



Josh Leisring
@joshleisring.bsky.social
Nephrologist / Hypertension Specialist in Columbus, Ohio
#Nephsky
He / him
#Nephsky
He / him

At our center we do the initial screen without altering the existing meds. Don’t wanna miss the opportunity. Patients with the most overt PA have suppressed renin even on RAASi+thiazide. If results aren’t conclusive and suspicion still there can then washout or try empiric MRA. #NephJC

September 18, 2025 at 3:55 AM
At our center we do the initial screen without altering the existing meds. Don’t wanna miss the opportunity. Patients with the most overt PA have suppressed renin even on RAASi+thiazide. If results aren’t conclusive and suspicion still there can then washout or try empiric MRA. #NephJC
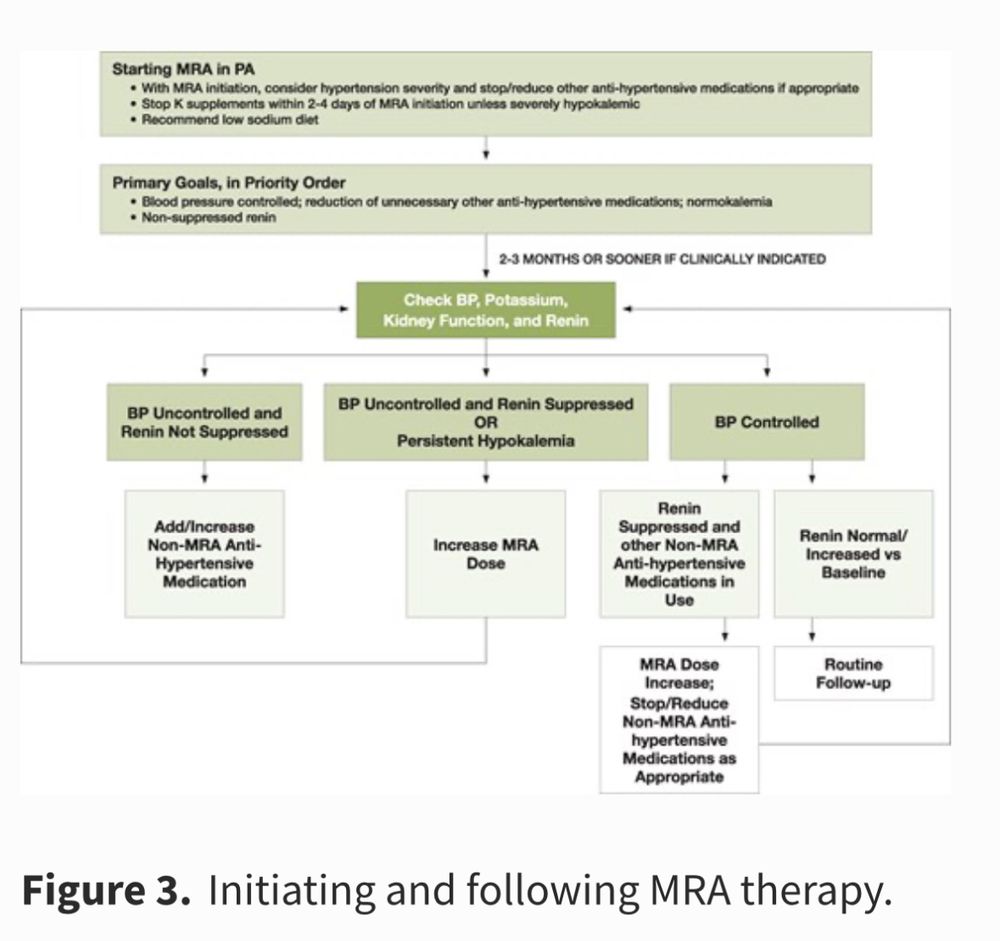
Implementing will be a challenge but that shouldn't discourage broader screening.
From the recent Endo Society guideline - the majority of these newly detected cases can be managed with MRA.
From the recent Endo Society guideline - the majority of these newly detected cases can be managed with MRA.

August 15, 2025 at 7:59 PM
Implementing will be a challenge but that shouldn't discourage broader screening.
From the recent Endo Society guideline - the majority of these newly detected cases can be managed with MRA.
From the recent Endo Society guideline - the majority of these newly detected cases can be managed with MRA.
Commentary on expanded screening for primary aldosteronism in the new HTN guideline.
www.ahajournals.org/doi/10.1161/... 🔓
www.ahajournals.org/doi/10.1161/... 🔓


August 15, 2025 at 7:56 PM
Commentary on expanded screening for primary aldosteronism in the new HTN guideline.
www.ahajournals.org/doi/10.1161/... 🔓
www.ahajournals.org/doi/10.1161/... 🔓
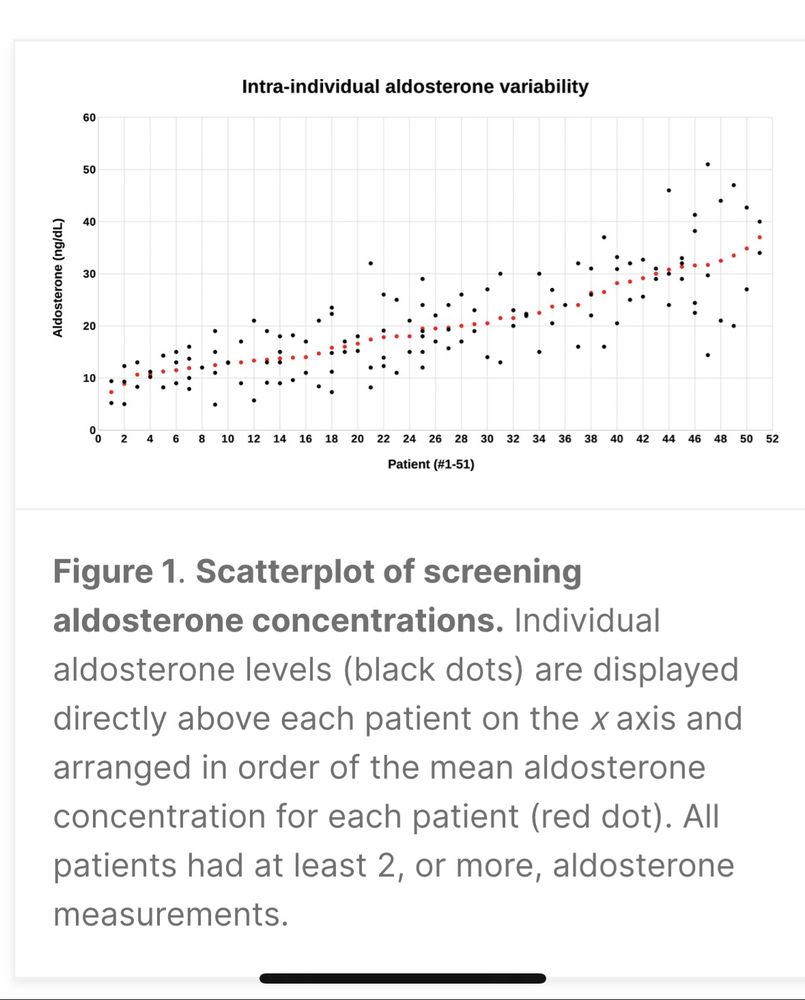
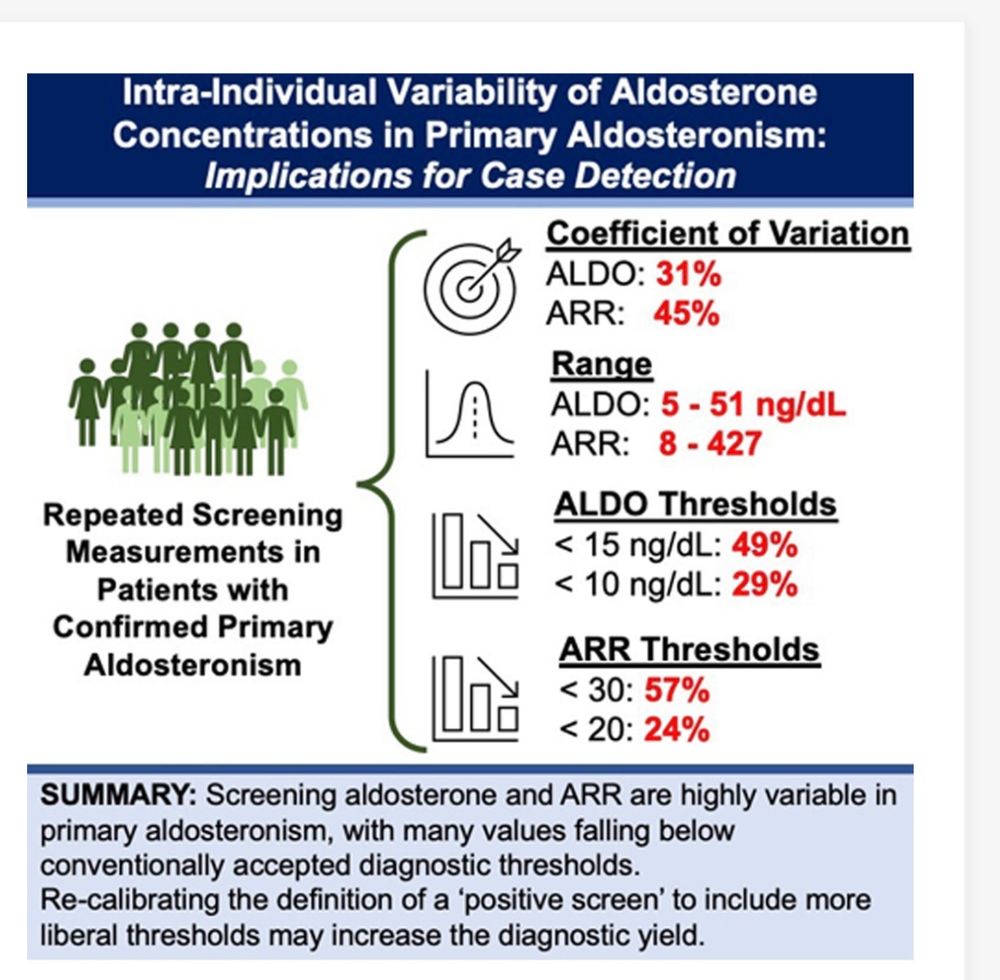
1/ Even outside of AVS the intra-individual variability of plasma aldo is important. Another study with the same message. www.ahajournals.org/doi/10.1161/...
July 28, 2025 at 9:27 PM
1/ Even outside of AVS the intra-individual variability of plasma aldo is important. Another study with the same message. www.ahajournals.org/doi/10.1161/...
Agree that the most spironolactone-responsive cases of RHTN are on that spectrum of PA. I have used a similar approach and this practice, along with monitoring for an increase in renin, has been adapted in the new Endo society guideline.
July 15, 2025 at 9:51 PM
Agree that the most spironolactone-responsive cases of RHTN are on that spectrum of PA. I have used a similar approach and this practice, along with monitoring for an increase in renin, has been adapted in the new Endo society guideline.
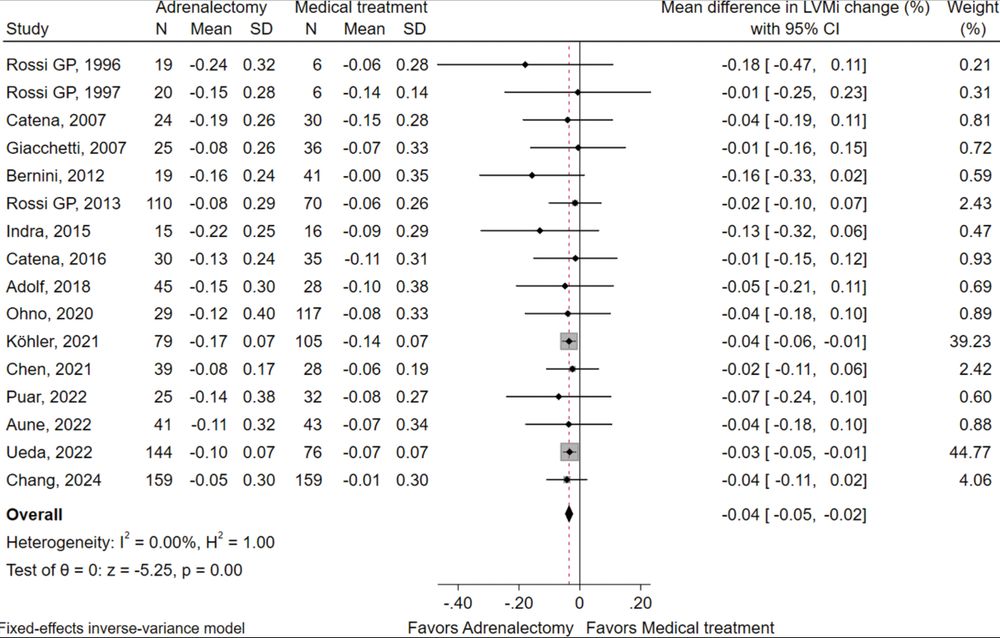
Should adrenalectomy still be first-line treatment of unilateral PA?
▶️adrenalectomy associates with greater decrease in LVM despite similar BP
▶️shorter duration of HTN associates with greater benefit after surgery
▶️high 24hr urine Na negatively impacts benefit of MRA
tiny.cc/jf2o001 🔒
#nephsky
▶️adrenalectomy associates with greater decrease in LVM despite similar BP
▶️shorter duration of HTN associates with greater benefit after surgery
▶️high 24hr urine Na negatively impacts benefit of MRA
tiny.cc/jf2o001 🔒
#nephsky
June 27, 2025 at 12:29 AM
Should adrenalectomy still be first-line treatment of unilateral PA?
▶️adrenalectomy associates with greater decrease in LVM despite similar BP
▶️shorter duration of HTN associates with greater benefit after surgery
▶️high 24hr urine Na negatively impacts benefit of MRA
tiny.cc/jf2o001 🔒
#nephsky
▶️adrenalectomy associates with greater decrease in LVM despite similar BP
▶️shorter duration of HTN associates with greater benefit after surgery
▶️high 24hr urine Na negatively impacts benefit of MRA
tiny.cc/jf2o001 🔒
#nephsky
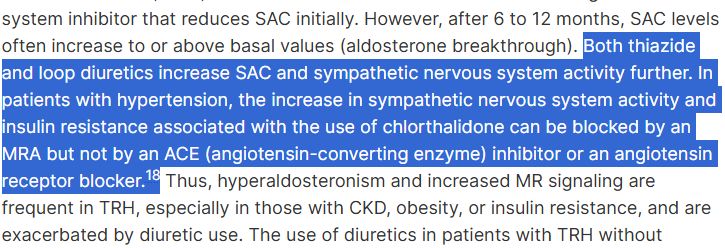
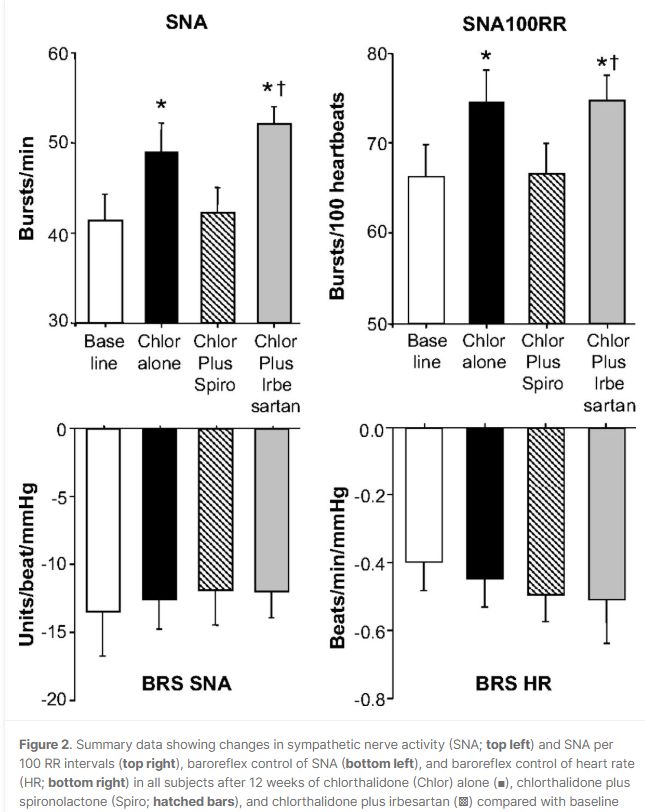
3/ I was interested to learn about the modulatory effect that spiro has on CTD-related sympathetic activation and insulin resistance. Maybe there is some specific benefit in adding MRA to thiazide. Just not sure if it’s directly related to blocking aldosterone. (Figure from the referenced study.)
May 30, 2025 at 8:38 PM
3/ I was interested to learn about the modulatory effect that spiro has on CTD-related sympathetic activation and insulin resistance. Maybe there is some specific benefit in adding MRA to thiazide. Just not sure if it’s directly related to blocking aldosterone. (Figure from the referenced study.)
2/ Is secondary (renin-angiotensin-dependent) hyperaldosteronism occurring secondary to diuretics / sodium depletion analogous to physiologic hyperaldosteronism seen with very low Na diet? I don't know.
May 30, 2025 at 8:34 PM
2/ Is secondary (renin-angiotensin-dependent) hyperaldosteronism occurring secondary to diuretics / sodium depletion analogous to physiologic hyperaldosteronism seen with very low Na diet? I don't know.
1/ Interesting read. The conclusion to use MRAs (or maybe ASIs) sooner makes sense to me. But is the main benefit just due to the high prevalence of primary aldosteronism, rather than in offsetting the secondary aldosteronism that accompanies thiazides? #nephsky #cardiosky #endosky #medsky


May 30, 2025 at 8:33 PM
1/ Interesting read. The conclusion to use MRAs (or maybe ASIs) sooner makes sense to me. But is the main benefit just due to the high prevalence of primary aldosteronism, rather than in offsetting the secondary aldosteronism that accompanies thiazides? #nephsky #cardiosky #endosky #medsky
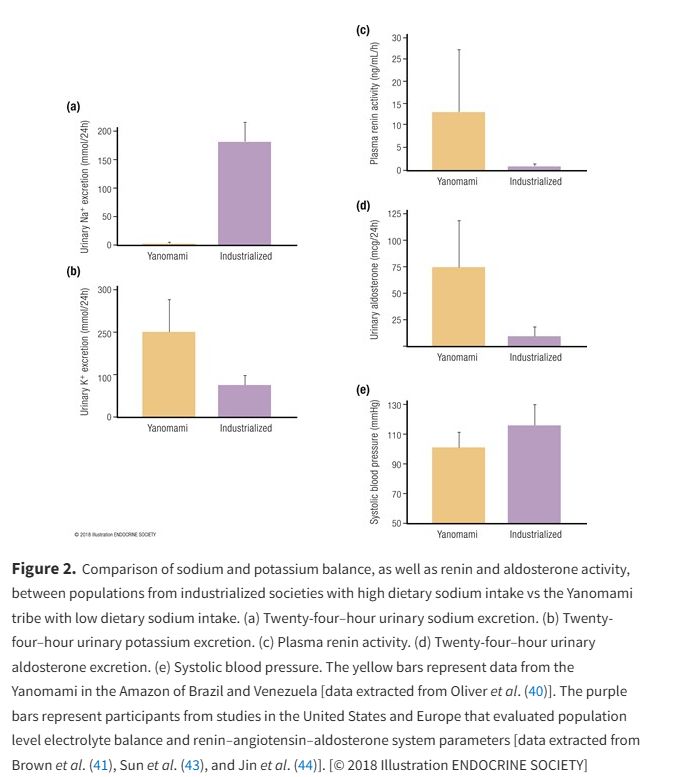
And a more visually agreeable figure from an excellent review article from @anandvaidya17.bsky.social et al. academic.oup.com/edrv/article...

May 28, 2025 at 2:13 AM
And a more visually agreeable figure from an excellent review article from @anandvaidya17.bsky.social et al. academic.oup.com/edrv/article...
I can't this question, but it gives me a good excuse to mention the 1970s study by Oliver et al demonstrating that high levels of renin / aldosterone alone don't drive blood pressure. It's some combination of salt+RAAS+(?). pubmed.ncbi.nlm.nih.gov/1132118/ #NephJC


May 28, 2025 at 2:11 AM
I can't this question, but it gives me a good excuse to mention the 1970s study by Oliver et al demonstrating that high levels of renin / aldosterone alone don't drive blood pressure. It's some combination of salt+RAAS+(?). pubmed.ncbi.nlm.nih.gov/1132118/ #NephJC
Anecdotally I still find the switch useful in RHTN. Maybe just my⚓️ bias but most of the patients in that study did not have RHTN and were on lower doses of CTD than I typically use for RHTN. I'm open to being enlightend but for now... #nephmadness

March 5, 2025 at 1:39 AM
Anecdotally I still find the switch useful in RHTN. Maybe just my⚓️ bias but most of the patients in that study did not have RHTN and were on lower doses of CTD than I typically use for RHTN. I'm open to being enlightend but for now... #nephmadness
SGLT2i as well! Modest BP effect but bank on hard outcome data. Here is my rough draft of where they might fit (in red) into the RHTN treatment algorithm. From a talk to #OSUNephrology fellows just last week ! Would love feedback! #nephmadness @jordybc.bsky.social @stephanietr612.bsky.social

March 2, 2025 at 10:27 PM
SGLT2i as well! Modest BP effect but bank on hard outcome data. Here is my rough draft of where they might fit (in red) into the RHTN treatment algorithm. From a talk to #OSUNephrology fellows just last week ! Would love feedback! #nephmadness @jordybc.bsky.social @stephanietr612.bsky.social
I got a link to the new Endocrine Society guideline for primary aldosteronism (draft open for public comments).
www.surveymonkey.com/r/endopacpg
>Suggests screening all individuals with hypertension
>Proposes various strategies re: handling of confounding BP meds during testing
#NephJC #Nephsky
www.surveymonkey.com/r/endopacpg
>Suggests screening all individuals with hypertension
>Proposes various strategies re: handling of confounding BP meds during testing
#NephJC #Nephsky



February 26, 2025 at 1:51 PM
I got a link to the new Endocrine Society guideline for primary aldosteronism (draft open for public comments).
www.surveymonkey.com/r/endopacpg
>Suggests screening all individuals with hypertension
>Proposes various strategies re: handling of confounding BP meds during testing
#NephJC #Nephsky
www.surveymonkey.com/r/endopacpg
>Suggests screening all individuals with hypertension
>Proposes various strategies re: handling of confounding BP meds during testing
#NephJC #Nephsky
3/ Prognostic value of renin as a biomarker in pharmacologic treatment. In PA treated with MRA, non-suppressed renin status (PRA > 1) associates better CV outcomes independent of BP. (I think this is still up for debate, needs prospective data.) #NephJC
academic.oup.com/edrv/article...
academic.oup.com/edrv/article...

February 12, 2025 at 3:55 AM
3/ Prognostic value of renin as a biomarker in pharmacologic treatment. In PA treated with MRA, non-suppressed renin status (PRA > 1) associates better CV outcomes independent of BP. (I think this is still up for debate, needs prospective data.) #NephJC
academic.oup.com/edrv/article...
academic.oup.com/edrv/article...
Up for debate - from a reveiw from some of the authors of today's paper.
@jenifermbr.bsky.social @anandvaidya17.bsky.social
pmc.ncbi.nlm.nih.gov/articles/PMC...
#NephJC
@jenifermbr.bsky.social @anandvaidya17.bsky.social
pmc.ncbi.nlm.nih.gov/articles/PMC...
#NephJC

February 12, 2025 at 3:03 AM
Up for debate - from a reveiw from some of the authors of today's paper.
@jenifermbr.bsky.social @anandvaidya17.bsky.social
pmc.ncbi.nlm.nih.gov/articles/PMC...
#NephJC
@jenifermbr.bsky.social @anandvaidya17.bsky.social
pmc.ncbi.nlm.nih.gov/articles/PMC...
#NephJC
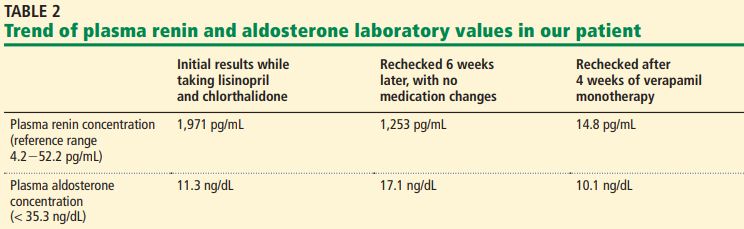
What's the highest renin you've ever seen?
An extreme example of a common issue. Severe hyperreninemia secondary to combination ARB+thiazide.
www.ccjm.org/content/91/2... (free)
@amyaimei.bsky.social
#medsky #nephsky
An extreme example of a common issue. Severe hyperreninemia secondary to combination ARB+thiazide.
www.ccjm.org/content/91/2... (free)
@amyaimei.bsky.social
#medsky #nephsky
February 2, 2025 at 4:36 AM
What's the highest renin you've ever seen?
An extreme example of a common issue. Severe hyperreninemia secondary to combination ARB+thiazide.
www.ccjm.org/content/91/2... (free)
@amyaimei.bsky.social
#medsky #nephsky
An extreme example of a common issue. Severe hyperreninemia secondary to combination ARB+thiazide.
www.ccjm.org/content/91/2... (free)
@amyaimei.bsky.social
#medsky #nephsky
Outstanding! Compare to primary aldosteronism:
->autonomous aldosterone
->excessive MR activation / ENaC
->distal Na reabsorption despite expanding CV
->renin/angII suppressed, no stimulus for proximal Na reabsorption
->greater Na delivery to ASDN
->inappropriate K excretion
tinyurl.com/3yd46a5c
->autonomous aldosterone
->excessive MR activation / ENaC
->distal Na reabsorption despite expanding CV
->renin/angII suppressed, no stimulus for proximal Na reabsorption
->greater Na delivery to ASDN
->inappropriate K excretion
tinyurl.com/3yd46a5c

February 2, 2025 at 4:22 AM
Outstanding! Compare to primary aldosteronism:
->autonomous aldosterone
->excessive MR activation / ENaC
->distal Na reabsorption despite expanding CV
->renin/angII suppressed, no stimulus for proximal Na reabsorption
->greater Na delivery to ASDN
->inappropriate K excretion
tinyurl.com/3yd46a5c
->autonomous aldosterone
->excessive MR activation / ENaC
->distal Na reabsorption despite expanding CV
->renin/angII suppressed, no stimulus for proximal Na reabsorption
->greater Na delivery to ASDN
->inappropriate K excretion
tinyurl.com/3yd46a5c