



Under the rules of war, parties to conflicts must help families find answers about missing loved ones.
@corduladroege.bsky.social, ICRC's chief legal officer, explains what this means in practical terms for families 👇🏽
@corduladroege.bsky.social, ICRC's chief legal officer, explains what this means in practical terms for families 👇🏽
November 11, 2025 at 6:00 PM
Under the rules of war, parties to conflicts must help families find answers about missing loved ones.
@corduladroege.bsky.social, ICRC's chief legal officer, explains what this means in practical terms for families 👇🏽
@corduladroege.bsky.social, ICRC's chief legal officer, explains what this means in practical terms for families 👇🏽
📅 Save the date: 20 November | Implementing IHL in Challenging Times
Marking 30 years of the ICRC’s Advisory Service on #IHL, this event reaffirms that even in challenging times, implementing IHL is both possible and essential.
🔗 Sign up now: bit.ly/4nKxhgH
Marking 30 years of the ICRC’s Advisory Service on #IHL, this event reaffirms that even in challenging times, implementing IHL is both possible and essential.
🔗 Sign up now: bit.ly/4nKxhgH

EVENT: Implementing IHL in Challenging Times: A Panel Discussion to Mark the 30th Anniversary of the ICRC’s Advisory Service on IHL
bit.ly
November 7, 2025 at 12:08 PM
📅 Save the date: 20 November | Implementing IHL in Challenging Times
Marking 30 years of the ICRC’s Advisory Service on #IHL, this event reaffirms that even in challenging times, implementing IHL is both possible and essential.
🔗 Sign up now: bit.ly/4nKxhgH
Marking 30 years of the ICRC’s Advisory Service on #IHL, this event reaffirms that even in challenging times, implementing IHL is both possible and essential.
🔗 Sign up now: bit.ly/4nKxhgH
We have started a multi-phase operation to facilitate the release and transfer of hostages and detainees as part of a ceasefire agreement between Israel and Hamas.
More details here: ms.spr.ly/6182s2AQs
More details here: ms.spr.ly/6182s2AQs

October 13, 2025 at 6:52 AM
We have started a multi-phase operation to facilitate the release and transfer of hostages and detainees as part of a ceasefire agreement between Israel and Hamas.
More details here: ms.spr.ly/6182s2AQs
More details here: ms.spr.ly/6182s2AQs
AP looks at the ICRC's role in hostage and prisoner releases

www.youtube.com
AP looks at the ICRC's role in hostage and prisoner releases
twp.ai
October 9, 2025 at 10:44 PM
AP looks at the ICRC's role in hostage and prisoner releases

@diekjobst.bsky.social, @rosalauterbach.bsky.social and Paulina Rob introduce the joint series between #ArticlesofWar and @voelkerrechtsblog.org, which highlights the contested terrain of customary international humanitarian law two decades after the ICRC’s Study was first published.
September 19, 2025 at 3:55 PM
@diekjobst.bsky.social, @rosalauterbach.bsky.social and Paulina Rob introduce the joint series between #ArticlesofWar and @voelkerrechtsblog.org, which highlights the contested terrain of customary international humanitarian law two decades after the ICRC’s Study was first published.

World: Protecting and Ensuring Safe Access to education: The ICRC’s Experience and Approach in Armed Conflict and Other Situations of Violence
World: Protecting and Ensuring Safe Access to education: The ICRC’s Experience and Approach in Armed Conflict and Other Situations of Violence
Country: World
Source: International Committee of the Red Cross
Please refer to the attached file.
This report provides an overview of what the International Committee of the Red Cross (ICRC) does to protect and ensure safe access to education in places affected by armed conflict and other violence. The report has two objectives: First, to give a humanitarian perspective on the many ways in which conflict and other violence disrupts learning and to pay tribute to the perseverance and resourcefulness of children, young adults, teachers, parents and entire communities who ensure that schooling can continue in spite of war. Second, to familiarize governments, donors and peer organizations with the ICRC’s approach to protecting and ensuring safe access to education during armed conflict and other violence.
reliefweb.int
February 25, 2024 at 12:49 AM
World: Protecting and Ensuring Safe Access to education: The ICRC’s Experience and Approach in Armed Conflict and Other Situations of Violence

2/ According to Dmytro Usov, secretary of the Coordination Headquarters, the ICRC’s confirmation of captivity provides no guarantee that Ukrainians will return alive. "If we believed the Red Cross would protect prisoners, unfortunately, this is not the case," he said.
December 8, 2024 at 5:55 PM
2/ According to Dmytro Usov, secretary of the Coordination Headquarters, the ICRC’s confirmation of captivity provides no guarantee that Ukrainians will return alive. "If we believed the Red Cross would protect prisoners, unfortunately, this is not the case," he said.

eg From the ICRC's database, which gives more context. ihl-databases.icrc.org/en/customary...

ihl-databases.icrc.org
June 16, 2025 at 4:22 PM
eg From the ICRC's database, which gives more context. ihl-databases.icrc.org/en/customary...
Did you know the @icrc.org's first president was a General? Swiss General Dufour died exactly 150 years ago. The ICRC’s humanitarian mission was grounded in battlefield experience from the start.
🔗Today’s military perspectives in the Intl Review of the Red Cross: library.icrc.org/library/sear...
🔗Today’s military perspectives in the Intl Review of the Red Cross: library.icrc.org/library/sear...


July 14, 2025 at 2:10 PM
Did you know the @icrc.org's first president was a General? Swiss General Dufour died exactly 150 years ago. The ICRC’s humanitarian mission was grounded in battlefield experience from the start.
🔗Today’s military perspectives in the Intl Review of the Red Cross: library.icrc.org/library/sear...
🔗Today’s military perspectives in the Intl Review of the Red Cross: library.icrc.org/library/sear...

We're at Wolfson College @uniofcam.bsky.social today to mark the 10-year anniversary of the @icrc.org and @unhcr.org regulatory frameworks on personal data protection.
Our ED @ginasue.bsky.social and the ICRC's Head of Data Protection Office @massimomarelli.bsky.social delivered opening remarks.
Our ED @ginasue.bsky.social and the ICRC's Head of Data Protection Office @massimomarelli.bsky.social delivered opening remarks.



March 10, 2025 at 3:11 PM
We're at Wolfson College @uniofcam.bsky.social today to mark the 10-year anniversary of the @icrc.org and @unhcr.org regulatory frameworks on personal data protection.
Our ED @ginasue.bsky.social and the ICRC's Head of Data Protection Office @massimomarelli.bsky.social delivered opening remarks.
Our ED @ginasue.bsky.social and the ICRC's Head of Data Protection Office @massimomarelli.bsky.social delivered opening remarks.

There has been a lot of discussion this week about the UK’s continued commitment to critical weapons treaties. @icrc’s message is clear: the humanitarian cost of anti-personnel mines and cluster munitions is widespread, long lasting and devastating for civilians. Commitment must remain steadfast.
Anti-personnel mines don’t bring security—they bring suffering. A new ICRC blog by @corduladroege.bsky.social
& Maya Brehm explores why making exceptions for these weapons is a dangerous mistake.
It's time to prioritize humanity over false promises of safety.
blogs.icrc.org/law-and-poli...
& Maya Brehm explores why making exceptions for these weapons is a dangerous mistake.
It's time to prioritize humanity over false promises of safety.
blogs.icrc.org/law-and-poli...

Anti-personnel mines: the false promise of security through exceptionalism in war
Efforts to abandon the APMBC challenge fundamental precepts of IHL and undermine essential safeguards for upholding humanity in war.
blogs.icrc.org
April 5, 2025 at 11:16 AM
There has been a lot of discussion this week about the UK’s continued commitment to critical weapons treaties. @icrc’s message is clear: the humanitarian cost of anti-personnel mines and cluster munitions is widespread, long lasting and devastating for civilians. Commitment must remain steadfast.

Powerful moment in today's tech panel at #AISE2025: discussion on how commercial AI innovation inevitably influences military applications.
🌐 How do we maintain the right balance between innovation & responsibility? This is where ICRC's humanitarian perspective is essential. ⚖️
🌐 How do we maintain the right balance between innovation & responsibility? This is where ICRC's humanitarian perspective is essential. ⚖️
March 28, 2025 at 12:14 PM
Powerful moment in today's tech panel at #AISE2025: discussion on how commercial AI innovation inevitably influences military applications.
🌐 How do we maintain the right balance between innovation & responsibility? This is where ICRC's humanitarian perspective is essential. ⚖️
🌐 How do we maintain the right balance between innovation & responsibility? This is where ICRC's humanitarian perspective is essential. ⚖️

Of course, the ICRC study refers quite explicitly to IHL (ius in bello), i.e. to the application of the laws of war (= the ICRC's business), rather than to the ius ad bellum, i.e. the question when states may use force (= the UN SC's business). 3/
July 8, 2025 at 1:23 PM
Of course, the ICRC study refers quite explicitly to IHL (ius in bello), i.e. to the application of the laws of war (= the ICRC's business), rather than to the ius ad bellum, i.e. the question when states may use force (= the UN SC's business). 3/
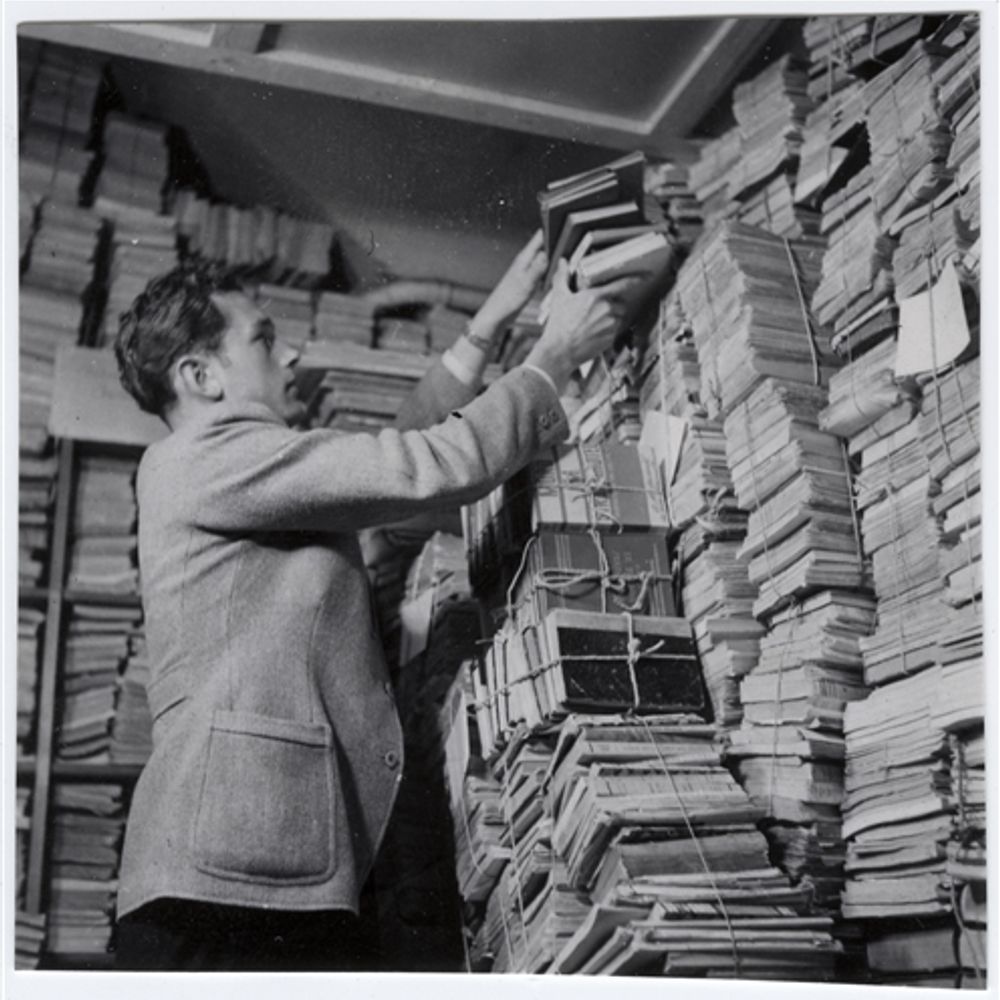
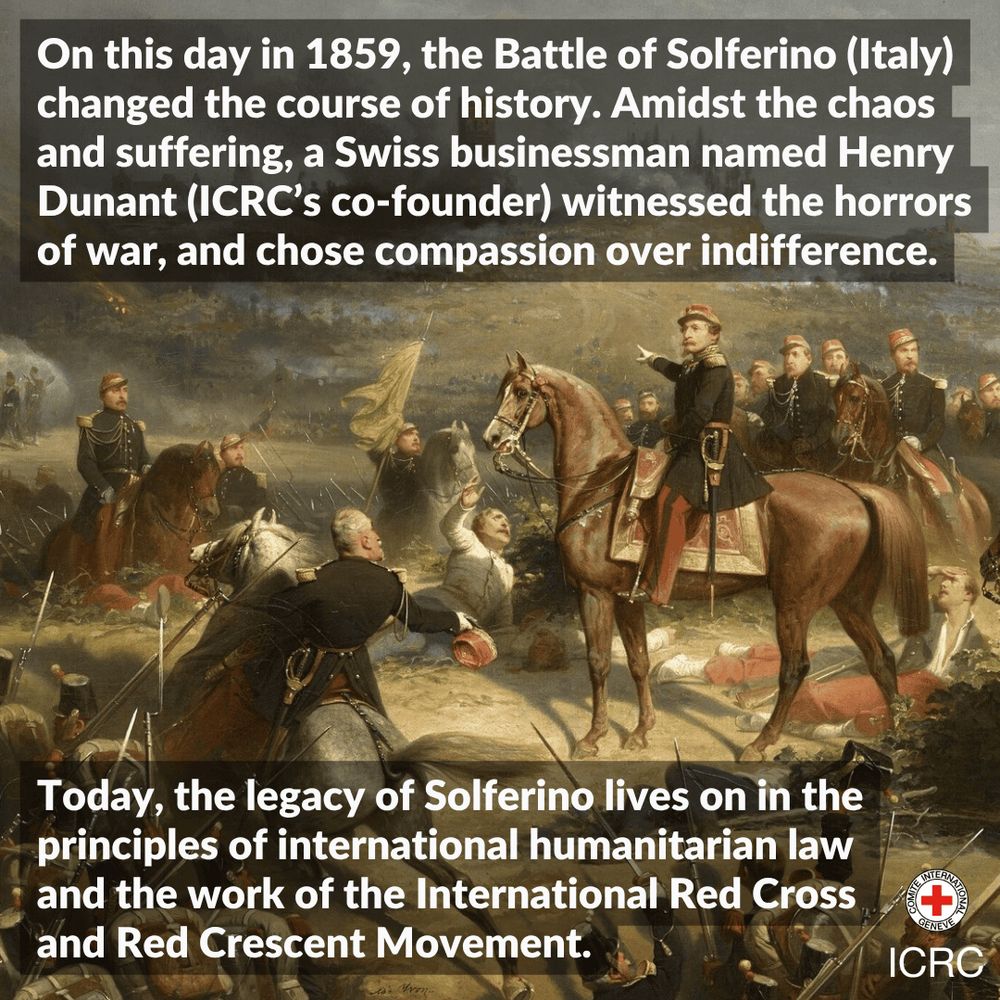
On June 24th 1859, Henry Dunant witnessed the horrors of the Battle of Solferino.
This inspired him to propose a treaty for armies to care for wounded soldiers & create national societies to support military medical services. In 1863, he co-founded the International Committee of the Red Cross 👇🏽
This inspired him to propose a treaty for armies to care for wounded soldiers & create national societies to support military medical services. In 1863, he co-founded the International Committee of the Red Cross 👇🏽
June 24, 2025 at 6:30 AM
On June 24th 1859, Henry Dunant witnessed the horrors of the Battle of Solferino.
This inspired him to propose a treaty for armies to care for wounded soldiers & create national societies to support military medical services. In 1863, he co-founded the International Committee of the Red Cross 👇🏽
This inspired him to propose a treaty for armies to care for wounded soldiers & create national societies to support military medical services. In 1863, he co-founded the International Committee of the Red Cross 👇🏽

The ICRC’s failures in Ukraine are a sobering reminder that humanitarian organisations must be held accountable when they fall short. Reform is urgently needed to prevent such lapses in future conflicts. 15/15
November 27, 2024 at 8:26 AM
The ICRC’s failures in Ukraine are a sobering reminder that humanitarian organisations must be held accountable when they fall short. Reform is urgently needed to prevent such lapses in future conflicts. 15/15

Great to meet with ICRC President Mirja Spoljaric to discuss humanitarian challenges in Palestine, Ukraine, and Sudan. Liechtenstein - ICRC's largest per capita donor- strongly supports its vital role in upholding international humanitarian law.

September 22, 2025 at 2:50 PM
Great to meet with ICRC President Mirja Spoljaric to discuss humanitarian challenges in Palestine, Ukraine, and Sudan. Liechtenstein - ICRC's largest per capita donor- strongly supports its vital role in upholding international humanitarian law.

Netanyahu spoke with Julien Lerisson, the ICRC’s regional coordinator
"The prime minister requested his involvement in providing food to our hostages and ensuring their immediate medical treatment,"
www.livemint.com/news/world/i...
"The prime minister requested his involvement in providing food to our hostages and ensuring their immediate medical treatment,"
www.livemint.com/news/world/i...

Netanyahu urges Red Cross for help after disturbing Hamas hostage videos surface | Today News
Israeli PM Benjamin Netanyahu has urged the Red Cross to help deliver food and medical care to hostages in Gaza after disturbing videos showed two captives, Rom Braslavski and Evyatar David, in severe...
www.livemint.com
August 4, 2025 at 11:10 AM
Netanyahu spoke with Julien Lerisson, the ICRC’s regional coordinator
"The prime minister requested his involvement in providing food to our hostages and ensuring their immediate medical treatment,"
www.livemint.com/news/world/i...
"The prime minister requested his involvement in providing food to our hostages and ensuring their immediate medical treatment,"
www.livemint.com/news/world/i...

The ICRC’s media chief addressed what they’re doing about the hostages (seeking access and release) in this MSNBC interview from a couple days ago. www.youtube.com/watch?v=Tk2T...

Honestly asking, and happy to be pointed to sources.
What did the ICRC do so far to make sure Israeli hostages in Gaza are being treated properly?
What did the ICRC do so far to make sure Israeli hostages in Gaza are being treated properly?
November 5, 2023 at 9:45 PM
The ICRC’s media chief addressed what they’re doing about the hostages (seeking access and release) in this MSNBC interview from a couple days ago. www.youtube.com/watch?v=Tk2T...

Humbled to be here. @icrc.org President Mirjana Spoljaric welcomed our director today. A strong reminder that International Humanitarian Law underpins the conventions prohibiting anti-personal landmines & Cluster Munitions–protecting lives during & long after conflict. Grateful for ICRC’s vital work



February 17, 2025 at 4:52 PM
Humbled to be here. @icrc.org President Mirjana Spoljaric welcomed our director today. A strong reminder that International Humanitarian Law underpins the conventions prohibiting anti-personal landmines & Cluster Munitions–protecting lives during & long after conflict. Grateful for ICRC’s vital work
Every day, detainees around the world face abuse and poor conditions, among others. In 2024, we worked in 67 contexts to ensure humane treatment, thanks to our neutral, humanitarian mandate.
Learn more about our work in detention: ms.spr.ly/63327sBI2W
#MandelaDay
Learn more about our work in detention: ms.spr.ly/63327sBI2W
#MandelaDay

July 18, 2025 at 2:17 PM
Every day, detainees around the world face abuse and poor conditions, among others. In 2024, we worked in 67 contexts to ensure humane treatment, thanks to our neutral, humanitarian mandate.
Learn more about our work in detention: ms.spr.ly/63327sBI2W
#MandelaDay
Learn more about our work in detention: ms.spr.ly/63327sBI2W
#MandelaDay
Under the rules of war, parties to conflicts must help families find answers about missing loved ones.
@corduladroege.bsky.social, ICRC's chief legal officer, explains what this means in practical terms for families 👇🏽
@corduladroege.bsky.social, ICRC's chief legal officer, explains what this means in practical terms for families 👇🏽
April 24, 2025 at 5:30 PM
Under the rules of war, parties to conflicts must help families find answers about missing loved ones.
@corduladroege.bsky.social, ICRC's chief legal officer, explains what this means in practical terms for families 👇🏽
@corduladroege.bsky.social, ICRC's chief legal officer, explains what this means in practical terms for families 👇🏽

In an interview at the ICRC's headquarters in Geneva, the organisation's president Mirjana Spoljaric said "humanity is failing" as it watched the horrors of the Gaza war.
Gaza has become worse than hell on earth, the head of the International Committee of the Red Cross (ICRC) has told the BBC.
www.bbc.com/news/article...
www.bbc.com/news/article...

Gaza now worse than hell on earth, humanitarian chief tells BBC
The situation in Gaza surpasses "any acceptable, legal, moral, and humane standard", the ICRC tells BBC's Jeremy Bowen.
www.bbc.com
June 5, 2025 at 1:21 PM
In an interview at the ICRC's headquarters in Geneva, the organisation's president Mirjana Spoljaric said "humanity is failing" as it watched the horrors of the Gaza war.