



Matt Fiedler
@mattafiedler.bsky.social
Senior Fellow, Center on Health Policy, The Brookings Institution. Former Chief Economist for Council of Economic Advisers.
Details are in the paper, but this figure shows the main results: across a wide range of assumptions about who “switchers” are (reflected in the different values of theta), changes in MA penetration have little effect on the degree of favorable selection into MA.

October 10, 2025 at 1:57 PM
Details are in the paper, but this figure shows the main results: across a wide range of assumptions about who “switchers” are (reflected in the different values of theta), changes in MA penetration have little effect on the degree of favorable selection into MA.
Indeed, it’s notable that *changes* in MA penetration are associated with modest declines in stayer-switcher differences, consistent with the concern that cross-sectional relationships are confounded to some degree.

October 10, 2025 at 1:57 PM
Indeed, it’s notable that *changes* in MA penetration are associated with modest declines in stayer-switcher differences, consistent with the concern that cross-sectional relationships are confounded to some degree.
Prior work has examined the cross-sectional relationship between MA penetration and stayer-switcher differences in risk-adjusted costs, finding little relationship. We replicate that finding:

October 10, 2025 at 1:57 PM
Prior work has examined the cross-sectional relationship between MA penetration and stayer-switcher differences in risk-adjusted costs, finding little relationship. We replicate that finding:
As illustrated in the figure below, the *gap* between the average cost of MA and TM enrollees can either grow or shrink as MA gets larger, depending on the exact shape of the relationship between beneficiary cost and propensity to enroll in MA vs. TM.

October 10, 2025 at 1:57 PM
As illustrated in the figure below, the *gap* between the average cost of MA and TM enrollees can either grow or shrink as MA gets larger, depending on the exact shape of the relationship between beneficiary cost and propensity to enroll in MA vs. TM.
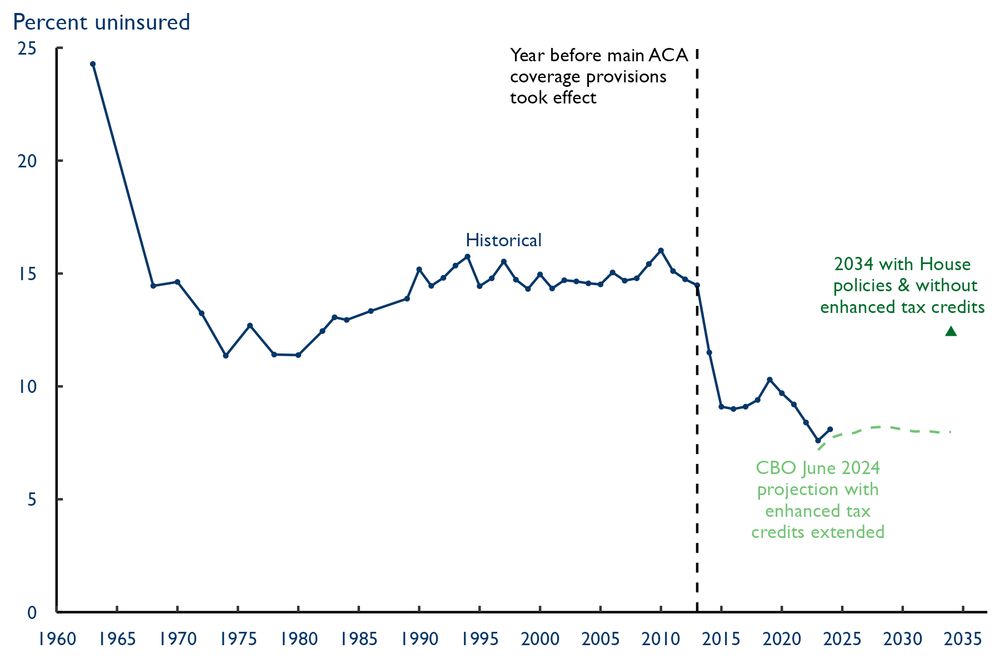
What will the Senate bill mean for health coverage? We don’t yet have final CBO estimates, but it’s clear they’ll be pretty similar to the House bill. That puts the U.S. on track for an unprecedented increase in the uninsured rate that will wipe out ~3/4 of post-2013 declines.
July 1, 2025 at 5:10 PM
What will the Senate bill mean for health coverage? We don’t yet have final CBO estimates, but it’s clear they’ll be pretty similar to the House bill. That puts the U.S. on track for an unprecedented increase in the uninsured rate that will wipe out ~3/4 of post-2013 declines.
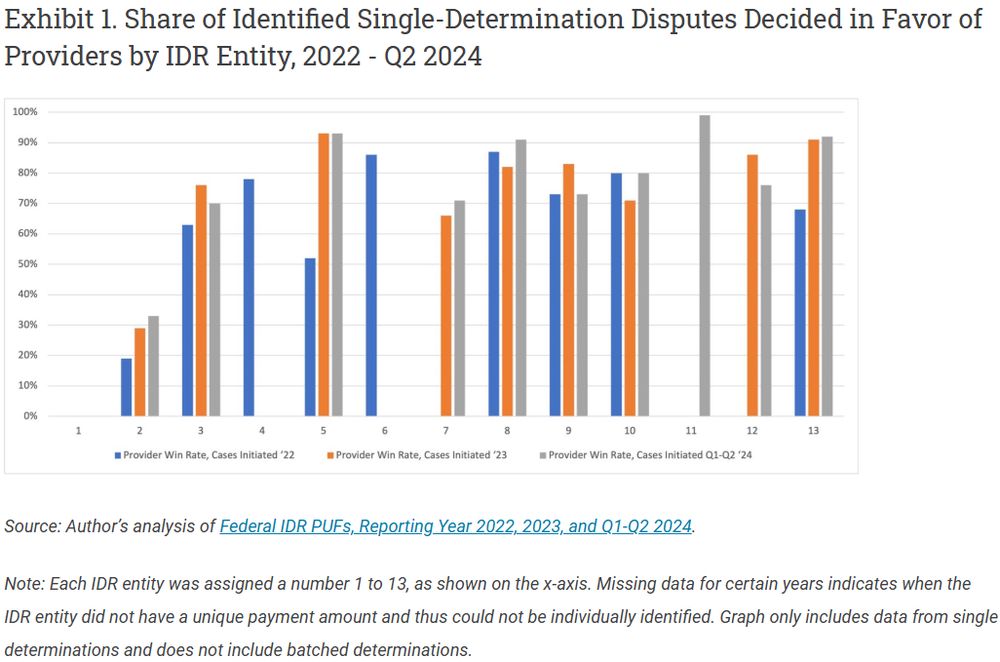
Clever new piece from Kennah Watts and Jack Hoadley takes a first look at how decisions under the No Surprises Act arbitration process vary across arbitrators. Lots of interesting findings here, including that provider win rates vary a lot by arbitrator.
June 25, 2025 at 1:18 PM
Clever new piece from Kennah Watts and Jack Hoadley takes a first look at how decisions under the No Surprises Act arbitration process vary across arbitrators. Lots of interesting findings here, including that provider win rates vary a lot by arbitrator.
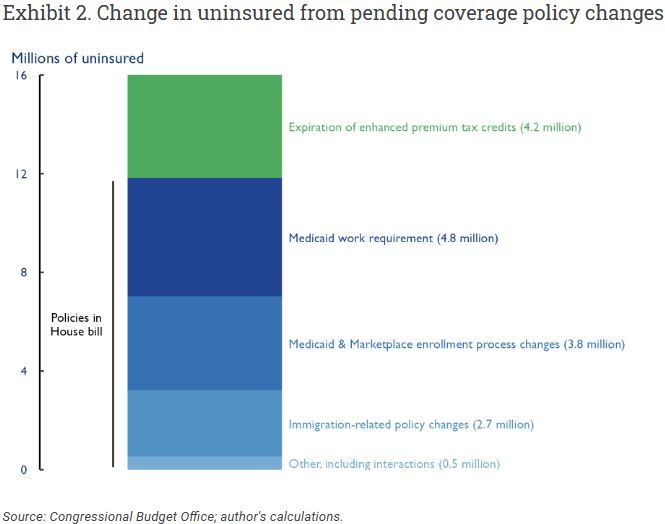
If lawmakers want to change the House bill to avoid this, they’ll have to change the provisions with big coverage impacts. Notably, the bill's provider tax changes, which seem to be attracting the most ire from Senators so far, are a fairly small part of the overall picture.
June 10, 2025 at 4:57 PM
If lawmakers want to change the House bill to avoid this, they’ll have to change the provisions with big coverage impacts. Notably, the bill's provider tax changes, which seem to be attracting the most ire from Senators so far, are a fairly small part of the overall picture.
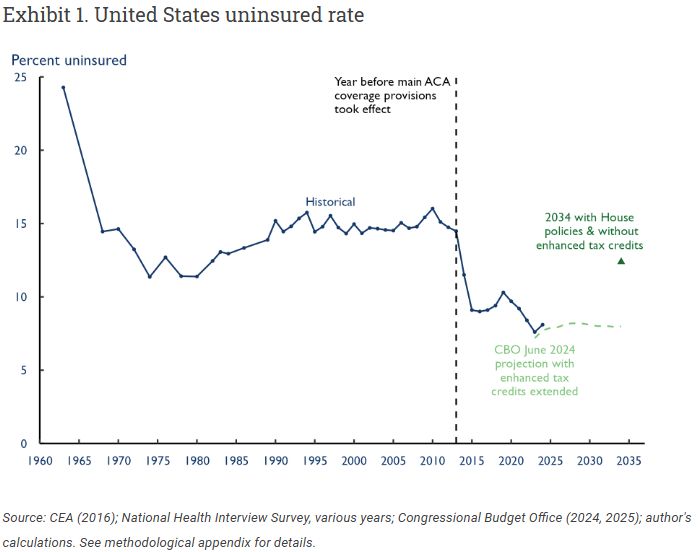
My new piece @healthaffairs.bsky.social Forefront finds that if the House bill becomes law and enhanced premium tax credits expire on schedule, the US will see an unprecedented increase in the uninsured rate, wiping out about ~3/4 of the post-2013 decline.
June 10, 2025 at 4:57 PM
My new piece @healthaffairs.bsky.social Forefront finds that if the House bill becomes law and enhanced premium tax credits expire on schedule, the US will see an unprecedented increase in the uninsured rate, wiping out about ~3/4 of the post-2013 decline.
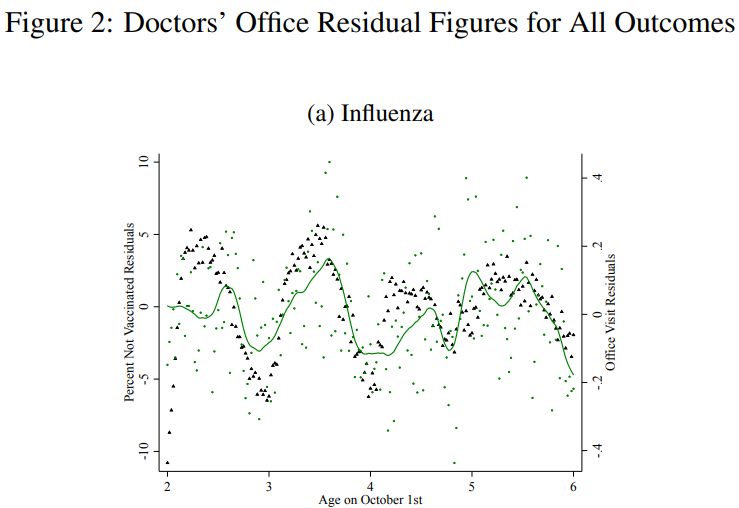
The authors then show that fall birthdays are, correspondingly, least likely to have a doctor’s office or emergency department visit for flu (green line/dots), indicating that higher vaccination rates do indeed translate into greater protection against flu.

May 27, 2025 at 3:22 PM
The authors then show that fall birthdays are, correspondingly, least likely to have a doctor’s office or emergency department visit for flu (green line/dots), indicating that higher vaccination rates do indeed translate into greater protection against flu.
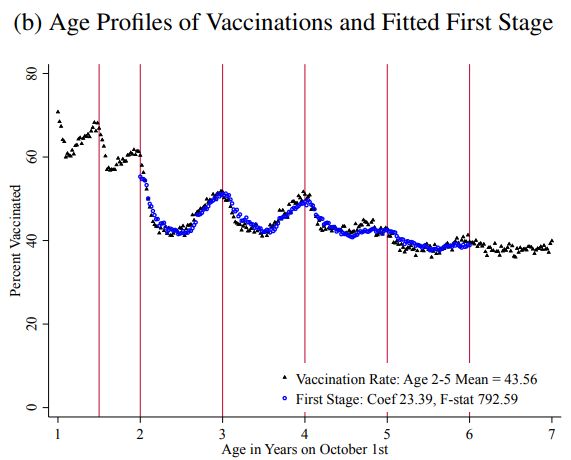
The authors leverage the fact that kids typically have a wellness visit around their birthday. For fall birthdays, the flu vaccine is typically available at that visit, resulting in higher vaccination rates than for kids a bit older/younger, esp. around 3rd & 4th birthdays.
May 27, 2025 at 3:22 PM
The authors leverage the fact that kids typically have a wellness visit around their birthday. For fall birthdays, the flu vaccine is typically available at that visit, resulting in higher vaccination rates than for kids a bit older/younger, esp. around 3rd & 4th birthdays.
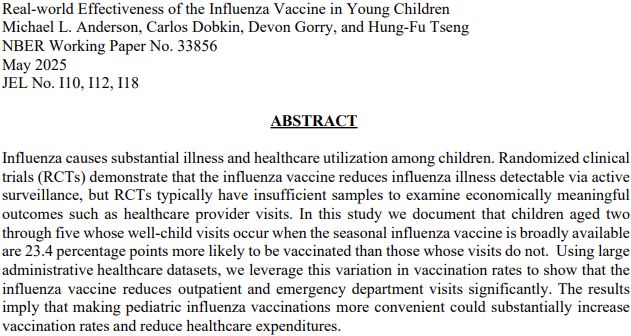
Interesting new paper providing clear evidence that the flu vaccine is effective at reducing both office and emergency department visits for flu in kids.
May 27, 2025 at 3:22 PM
Interesting new paper providing clear evidence that the flu vaccine is effective at reducing both office and emergency department visits for flu in kids.
The updated reconciliation language doubles down on the bill’s Marketplace cuts by ending “silver loading” for the 2026 plan year. This would greatly increase many Marketplace enrollees’ premiums, compounding increases due to expiration of enhanced tax credits.

May 22, 2025 at 1:32 AM
The updated reconciliation language doubles down on the bill’s Marketplace cuts by ending “silver loading” for the 2026 plan year. This would greatly increase many Marketplace enrollees’ premiums, compounding increases due to expiration of enhanced tax credits.
A final caveat is that I project long-term outcomes by using data from the 9 months Arkansas’ policy was in effect to fit a structural model of the underlying dynamics. That’s necessarily an uncertain exercise, although sensitivity analyses all show large enrollment declines.

April 30, 2025 at 6:47 PM
A final caveat is that I project long-term outcomes by using data from the 9 months Arkansas’ policy was in effect to fit a structural model of the underlying dynamics. That’s necessarily an uncertain exercise, although sensitivity analyses all show large enrollment declines.
The paper offers a lengthy discussion of how outcomes under an Arkansas-like federal policy might differ from outcomes in Arkansas, whether due to differences in state choices or circumstances. The short version is that there are factors cutting in both directions.


April 30, 2025 at 6:47 PM
The paper offers a lengthy discussion of how outcomes under an Arkansas-like federal policy might differ from outcomes in Arkansas, whether due to differences in state choices or circumstances. The short version is that there are factors cutting in both directions.
How would a federal Medicaid work requirement affect enrollment?
My new paper looks back at an Arkansas requirement very similar to one the House passed in 2023.
I estimate an Arkansas-like policy would reduce Medicaid enrollment for ppl subject to it by 34% in the long run:
My new paper looks back at an Arkansas requirement very similar to one the House passed in 2023.
I estimate an Arkansas-like policy would reduce Medicaid enrollment for ppl subject to it by 34% in the long run:

April 30, 2025 at 6:47 PM
How would a federal Medicaid work requirement affect enrollment?
My new paper looks back at an Arkansas requirement very similar to one the House passed in 2023.
I estimate an Arkansas-like policy would reduce Medicaid enrollment for ppl subject to it by 34% in the long run:
My new paper looks back at an Arkansas requirement very similar to one the House passed in 2023.
I estimate an Arkansas-like policy would reduce Medicaid enrollment for ppl subject to it by 34% in the long run:
An added wrinkle is that calibrating using the encounter data likely “turns off” the statutory requirement to make a coding pattern adjustment (and the associated statutory minimum adjustment), which could make it harder for CMS to apply an adequate adjustment.

February 13, 2025 at 3:01 PM
An added wrinkle is that calibrating using the encounter data likely “turns off” the statutory requirement to make a coding pattern adjustment (and the associated statutory minimum adjustment), which could make it harder for CMS to apply an adequate adjustment.
The appropriate coding pattern adjustment could change, but it’s unclear if it would get larger or smaller. That hinges on whether the beneficiaries who are “upcoded” in MA are relatively high spenders or relatively low spenders (see two scenarios below).


February 13, 2025 at 3:01 PM
The appropriate coding pattern adjustment could change, but it’s unclear if it would get larger or smaller. That hinges on whether the beneficiaries who are “upcoded” in MA are relatively high spenders or relatively low spenders (see two scenarios below).
In the 2026 MA Advance Notice, CMS said that it may begin calibrating the MA risk adjustment model using encounter data (snippet below). Unfortunately, this change would not achieve what CMS hopes it would—and might well be a step in the wrong direction.

February 13, 2025 at 3:01 PM
In the 2026 MA Advance Notice, CMS said that it may begin calibrating the MA risk adjustment model using encounter data (snippet below). Unfortunately, this change would not achieve what CMS hopes it would—and might well be a step in the wrong direction.
We also find that CMS could make its estimates more accurate for these counties by: (1) improving how it ensures credibility adjustments are budget neutral; and (2) changing how it sets the weight on the county’s own estimate vs. its region (see figure).

January 9, 2025 at 3:24 PM
We also find that CMS could make its estimates more accurate for these counties by: (1) improving how it ensures credibility adjustments are budget neutral; and (2) changing how it sets the weight on the county’s own estimate vs. its region (see figure).
However, for these counties, the total error in CMS’ estimates when accounting for this non-sampling error is (light blue line) is meaningfully greater than sampling error alone (dashed dark blue line), as counties do typically differ from their regions.

January 9, 2025 at 3:24 PM
However, for these counties, the total error in CMS’ estimates when accounting for this non-sampling error is (light blue line) is meaningfully greater than sampling error alone (dashed dark blue line), as counties do typically differ from their regions.
This non-sampling error is of limited importance in the aggregate since only 2.2% of beneficiaries live in counties subject to credibility adjustments even in our lowest-enrollment scenario.

January 9, 2025 at 3:24 PM
This non-sampling error is of limited importance in the aggregate since only 2.2% of beneficiaries live in counties subject to credibility adjustments even in our lowest-enrollment scenario.
We then estimate the standard error of CMS’ TM cost estimates in three enrollment scenarios (2022 + two 2033 scenarios). The median beneficiary is in a county where the standard error is 0.7% of TM costs or less; for the 95th percentile beneficiary, this is 2.4% or less.

January 9, 2025 at 3:24 PM
We then estimate the standard error of CMS’ TM cost estimates in three enrollment scenarios (2022 + two 2033 scenarios). The median beneficiary is in a county where the standard error is 0.7% of TM costs or less; for the 95th percentile beneficiary, this is 2.4% or less.
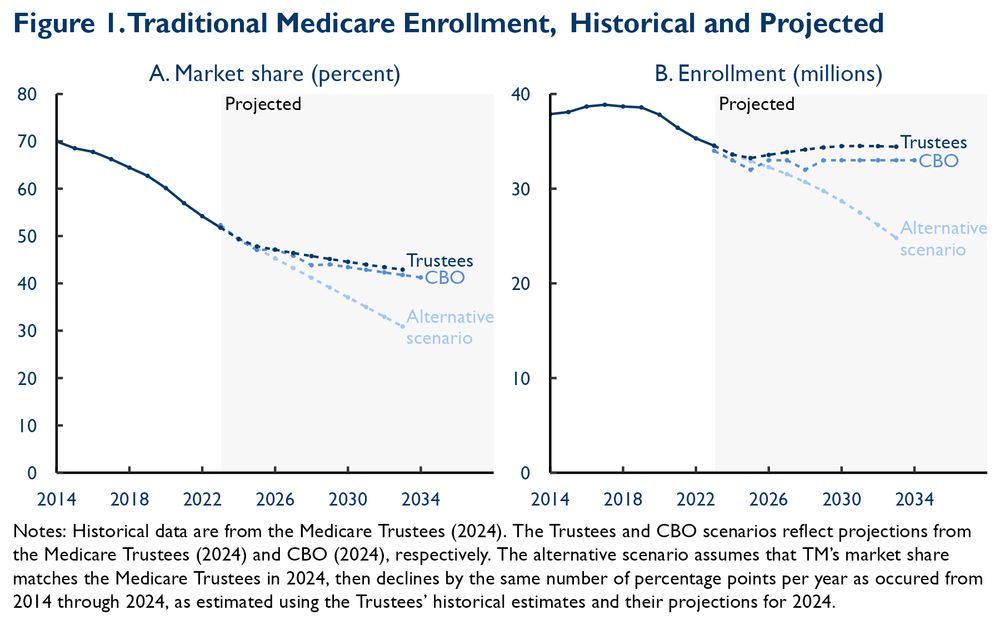
The amount of sampling error in estimates of local TM costs depends on TM enrollment, so we start with TM enrollment forecasts. CBO and the Trustees project roughly flat TM enrollment, with falling TM market share offset by rising total Medicare enrollment.
January 9, 2025 at 3:24 PM
The amount of sampling error in estimates of local TM costs depends on TM enrollment, so we start with TM enrollment forecasts. CBO and the Trustees project roughly flat TM enrollment, with falling TM market share offset by rising total Medicare enrollment.
How much do nongroup plans pay providers? Really enjoyed this new paper from Hanson et al. that finally offers a good answer. Short answer: less than group plans, but a lot more than Medicare.
Link: www.healthaffairs.org/doi/full/10....
Link: www.healthaffairs.org/doi/full/10....

November 21, 2024 at 9:32 PM
How much do nongroup plans pay providers? Really enjoyed this new paper from Hanson et al. that finally offers a good answer. Short answer: less than group plans, but a lot more than Medicare.
Link: www.healthaffairs.org/doi/full/10....
Link: www.healthaffairs.org/doi/full/10....