months (2.0-1.8 = 0.2), lecanemab slowed the CDR-SB decline by 37.5% vs placebo in the first period (0.3 / 0.8) \* 100). That difference narrowed to 10% in the second (0.2 / 2.0) \* 100).


September 5, 2025 at 9:01 PM
(3/9) 2025 𝐥𝐞𝐜𝐚𝐧𝐞𝐦𝐚𝐛 𝐝𝐚𝐭𝐚: At 18 months (0.8-0.5 = 0.3) and 36 months (2.0-1.8 = 0.2), lecanemab slowed the CDR-SB decline by 37.5% vs placebo in the first period (0.3 / 0.8) \* 100). That difference narrowed to 10% in the second (0.2 / 2.0) \* 100).
(2/9) 2024 𝐬𝐢𝐦𝐮𝐥𝐚𝐭𝐢𝐨𝐧: At 18 months (0.8-0.6 = 0.2) and 36 months (2.0-1.5 = 0.5), lecanemab 𝐬𝐥𝐨𝐰𝐞𝐝 𝐭𝐡𝐞 𝐂𝐃𝐑-𝐒𝐁 𝐝𝐞𝐜𝐥𝐢𝐧𝐞 by 25% vs placebo at both timepoints (0.2 / 0.8) \* 100) & (0.5 / 2.0) \* 100).


September 5, 2025 at 9:01 PM
(2/9) 2024 𝐬𝐢𝐦𝐮𝐥𝐚𝐭𝐢𝐨𝐧: At 18 months (0.8-0.6 = 0.2) and 36 months (2.0-1.5 = 0.5), lecanemab 𝐬𝐥𝐨𝐰𝐞𝐝 𝐭𝐡𝐞 𝐂𝐃𝐑-𝐒𝐁 𝐝𝐞𝐜𝐥𝐢𝐧𝐞 by 25% vs placebo at both timepoints (0.2 / 0.8) \* 100) & (0.5 / 2.0) \* 100).
Remember the “time saved” modeling for #Alzheimers infusions introduced a year ago? Extrapolating the observed curves, patients would increase their months ‘saved’ to 7.5. The #lecanemab data have shattered the optimistic model prediction—Details on this discrepancy follow (🧵1 of 5).


September 5, 2025 at 9:01 PM
Remember the “time saved” modeling for #Alzheimers infusions introduced a year ago? Extrapolating the observed curves, patients would increase their months ‘saved’ to 7.5. The #lecanemab data have shattered the optimistic model prediction—Details on this discrepancy follow (🧵1 of 5).
(6/9) Comparing the extrapolated slope of the placebo arm vs the observed donanemab arm, the CDR-SB difference favoring donanemab shrinks from 0.6 at 18 months to 0.3 at 36 months. Versus the ADNI slope used for lecanemab there would be no difference. This ADNI slope is steeper.

August 28, 2025 at 3:10 PM
(6/9) Comparing the extrapolated slope of the placebo arm vs the observed donanemab arm, the CDR-SB difference favoring donanemab shrinks from 0.6 at 18 months to 0.3 at 36 months. Versus the ADNI slope used for lecanemab there would be no difference. This ADNI slope is steeper.
(5/9) Comparing the extrapolated slope of the placebo arm vs the observed lecanemab arm, the CDR-SB difference favoring lecanemab does not expand but shrinks: from 0.5 at the end of the double-blind period to 0.2 at month 48 of the open-label extension.

August 28, 2025 at 3:10 PM
(5/9) Comparing the extrapolated slope of the placebo arm vs the observed lecanemab arm, the CDR-SB difference favoring lecanemab does not expand but shrinks: from 0.5 at the end of the double-blind period to 0.2 at month 48 of the open-label extension.
(3/9) Donanemab: In the 18 double-blind months, the CDR-SB score lowers by 1.6 (vs. 2.2 in placebo); in the subsequent 18 open-label months, the CDR-SB lowers 2.5 (4.1-1.6) –a 𝟱𝟲% 𝗳𝗮𝘀𝘁𝗲𝗿 𝗱𝗲𝗰𝗹𝗶𝗻𝗲 (2.5 -1.6 /1.6 * 100).

August 28, 2025 at 3:10 PM
(3/9) Donanemab: In the 18 double-blind months, the CDR-SB score lowers by 1.6 (vs. 2.2 in placebo); in the subsequent 18 open-label months, the CDR-SB lowers 2.5 (4.1-1.6) –a 𝟱𝟲% 𝗳𝗮𝘀𝘁𝗲𝗿 𝗱𝗲𝗰𝗹𝗶𝗻𝗲 (2.5 -1.6 /1.6 * 100).
(2/9) Lecanemab: In the 18 double-blind months, the CDR-SB score lowers (worsens) by 1.2 (vs. 1.7 in placebo); in the subsequent 18 open-label months, the CDR-SB lowers by 1.8 (3 -1.2) –a 𝟱𝟬% 𝗳𝗮𝘀𝘁𝗲𝗿 𝗱𝗲𝗰𝗹𝗶𝗻𝗲 (1.8 -1.2 /1.2 * 100).

August 28, 2025 at 3:10 PM
(2/9) Lecanemab: In the 18 double-blind months, the CDR-SB score lowers (worsens) by 1.2 (vs. 1.7 in placebo); in the subsequent 18 open-label months, the CDR-SB lowers by 1.8 (3 -1.2) –a 𝟱𝟬% 𝗳𝗮𝘀𝘁𝗲𝗿 𝗱𝗲𝗰𝗹𝗶𝗻𝗲 (1.8 -1.2 /1.2 * 100).
In #Alzheimers news: “4 years on #lecanemab, the benefit tripled” … “3 years on #donanemab, the benefit doubled”, as summed by @Alzforum from #AAIC25 reported data. How the graphical illusion hides the acceleration of cognitive decline (9-part thread).
www.alzforum.org/news/confere...
www.alzforum.org/news/confere...


August 28, 2025 at 3:10 PM
In #Alzheimers news: “4 years on #lecanemab, the benefit tripled” … “3 years on #donanemab, the benefit doubled”, as summed by @Alzforum from #AAIC25 reported data. How the graphical illusion hides the acceleration of cognitive decline (9-part thread).
www.alzforum.org/news/confere...
www.alzforum.org/news/confere...
5/7 The most interesting finding:
Higher CSF C-α-syn was linked to slower MMSE decline in AD. The higher the CSF C-α-syn, the lower the rate of MMSE change (dMMSE/dT) in AD patients; therefore, the more stable the MMSE is. This is good!
Higher CSF C-α-syn was linked to slower MMSE decline in AD. The higher the CSF C-α-syn, the lower the rate of MMSE change (dMMSE/dT) in AD patients; therefore, the more stable the MMSE is. This is good!

August 15, 2025 at 4:38 PM
5/7 The most interesting finding:
Higher CSF C-α-syn was linked to slower MMSE decline in AD. The higher the CSF C-α-syn, the lower the rate of MMSE change (dMMSE/dT) in AD patients; therefore, the more stable the MMSE is. This is good!
Higher CSF C-α-syn was linked to slower MMSE decline in AD. The higher the CSF C-α-syn, the lower the rate of MMSE change (dMMSE/dT) in AD patients; therefore, the more stable the MMSE is. This is good!
Looking forward to tomorrow's noon EST debate at Indiana University on 'proteinopathies' as cause (Dr. Malu Tamsey) versus consequence (me). Here is the link:

August 10, 2025 at 3:47 PM
Looking forward to tomorrow's noon EST debate at Indiana University on 'proteinopathies' as cause (Dr. Malu Tamsey) versus consequence (me). Here is the link:
The scorecard on the “diagnostic revolution” of #Alzheimers blood biomarkers based on 885 studies: sobering.
⚠️ Good lab accuracy, not real-world benefit
⚠️ No gains for patients or caregivers
Availability ≠ necessity. Don't do it just because you can.
www.bmj.com/content/390/...
⚠️ Good lab accuracy, not real-world benefit
⚠️ No gains for patients or caregivers
Availability ≠ necessity. Don't do it just because you can.
www.bmj.com/content/390/...

August 9, 2025 at 3:43 PM
The scorecard on the “diagnostic revolution” of #Alzheimers blood biomarkers based on 885 studies: sobering.
⚠️ Good lab accuracy, not real-world benefit
⚠️ No gains for patients or caregivers
Availability ≠ necessity. Don't do it just because you can.
www.bmj.com/content/390/...
⚠️ Good lab accuracy, not real-world benefit
⚠️ No gains for patients or caregivers
Availability ≠ necessity. Don't do it just because you can.
www.bmj.com/content/390/...
July 11, 2025 at 10:50 PM
(4/4) The biophysical model for reinterpreting brain proteins could redefine the approach to Alzheimer’s, Parkinson’s, and other neurodegenerative diseases—and help retire the “toxic protein” and "toxic amyloid" narratives from the neurological literature.

June 27, 2025 at 9:50 PM
(4/4) The biophysical model for reinterpreting brain proteins could redefine the approach to Alzheimer’s, Parkinson’s, and other neurodegenerative diseases—and help retire the “toxic protein” and "toxic amyloid" narratives from the neurological literature.
(3/4) Spread can be active or passive. The phase transition of water into ice is an example of passive “growth” via crystallization. The growth or “spread” of pathology in neurodegenerative disorders reflects the transition of normal proteins.

June 27, 2025 at 9:50 PM
(3/4) Spread can be active or passive. The phase transition of water into ice is an example of passive “growth” via crystallization. The growth or “spread” of pathology in neurodegenerative disorders reflects the transition of normal proteins.
(2/4) Pathological proteins do not 'template' or encode themselves onto others. Under electron microscopy, they do not form identical copies of themselves, 'strains', but rather infinitely diverse fibrils, or polymorphs in a biophysical language. febs.onlinelibrary.wiley.com/doi/10.1002/...

June 27, 2025 at 9:50 PM
(2/4) Pathological proteins do not 'template' or encode themselves onto others. Under electron microscopy, they do not form identical copies of themselves, 'strains', but rather infinitely diverse fibrils, or polymorphs in a biophysical language. febs.onlinelibrary.wiley.com/doi/10.1002/...
Two articles this week highlight the importance of high CSF Aβ42 levels in lowering the risk of dementia:
1. Prediction of cognitive impairment via a computational modeling framework: "Higher CSF Aβ42 levels consistently demonstrated a protective effect".
www.mdpi.com/2075-4418/15...
1. Prediction of cognitive impairment via a computational modeling framework: "Higher CSF Aβ42 levels consistently demonstrated a protective effect".
www.mdpi.com/2075-4418/15...

June 14, 2025 at 3:31 PM
Two articles this week highlight the importance of high CSF Aβ42 levels in lowering the risk of dementia:
1. Prediction of cognitive impairment via a computational modeling framework: "Higher CSF Aβ42 levels consistently demonstrated a protective effect".
www.mdpi.com/2075-4418/15...
1. Prediction of cognitive impairment via a computational modeling framework: "Higher CSF Aβ42 levels consistently demonstrated a protective effect".
www.mdpi.com/2075-4418/15...
Should we stop embarking on epidemiology-inspired disease-modifying clinical trials in #Parkinsons? I think so. But the 'disagree' side remains popular. This 2024 PSG debate (against 'opponent' Michael Schwarzschild) has just been published in @ParkinsonismD.
authors.elsevier.com/c/1lFg54pqQO...
authors.elsevier.com/c/1lFg54pqQO...

June 13, 2025 at 1:39 PM
Should we stop embarking on epidemiology-inspired disease-modifying clinical trials in #Parkinsons? I think so. But the 'disagree' side remains popular. This 2024 PSG debate (against 'opponent' Michael Schwarzschild) has just been published in @ParkinsonismD.
authors.elsevier.com/c/1lFg54pqQO...
authors.elsevier.com/c/1lFg54pqQO...
The @alzassociation Workgroup created a 2-dimensional "biological-clinical staging framework" in 2024. New #ADNI data showed it only explains progression in one-third of participants. The framework is divorced from reality. Can we divorce ourselves from it?
www.neurology.org/doi/10.1212/...
www.neurology.org/doi/10.1212/...

June 11, 2025 at 5:19 PM
The @alzassociation Workgroup created a 2-dimensional "biological-clinical staging framework" in 2024. New #ADNI data showed it only explains progression in one-third of participants. The framework is divorced from reality. Can we divorce ourselves from it?
www.neurology.org/doi/10.1212/...
www.neurology.org/doi/10.1212/...
APOE4 E4/E4 yields a 60% lifetime risk of #Alzheimers by age 85. E3/E3 does not affect risk. Why the difference?
Although amyloid and tau PET look similar, there is a rapid and early Aβ42-to-amyloid conversion in E4/E4, depleting CSF Aβ42 levels.
www.nature.com/articles/s41...
Although amyloid and tau PET look similar, there is a rapid and early Aβ42-to-amyloid conversion in E4/E4, depleting CSF Aβ42 levels.
www.nature.com/articles/s41...

June 3, 2025 at 12:03 PM
APOE4 E4/E4 yields a 60% lifetime risk of #Alzheimers by age 85. E3/E3 does not affect risk. Why the difference?
Although amyloid and tau PET look similar, there is a rapid and early Aβ42-to-amyloid conversion in E4/E4, depleting CSF Aβ42 levels.
www.nature.com/articles/s41...
Although amyloid and tau PET look similar, there is a rapid and early Aβ42-to-amyloid conversion in E4/E4, depleting CSF Aβ42 levels.
www.nature.com/articles/s41...
No real ‘biological-clinical alignment’ in #Alzheimers. Only 37.7% of BioFINDER-2 cohort matched pathological and clinical stages. How hard is it to say, 'biological' staging poorly predicts clinical disease, rather than blaming 'copathologies' for the discrepancy?
jamanetwork.com/journals/jam...
jamanetwork.com/journals/jam...

May 19, 2025 at 8:53 PM
No real ‘biological-clinical alignment’ in #Alzheimers. Only 37.7% of BioFINDER-2 cohort matched pathological and clinical stages. How hard is it to say, 'biological' staging poorly predicts clinical disease, rather than blaming 'copathologies' for the discrepancy?
jamanetwork.com/journals/jam...
jamanetwork.com/journals/jam...
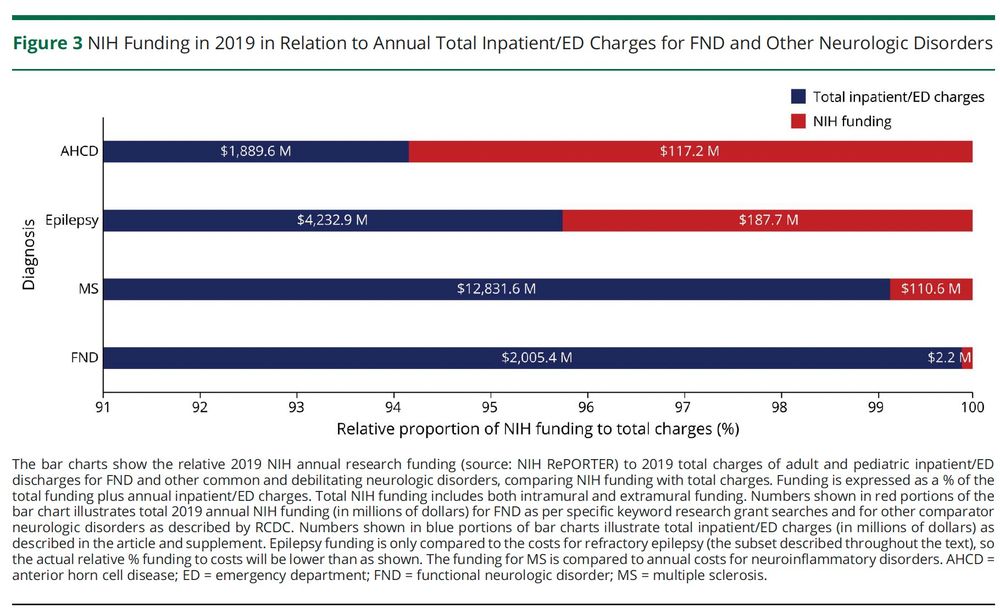
Functional neurological disorder (#FND) remains a research orphan at NIH. FND is among the costliest and least funded sources of neurological disability (see graph). The latest NIH review cycle was no exception: zero FND-based grants were funded.
www.neurology.org/doi/abs/10.1...
www.neurology.org/doi/abs/10.1...
May 17, 2025 at 3:07 PM
Functional neurological disorder (#FND) remains a research orphan at NIH. FND is among the costliest and least funded sources of neurological disability (see graph). The latest NIH review cycle was no exception: zero FND-based grants were funded.
www.neurology.org/doi/abs/10.1...
www.neurology.org/doi/abs/10.1...
(3/4) This is worse: Levodopa led to a “stage regression” in a significant number of patients:
• 8% of Stage 3 patients
• 41% (!) of Stage 4 patients
If a staging system can be shifted backward with asymptomatic treatment, can it reliably measure disease progression?
• 8% of Stage 3 patients
• 41% (!) of Stage 4 patients
If a staging system can be shifted backward with asymptomatic treatment, can it reliably measure disease progression?

May 1, 2025 at 12:32 AM
(3/4) This is worse: Levodopa led to a “stage regression” in a significant number of patients:
• 8% of Stage 3 patients
• 41% (!) of Stage 4 patients
If a staging system can be shifted backward with asymptomatic treatment, can it reliably measure disease progression?
• 8% of Stage 3 patients
• 41% (!) of Stage 4 patients
If a staging system can be shifted backward with asymptomatic treatment, can it reliably measure disease progression?
I am honored to deliver the Weiner Family Memorial Lecture this Wednesday at the University of Maryland, in memory of Prof. Bill Weiner, a visionary who challenged dogma in Parkinson’s research. His bold 2008 paper said it first: "There is no single Parkinson disease" jamanetwork.com/journals/jam...


April 28, 2025 at 10:09 PM
I am honored to deliver the Weiner Family Memorial Lecture this Wednesday at the University of Maryland, in memory of Prof. Bill Weiner, a visionary who challenged dogma in Parkinson’s research. His bold 2008 paper said it first: "There is no single Parkinson disease" jamanetwork.com/journals/jam...
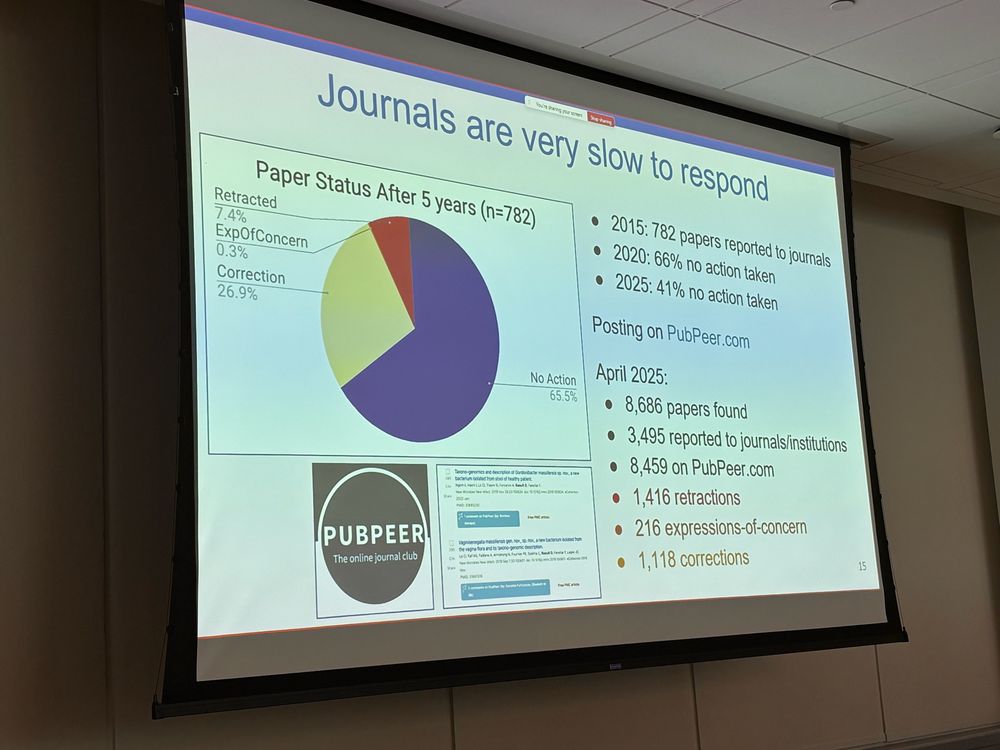
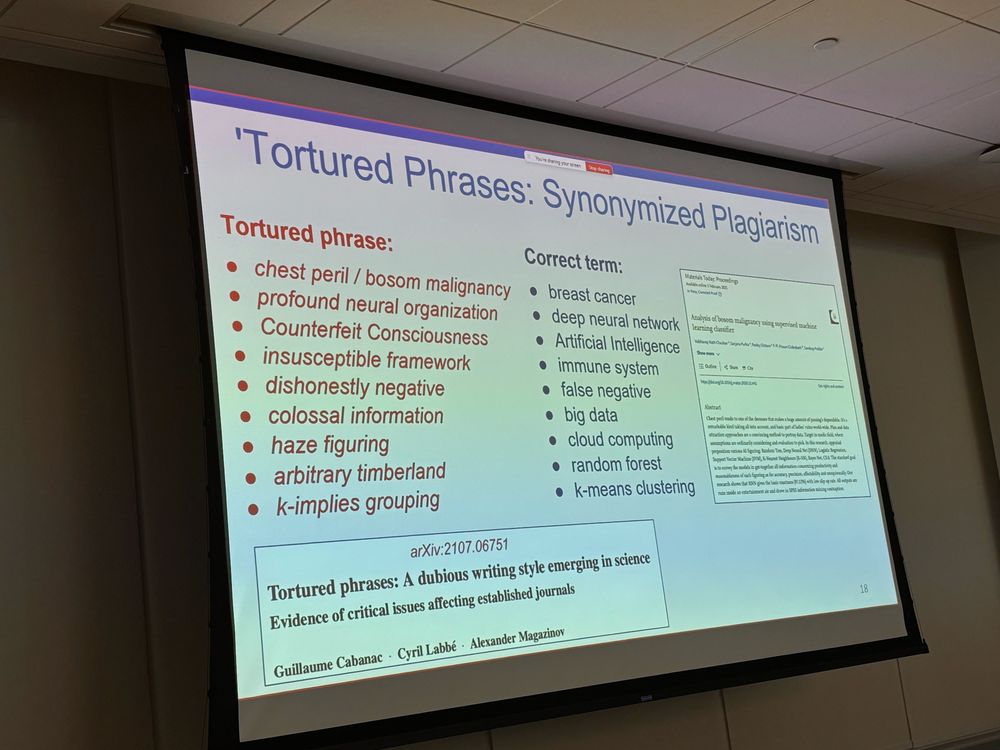
@elisabethbik.bsky.social delivered a brilliant Neurology Grand Rounds at the University of Cincinnati. Science is not self correcting. It requires correctors like Dr. Bik. Data pushed to fit theory will be uncovered, even if many years elapse before retractions. I’m grateful science sleuths exist!

April 18, 2025 at 10:22 PM
@elisabethbik.bsky.social delivered a brilliant Neurology Grand Rounds at the University of Cincinnati. Science is not self correcting. It requires correctors like Dr. Bik. Data pushed to fit theory will be uncovered, even if many years elapse before retractions. I’m grateful science sleuths exist!