




Geoff Macintyre
@gmaci.bsky.social
Group leader in computational oncology at CNIO, Madrid. CSO at Tailor Bio. Chromosomal instability and tumour evolution. www.macintyrelab.org
9/ To ensure a flexible pathway to the clinic, we also tested biomarker reproducibility in ctDNA samples and TSO500 panel data, bringing us closer to real-world implementation

June 23, 2025 at 9:03 AM
9/ To ensure a flexible pathway to the clinic, we also tested biomarker reproducibility in ctDNA samples and TSO500 panel data, bringing us closer to real-world implementation
8/ It worked! We emulated trials to validate resistance predictions to platins, taxanes & anthracyclines across ovarian, breast, prostate & sarcoma

June 23, 2025 at 9:03 AM
8/ It worked! We emulated trials to validate resistance predictions to platins, taxanes & anthracyclines across ovarian, breast, prostate & sarcoma
7/ Next step? A prospective trial? We tried but couldn’t! No one wanted to run/fund a trial using “old” chemos. So we had to get creative. Luckily, as chemos are widely used, there was a wealth of real-world data eg TCGA & @HartwigMedical to emulate biomarker trials - even RCTs!

June 23, 2025 at 9:03 AM
7/ Next step? A prospective trial? We tried but couldn’t! No one wanted to run/fund a trial using “old” chemos. So we had to get creative. Luckily, as chemos are widely used, there was a wealth of real-world data eg TCGA & @HartwigMedical to emulate biomarker trials - even RCTs!
6/ Our results looked great!

June 23, 2025 at 9:03 AM
6/ Our results looked great!
4/ We focused on optimising 3 CIN signature-based biomarkers to classify patients as resistant or sensitive to 3 commonly used chemotherapies: platins, taxanes or anthracyclines. Our goal: to optimise biomarker thresholds to use pan-cancer

June 23, 2025 at 9:03 AM
4/ We focused on optimising 3 CIN signature-based biomarkers to classify patients as resistant or sensitive to 3 commonly used chemotherapies: platins, taxanes or anthracyclines. Our goal: to optimise biomarker thresholds to use pan-cancer
MET amps cause EGFRi resistance in ~25% of NSCLCs. Forecasting MET amp in 33 EGFR-mutant NSCLC tumours treated with osimertinib showed high-risk patients had shorter PFS & OS. This can be used to flag candidates for upfront EGFR+MET inhibition (eg MARIPOSA trial) 12/

June 10, 2025 at 2:15 PM
MET amps cause EGFRi resistance in ~25% of NSCLCs. Forecasting MET amp in 33 EGFR-mutant NSCLC tumours treated with osimertinib showed high-risk patients had shorter PFS & OS. This can be used to flag candidates for upfront EGFR+MET inhibition (eg MARIPOSA trial) 12/
Currently, LGGs are classified into 4 WHO risk groups. CDK4/PDGFRA amps and CDKN2A dels are linked with poor prognosis but under utilised. Forecasting these facilitates a risk upgrade of 9% of IDHmut-non-codel cases while maintaining median survival times across WHO groups 11/

June 10, 2025 at 2:15 PM
Currently, LGGs are classified into 4 WHO risk groups. CDK4/PDGFRA amps and CDKN2A dels are linked with poor prognosis but under utilised. Forecasting these facilitates a risk upgrade of 9% of IDHmut-non-codel cases while maintaining median survival times across WHO groups 11/
Next we tested longitudinal pairs forecasting at the early time point (before driver amp) and testing at the latter. In prostate, we predicted AR amp (linked to ADT resistance) in pretreatment samples. In NSCLC, we predicted HIST1H3B amp (exclusive to metastases) in primaries 9/

June 10, 2025 at 2:15 PM
Next we tested longitudinal pairs forecasting at the early time point (before driver amp) and testing at the latter. In prostate, we predicted AR amp (linked to ADT resistance) in pretreatment samples. In NSCLC, we predicted HIST1H3B amp (exclusive to metastases) in primaries 9/
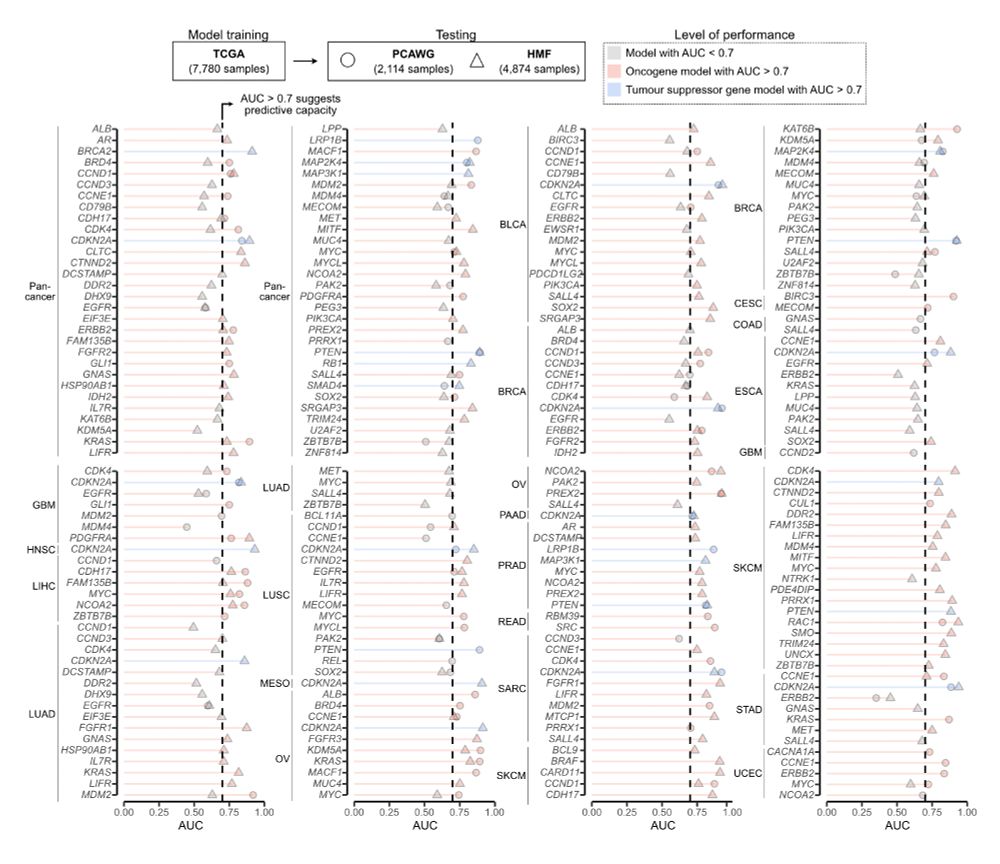
First, we tested performance on two independent cohorts: PCAWG: 2,114 primaries; HMF: 4,784 metastases. 147 of the 241 models showed AUC > 0.7 across both datasets 8/
June 10, 2025 at 2:15 PM
First, we tested performance on two independent cohorts: PCAWG: 2,114 primaries; HMF: 4,784 metastases. 147 of the 241 models showed AUC > 0.7 across both datasets 8/
Challenge 3: forecasting in a clinical setting. Solution: binarise predictions and only use standard genomic test data as input. We designed guidelines to apply and (if needed) train the model + optimize thresholds for binary risk classification (high vs low) 6/

June 10, 2025 at 2:15 PM
Challenge 3: forecasting in a clinical setting. Solution: binarise predictions and only use standard genomic test data as input. We designed guidelines to apply and (if needed) train the model + optimize thresholds for binary risk classification (high vs low) 6/
Challenge 2: growth rates of mutant vs non-mutant cells (and thus selection) cannot be easily determined in a clinical context. Solution: approximate selection coeffs using driver amp/del frequency at a population-level (supported by recent work showing s≈fβ) 5/

June 10, 2025 at 2:15 PM
Challenge 2: growth rates of mutant vs non-mutant cells (and thus selection) cannot be easily determined in a clinical context. Solution: approximate selection coeffs using driver amp/del frequency at a population-level (supported by recent work showing s≈fβ) 5/
Challenge 1: amp/del rates cannot be readily measured from an input genome. Solution: approximate using a steady-state probability of locus-specific copy number change over tumour lifetime. We adapted our previous CIN signatures (CX bit.ly/42SVA3i) for this 4/

June 10, 2025 at 2:15 PM
Challenge 1: amp/del rates cannot be readily measured from an input genome. Solution: approximate using a steady-state probability of locus-specific copy number change over tumour lifetime. We adapted our previous CIN signatures (CX bit.ly/42SVA3i) for this 4/
Inspired by previous work showing that cancer genome evolution is deterministic bit.ly/44sAYBG bit.ly/4d3MBBb we built a model that uses mutation rate and selection estimates to predict the probability of future driver amp/dels, given a tumour genome as input 2/

June 10, 2025 at 2:15 PM
Inspired by previous work showing that cancer genome evolution is deterministic bit.ly/44sAYBG bit.ly/4d3MBBb we built a model that uses mutation rate and selection estimates to predict the probability of future driver amp/dels, given a tumour genome as input 2/
If you are at AACR and want to find out how we are turning chemotherapies into precision medicines, come to my talk on Tuesday! www.abstractsonline.com/pp8/#!/20273...

April 27, 2025 at 10:37 PM
If you are at AACR and want to find out how we are turning chemotherapies into precision medicines, come to my talk on Tuesday! www.abstractsonline.com/pp8/#!/20273...