




Isaac Lamb, MD
@isaaclamb01.bsky.social
PGY-4 neurology resident. Interested in clinical neurology, medical education, history, and nerd stuff.
Should you close a PFO?
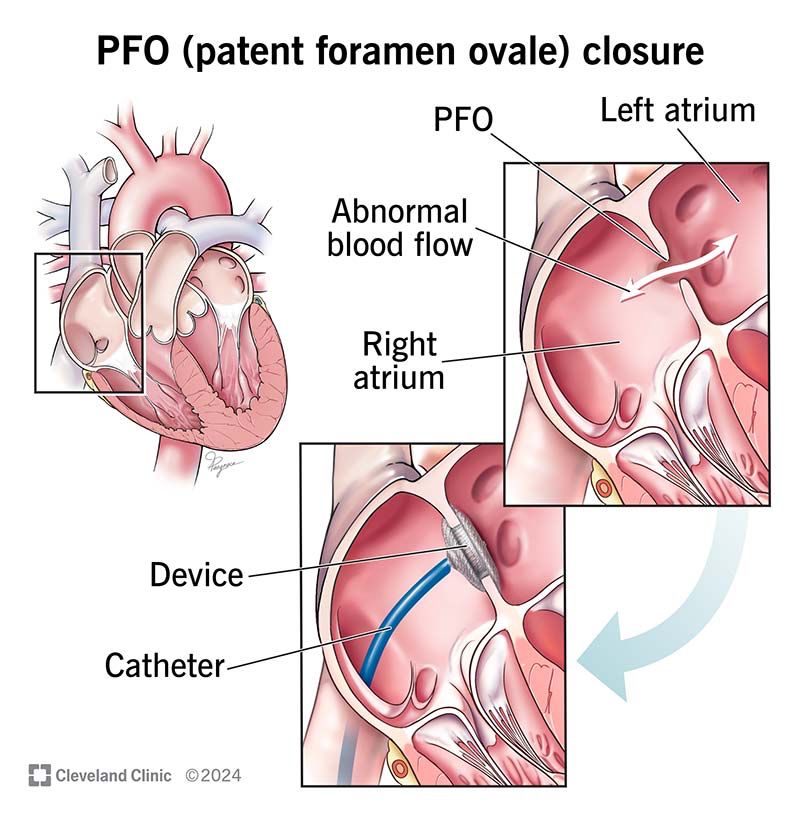
Not necessarily. About 20% of the population has a PFO. Most strokes, even in patients with a PFO, were probably from something else.
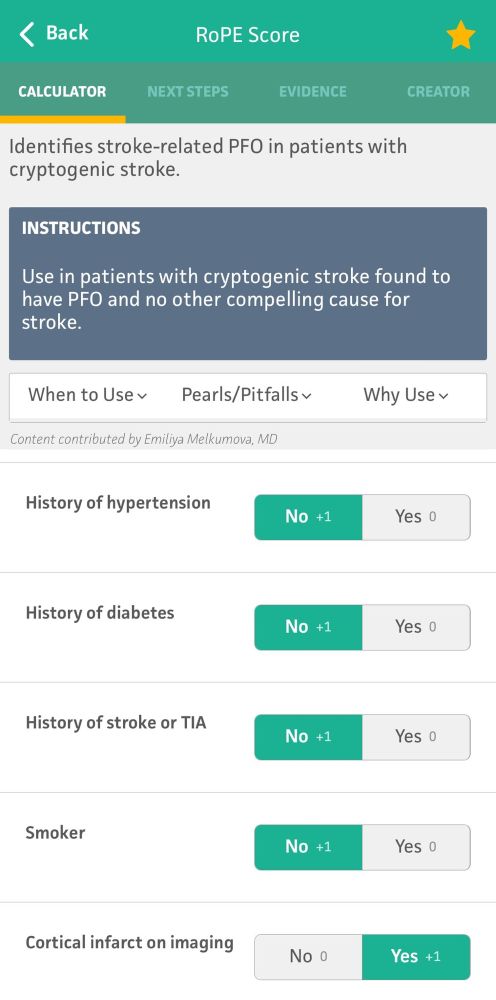
The decision to close one is based off of size, imaging, patient age and risk, and scoring tools (eg RoPE score).
Not necessarily. About 20% of the population has a PFO. Most strokes, even in patients with a PFO, were probably from something else.
The decision to close one is based off of size, imaging, patient age and risk, and scoring tools (eg RoPE score).
July 12, 2025 at 8:52 PM
Should you close a PFO?
Not necessarily. About 20% of the population has a PFO. Most strokes, even in patients with a PFO, were probably from something else.
The decision to close one is based off of size, imaging, patient age and risk, and scoring tools (eg RoPE score).
Not necessarily. About 20% of the population has a PFO. Most strokes, even in patients with a PFO, were probably from something else.
The decision to close one is based off of size, imaging, patient age and risk, and scoring tools (eg RoPE score).
TREATMENT
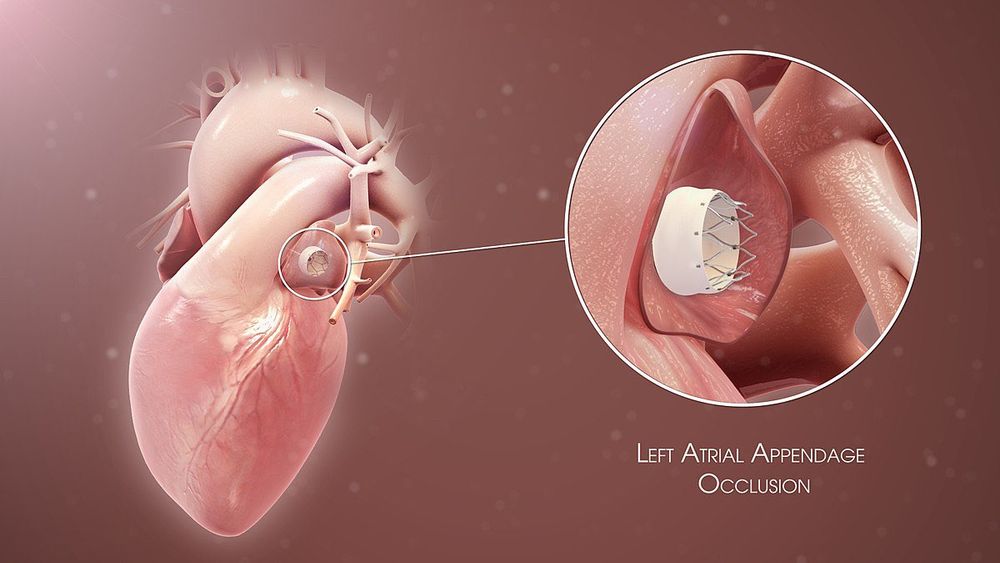
Most afib patients require chronic anticoagulation, and this is doubly true for stroke patients. Studies have shown superiority in DOACs (eg apixaban) over warfarin. If patients have contraindications to chronic AC, a LAA occlusive device gets almost the same benefit.
Most afib patients require chronic anticoagulation, and this is doubly true for stroke patients. Studies have shown superiority in DOACs (eg apixaban) over warfarin. If patients have contraindications to chronic AC, a LAA occlusive device gets almost the same benefit.
July 12, 2025 at 8:52 PM
TREATMENT
Most afib patients require chronic anticoagulation, and this is doubly true for stroke patients. Studies have shown superiority in DOACs (eg apixaban) over warfarin. If patients have contraindications to chronic AC, a LAA occlusive device gets almost the same benefit.
Most afib patients require chronic anticoagulation, and this is doubly true for stroke patients. Studies have shown superiority in DOACs (eg apixaban) over warfarin. If patients have contraindications to chronic AC, a LAA occlusive device gets almost the same benefit.
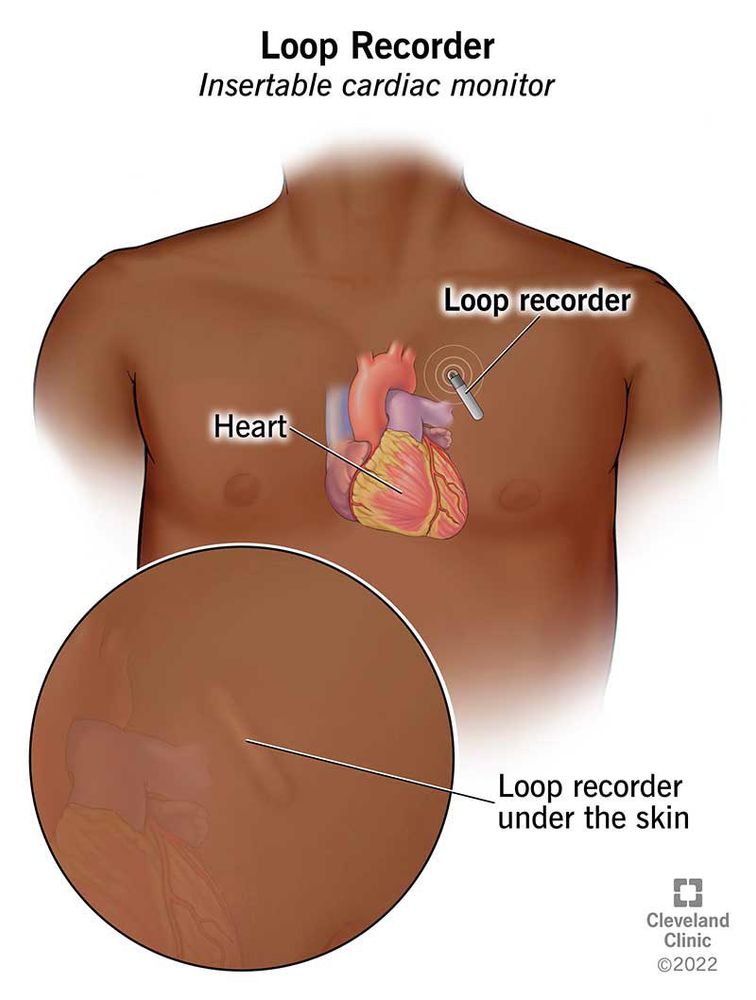
While we monitor all stroke patients while inpatient, statistically many cases of afib are paroxysmal and will be missed. We use a variety of ambulatory cardiac monitoring devices on discharge to improve sensitivity.

July 12, 2025 at 8:52 PM
While we monitor all stroke patients while inpatient, statistically many cases of afib are paroxysmal and will be missed. We use a variety of ambulatory cardiac monitoring devices on discharge to improve sensitivity.
While getting a TTE, we almost always inject agitated saline contrast to look for a PFO. If no PFO is seen, we can usually exclude paradoxical embolus. If we see one, we may have to go DVT hunting in the limbs and pelvis via ultrasound and/or MRV/CTV.
July 12, 2025 at 8:52 PM
While getting a TTE, we almost always inject agitated saline contrast to look for a PFO. If no PFO is seen, we can usually exclude paradoxical embolus. If we see one, we may have to go DVT hunting in the limbs and pelvis via ultrasound and/or MRV/CTV.
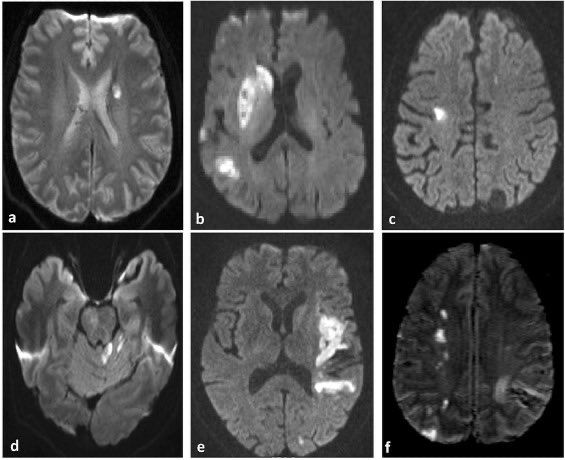
IMAGING
The thrombi from cardioembolic strokes are typically larger than atheroembolic strokes (see pt 1) meaning the strokes generally fall in large vessel territories (not lacunes).
The unique feature is that it can hit any vascular territory, left/right/anterior posterior.
The thrombi from cardioembolic strokes are typically larger than atheroembolic strokes (see pt 1) meaning the strokes generally fall in large vessel territories (not lacunes).
The unique feature is that it can hit any vascular territory, left/right/anterior posterior.
July 12, 2025 at 8:52 PM
IMAGING
The thrombi from cardioembolic strokes are typically larger than atheroembolic strokes (see pt 1) meaning the strokes generally fall in large vessel territories (not lacunes).
The unique feature is that it can hit any vascular territory, left/right/anterior posterior.
The thrombi from cardioembolic strokes are typically larger than atheroembolic strokes (see pt 1) meaning the strokes generally fall in large vessel territories (not lacunes).
The unique feature is that it can hit any vascular territory, left/right/anterior posterior.
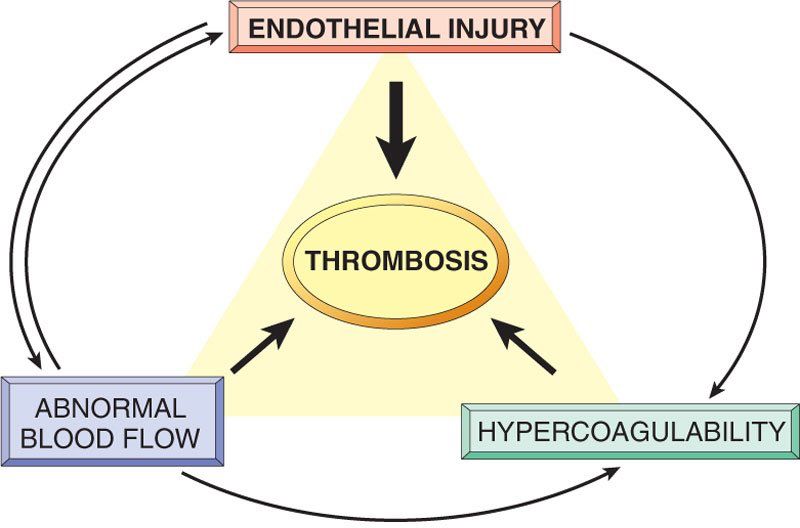
PATHOPHYSIOLOGY
Cardioembolic strokes are generally caused by the other two corners of Virchow’s triad: stasis (eg afib) and hypercoagulability (eg paradoxical embolus from a DVT). Overactivity of secondary coagulation results in a thrombus which can embolize.
Cardioembolic strokes are generally caused by the other two corners of Virchow’s triad: stasis (eg afib) and hypercoagulability (eg paradoxical embolus from a DVT). Overactivity of secondary coagulation results in a thrombus which can embolize.
July 12, 2025 at 8:52 PM
PATHOPHYSIOLOGY
Cardioembolic strokes are generally caused by the other two corners of Virchow’s triad: stasis (eg afib) and hypercoagulability (eg paradoxical embolus from a DVT). Overactivity of secondary coagulation results in a thrombus which can embolize.
Cardioembolic strokes are generally caused by the other two corners of Virchow’s triad: stasis (eg afib) and hypercoagulability (eg paradoxical embolus from a DVT). Overactivity of secondary coagulation results in a thrombus which can embolize.
Traditional vascular risk factor mitigation is crucial, most importantly diabetes and hypertension.
These patients are also treated with lifelong single antiplatelet therapy (remember Virchow’s triad).
DAPT has a slight benefit but only in the very short term (ie 21 days).
These patients are also treated with lifelong single antiplatelet therapy (remember Virchow’s triad).
DAPT has a slight benefit but only in the very short term (ie 21 days).
July 7, 2025 at 10:06 PM
Traditional vascular risk factor mitigation is crucial, most importantly diabetes and hypertension.
These patients are also treated with lifelong single antiplatelet therapy (remember Virchow’s triad).
DAPT has a slight benefit but only in the very short term (ie 21 days).
These patients are also treated with lifelong single antiplatelet therapy (remember Virchow’s triad).
DAPT has a slight benefit but only in the very short term (ie 21 days).
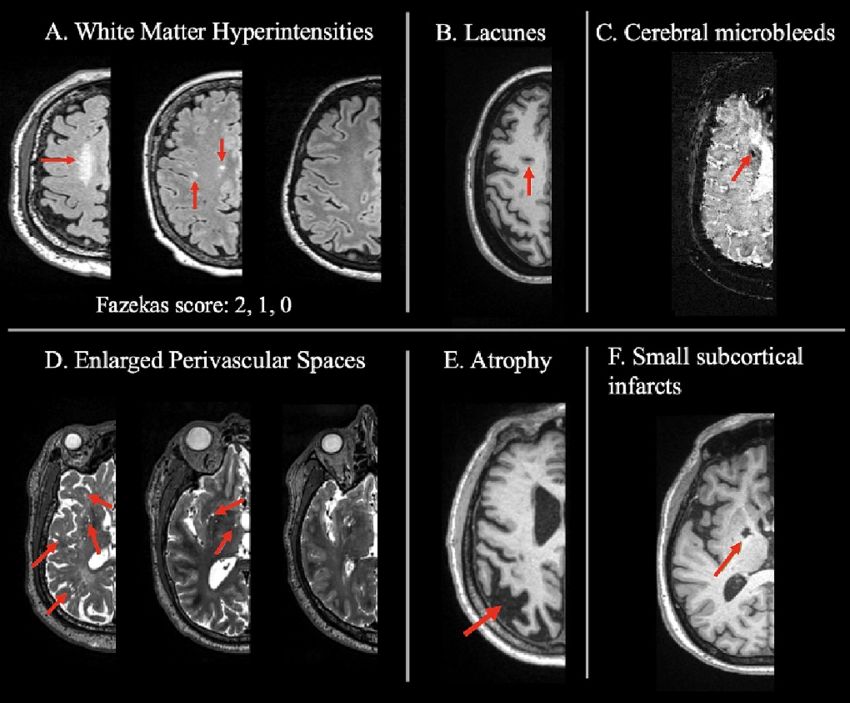
SVD leaves very classic imaging findings, making it easier to radiographically identify:
1. “Holes” of dead tissue (lacunes)
2. Enlarged perivascular spaces
3. White matter hyperintensities (on T2 weighted imaging)
These findings may be too subtle to pick up on CT, though.
1. “Holes” of dead tissue (lacunes)
2. Enlarged perivascular spaces
3. White matter hyperintensities (on T2 weighted imaging)
These findings may be too subtle to pick up on CT, though.
July 7, 2025 at 10:06 PM
SVD leaves very classic imaging findings, making it easier to radiographically identify:
1. “Holes” of dead tissue (lacunes)
2. Enlarged perivascular spaces
3. White matter hyperintensities (on T2 weighted imaging)
These findings may be too subtle to pick up on CT, though.
1. “Holes” of dead tissue (lacunes)
2. Enlarged perivascular spaces
3. White matter hyperintensities (on T2 weighted imaging)
These findings may be too subtle to pick up on CT, though.
Arteriosclerosis, though, is the more classic and traditional mechanism for small vessel strokes. Chronic exposure to high blood pressure causes vessel wall thickening and endothelial damage, which eventually causes distal occlusion.


July 7, 2025 at 10:06 PM
Arteriosclerosis, though, is the more classic and traditional mechanism for small vessel strokes. Chronic exposure to high blood pressure causes vessel wall thickening and endothelial damage, which eventually causes distal occlusion.
There are two major mechanisms for small vessel strokes:
1. Lipohyalinosis -> arteriosclerosis and occlusion
2. Branch atheroma with distal occlusion
The second is probable easier to understand: atheromatous disease can block off these branches at the proximal supply.
1. Lipohyalinosis -> arteriosclerosis and occlusion
2. Branch atheroma with distal occlusion
The second is probable easier to understand: atheromatous disease can block off these branches at the proximal supply.

July 7, 2025 at 10:06 PM
There are two major mechanisms for small vessel strokes:
1. Lipohyalinosis -> arteriosclerosis and occlusion
2. Branch atheroma with distal occlusion
The second is probable easier to understand: atheromatous disease can block off these branches at the proximal supply.
1. Lipohyalinosis -> arteriosclerosis and occlusion
2. Branch atheroma with distal occlusion
The second is probable easier to understand: atheromatous disease can block off these branches at the proximal supply.
PATHOPHYSIOLOGY
Small vessel occlusions refer to ischemic strokes impacting vessels too small to have names. These small perforating arteries are at right angles to larger vessels and primarily supply the basal ganglia, thalami, white matter, and brainstem.
Small vessel occlusions refer to ischemic strokes impacting vessels too small to have names. These small perforating arteries are at right angles to larger vessels and primarily supply the basal ganglia, thalami, white matter, and brainstem.

July 7, 2025 at 10:06 PM
PATHOPHYSIOLOGY
Small vessel occlusions refer to ischemic strokes impacting vessels too small to have names. These small perforating arteries are at right angles to larger vessels and primarily supply the basal ganglia, thalami, white matter, and brainstem.
Small vessel occlusions refer to ischemic strokes impacting vessels too small to have names. These small perforating arteries are at right angles to larger vessels and primarily supply the basal ganglia, thalami, white matter, and brainstem.
As before, we will be following the TOAST framework. While the trial itself bears little significance today, the framework it used to categorize strokes is a very helpful cognitive tool and has been repeatedly used in subsequent research.

July 7, 2025 at 10:06 PM
As before, we will be following the TOAST framework. While the trial itself bears little significance today, the framework it used to categorize strokes is a very helpful cognitive tool and has been repeatedly used in subsequent research.
Antiplatelets are also a key factor. APT is preferred based on the mechanism (Virchow’s triad: endothelial injury leads to primary platelet aggregation) as well as trial data (eg WASSID). Sometimes DAPT is used, but always for a limited time (often 90d).
July 5, 2025 at 9:33 PM
Antiplatelets are also a key factor. APT is preferred based on the mechanism (Virchow’s triad: endothelial injury leads to primary platelet aggregation) as well as trial data (eg WASSID). Sometimes DAPT is used, but always for a limited time (often 90d).
LAA usually causes either full-territory or embolic-appearing strokes confined to a single vascular territory. There are exceptions (such as athero-embolism “jailing” a small vessel causing a lacunar appearance) but this is a good rule of thumb.
July 5, 2025 at 9:33 PM
LAA usually causes either full-territory or embolic-appearing strokes confined to a single vascular territory. There are exceptions (such as athero-embolism “jailing” a small vessel causing a lacunar appearance) but this is a good rule of thumb.
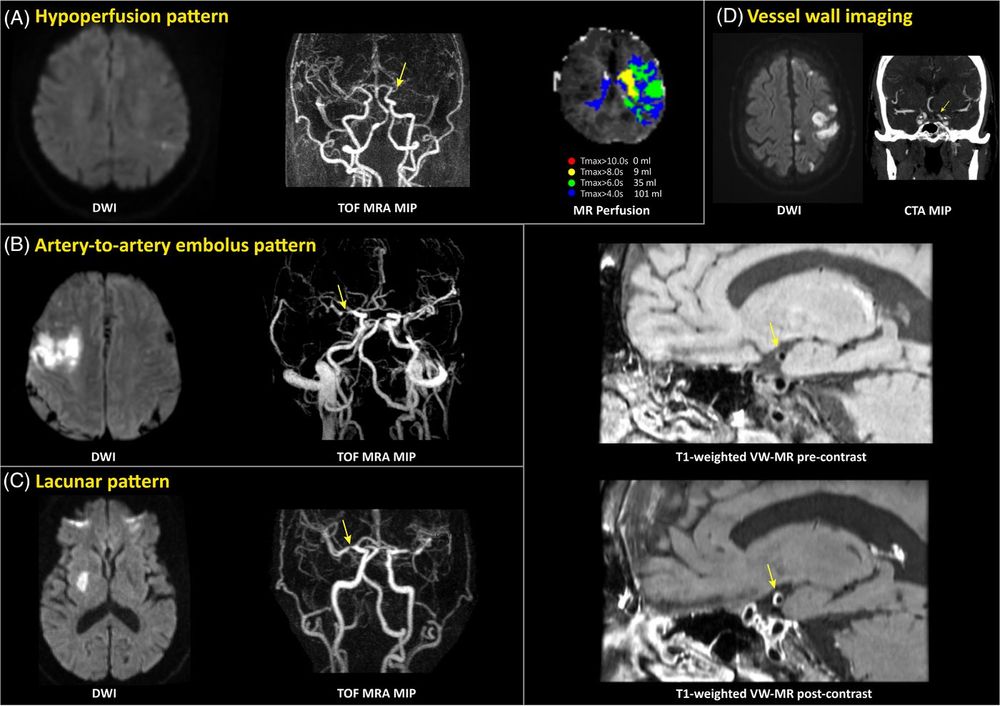
DIAGNOSIS
LAA is diagnosed based on imaging characteristics, both of the stroke itself and the blood vessels. The latter is critical for management, meaning we need vessel imaging to work it up.
Options include:
- CTA (preferred)
- MRA
- Carotid ultrasound
LAA is diagnosed based on imaging characteristics, both of the stroke itself and the blood vessels. The latter is critical for management, meaning we need vessel imaging to work it up.
Options include:
- CTA (preferred)
- MRA
- Carotid ultrasound

July 5, 2025 at 9:33 PM
DIAGNOSIS
LAA is diagnosed based on imaging characteristics, both of the stroke itself and the blood vessels. The latter is critical for management, meaning we need vessel imaging to work it up.
Options include:
- CTA (preferred)
- MRA
- Carotid ultrasound
LAA is diagnosed based on imaging characteristics, both of the stroke itself and the blood vessels. The latter is critical for management, meaning we need vessel imaging to work it up.
Options include:
- CTA (preferred)
- MRA
- Carotid ultrasound
PATHOPHYSIOLOGY
LAA is caused by the same common pathway that often causes other vascular diseases including MIs and PVD: atherosclerosis.
Risk factors include anything that causes vessel trauma: HTN, diabetes, smoking, FHx, and high LDL. It accounts for about 25% of strokes in the USA.
LAA is caused by the same common pathway that often causes other vascular diseases including MIs and PVD: atherosclerosis.
Risk factors include anything that causes vessel trauma: HTN, diabetes, smoking, FHx, and high LDL. It accounts for about 25% of strokes in the USA.

July 5, 2025 at 9:33 PM
PATHOPHYSIOLOGY
LAA is caused by the same common pathway that often causes other vascular diseases including MIs and PVD: atherosclerosis.
Risk factors include anything that causes vessel trauma: HTN, diabetes, smoking, FHx, and high LDL. It accounts for about 25% of strokes in the USA.
LAA is caused by the same common pathway that often causes other vascular diseases including MIs and PVD: atherosclerosis.
Risk factors include anything that causes vessel trauma: HTN, diabetes, smoking, FHx, and high LDL. It accounts for about 25% of strokes in the USA.
For decades, stroke neurologists have categorized strokes into five etiologies based on the TOAST criteria: large artery atherosclerosis, cardioembolic, small vessel, embolic stroke of undetermined source, and other.
Let’s start with large artery atherosclerosis.
Let’s start with large artery atherosclerosis.
July 5, 2025 at 9:33 PM
For decades, stroke neurologists have categorized strokes into five etiologies based on the TOAST criteria: large artery atherosclerosis, cardioembolic, small vessel, embolic stroke of undetermined source, and other.
Let’s start with large artery atherosclerosis.
Let’s start with large artery atherosclerosis.
PHYSIOLOGY
The cerebellum receives inputs from 3 sources: eyes, inner ear, and nerves. If any one system goes down, you have a backup. If 2 go down, or if the cerebellum goes out, you have a problem.
The cerebellum receives inputs from 3 sources: eyes, inner ear, and nerves. If any one system goes down, you have a backup. If 2 go down, or if the cerebellum goes out, you have a problem.

July 4, 2025 at 12:35 AM
PHYSIOLOGY
The cerebellum receives inputs from 3 sources: eyes, inner ear, and nerves. If any one system goes down, you have a backup. If 2 go down, or if the cerebellum goes out, you have a problem.
The cerebellum receives inputs from 3 sources: eyes, inner ear, and nerves. If any one system goes down, you have a backup. If 2 go down, or if the cerebellum goes out, you have a problem.
To check for a Romberg sign, have the patient stand with their feet together with their eyes closed. Excessive swaying or falling within 30-60 seconds is a positive test.
There are also variants designed to increase sensitivity in special situations.
There are also variants designed to increase sensitivity in special situations.

July 4, 2025 at 12:35 AM
To check for a Romberg sign, have the patient stand with their feet together with their eyes closed. Excessive swaying or falling within 30-60 seconds is a positive test.
There are also variants designed to increase sensitivity in special situations.
There are also variants designed to increase sensitivity in special situations.
Can you actually trust the computer's QT measurement, though? Good point. If the baseline is wonky, maybe not. Have no fear, you can simply manually count the number of small boxes and plug that in on the same calculator on MDCalc. It really does it all.

June 26, 2025 at 1:32 PM
Can you actually trust the computer's QT measurement, though? Good point. If the baseline is wonky, maybe not. Have no fear, you can simply manually count the number of small boxes and plug that in on the same calculator on MDCalc. It really does it all.
The good news is that MDCalc has an easy and free calculator to fix this: just type in the HR and uncorrected QT and choose which formula you want. 15 seconds or less!

June 26, 2025 at 1:32 PM
The good news is that MDCalc has an easy and free calculator to fix this: just type in the HR and uncorrected QT and choose which formula you want. 15 seconds or less!
Here's a graph comparing how each formula compares at different heart rates (technically 1/HR). You want the line to be flat. None are perfect, but you'll notice that one performs nearly as poorly as not correcting at all: Bazett.

June 26, 2025 at 1:32 PM
Here's a graph comparing how each formula compares at different heart rates (technically 1/HR). You want the line to be flat. None are perfect, but you'll notice that one performs nearly as poorly as not correcting at all: Bazett.
Background: QT intervals change depending on HR. To compare them, one can correct for HR using many different formulas:
- Bazett
- Hodges
- Fridericia
- Framingham
- Rautaharju
- Bazett
- Hodges
- Fridericia
- Framingham
- Rautaharju

June 26, 2025 at 1:32 PM
Background: QT intervals change depending on HR. To compare them, one can correct for HR using many different formulas:
- Bazett
- Hodges
- Fridericia
- Framingham
- Rautaharju
- Bazett
- Hodges
- Fridericia
- Framingham
- Rautaharju
This degree of detail is rarely clinically relevant, and we can simplify for mnemonic purposes into two groups per level: middle (M) and side (S).
Medulla: ASA (M) + PICA (S)
Pons: basilar (M) + AICA (S)
Midbrain: SCA (inf M/S) + PCA (sup M/S)
Medulla: ASA (M) + PICA (S)
Pons: basilar (M) + AICA (S)
Midbrain: SCA (inf M/S) + PCA (sup M/S)

June 24, 2025 at 5:56 PM
This degree of detail is rarely clinically relevant, and we can simplify for mnemonic purposes into two groups per level: middle (M) and side (S).
Medulla: ASA (M) + PICA (S)
Pons: basilar (M) + AICA (S)
Midbrain: SCA (inf M/S) + PCA (sup M/S)
Medulla: ASA (M) + PICA (S)
Pons: basilar (M) + AICA (S)
Midbrain: SCA (inf M/S) + PCA (sup M/S)
Now to really get practical, you also want to apply vascular anatomy! Each level of the brainstem is supplied by 4 (!) groups of vessels:
- Anteromedial (paramedian)
- Anterolateral (short circumferential)
- Lateral (long circumferential)
- Posterior
- Anteromedial (paramedian)
- Anterolateral (short circumferential)
- Lateral (long circumferential)
- Posterior

June 24, 2025 at 5:56 PM
Now to really get practical, you also want to apply vascular anatomy! Each level of the brainstem is supplied by 4 (!) groups of vessels:
- Anteromedial (paramedian)
- Anterolateral (short circumferential)
- Lateral (long circumferential)
- Posterior
- Anteromedial (paramedian)
- Anterolateral (short circumferential)
- Lateral (long circumferential)
- Posterior