

David Warner (he/him)
@davidwarner2.bsky.social
First-generation, non-traditional MS4 at UCincy. UNC ‘14. MSMP CWRU ‘21. Former high school teacher and lab tech. Budding nephrologist.
Interested in physiology, medical education, LGBTQ+ health, and the kidneys.
Skeets are my own/not medical advice. 🏳️🌈
Interested in physiology, medical education, LGBTQ+ health, and the kidneys.
Skeets are my own/not medical advice. 🏳️🌈
Summary:
🧠 MSCC is an onc emergency causing severe back pain + FND
🧠 Dx: whole-spine MRI
🧠 Tx: steroids, pain control, radiotherapy, +/- surgery
Sources:
1. 2023 NICE Guidelines: buff.ly/3DC4SrM
2. Review by Akanda/McKay: buff.ly/4iZOoK8.
3. Youtube: buff.ly/40koN7i
🧠 MSCC is an onc emergency causing severe back pain + FND
🧠 Dx: whole-spine MRI
🧠 Tx: steroids, pain control, radiotherapy, +/- surgery
Sources:
1. 2023 NICE Guidelines: buff.ly/3DC4SrM
2. Review by Akanda/McKay: buff.ly/4iZOoK8.
3. Youtube: buff.ly/40koN7i
Recommendations | Spinal metastases and metastatic spinal cord compression | Guidance | NICE
NICE guideline [NG234] Published: 06 September 2023
www.nice.org.uk
March 7, 2025 at 1:00 PM
Summary:
🧠 MSCC is an onc emergency causing severe back pain + FND
🧠 Dx: whole-spine MRI
🧠 Tx: steroids, pain control, radiotherapy, +/- surgery
Sources:
1. 2023 NICE Guidelines: buff.ly/3DC4SrM
2. Review by Akanda/McKay: buff.ly/4iZOoK8.
3. Youtube: buff.ly/40koN7i
🧠 MSCC is an onc emergency causing severe back pain + FND
🧠 Dx: whole-spine MRI
🧠 Tx: steroids, pain control, radiotherapy, +/- surgery
Sources:
1. 2023 NICE Guidelines: buff.ly/3DC4SrM
2. Review by Akanda/McKay: buff.ly/4iZOoK8.
3. Youtube: buff.ly/40koN7i
Surgical options include decompression and stabilization.
Indications:
🧠 Single level cord compression
🧠 Adequate baseline performance status
🧠 Spinal instability present
🧠 Uncontrolled pain
🧠 Radioresistant tumor
🧠 Histological diagnosis
Surgery is often followed by adjuvant radiotherapy.
Indications:
🧠 Single level cord compression
🧠 Adequate baseline performance status
🧠 Spinal instability present
🧠 Uncontrolled pain
🧠 Radioresistant tumor
🧠 Histological diagnosis
Surgery is often followed by adjuvant radiotherapy.
March 7, 2025 at 1:00 PM
Surgical options include decompression and stabilization.
Indications:
🧠 Single level cord compression
🧠 Adequate baseline performance status
🧠 Spinal instability present
🧠 Uncontrolled pain
🧠 Radioresistant tumor
🧠 Histological diagnosis
Surgery is often followed by adjuvant radiotherapy.
Indications:
🧠 Single level cord compression
🧠 Adequate baseline performance status
🧠 Spinal instability present
🧠 Uncontrolled pain
🧠 Radioresistant tumor
🧠 Histological diagnosis
Surgery is often followed by adjuvant radiotherapy.
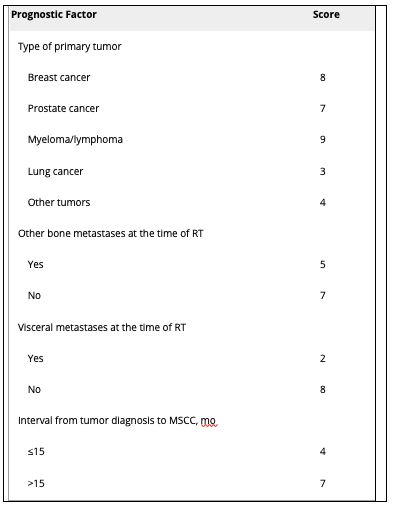
Rades et. al published a validated scoring system to predict prognosis within 6 months to guide radiotherapy.
🧠 Score 20-30 = poor prognosis (short-course recommended)
🧠 Score 30-35 = intermediate prognosis
🧠 Score 36-45 = favorable prognosis (longer course recommended, as more likely to recur)
🧠 Score 20-30 = poor prognosis (short-course recommended)
🧠 Score 30-35 = intermediate prognosis
🧠 Score 36-45 = favorable prognosis (longer course recommended, as more likely to recur)
March 7, 2025 at 1:00 PM
Rades et. al published a validated scoring system to predict prognosis within 6 months to guide radiotherapy.
🧠 Score 20-30 = poor prognosis (short-course recommended)
🧠 Score 30-35 = intermediate prognosis
🧠 Score 36-45 = favorable prognosis (longer course recommended, as more likely to recur)
🧠 Score 20-30 = poor prognosis (short-course recommended)
🧠 Score 30-35 = intermediate prognosis
🧠 Score 36-45 = favorable prognosis (longer course recommended, as more likely to recur)
Radiotherapy:
🧠 Offer within 24 hrs if the pt is not a surgical candidate (unless pt has been tetra- or paraplegic for 2 wks and pain is managed)
🧠 Assess desire for future fertility
🧠 Repeat radiotherapy if good response and symptoms return >3 months after treatment
🧠 Offer within 24 hrs if the pt is not a surgical candidate (unless pt has been tetra- or paraplegic for 2 wks and pain is managed)
🧠 Assess desire for future fertility
🧠 Repeat radiotherapy if good response and symptoms return >3 months after treatment
March 7, 2025 at 1:00 PM
Radiotherapy:
🧠 Offer within 24 hrs if the pt is not a surgical candidate (unless pt has been tetra- or paraplegic for 2 wks and pain is managed)
🧠 Assess desire for future fertility
🧠 Repeat radiotherapy if good response and symptoms return >3 months after treatment
🧠 Offer within 24 hrs if the pt is not a surgical candidate (unless pt has been tetra- or paraplegic for 2 wks and pain is managed)
🧠 Assess desire for future fertility
🧠 Repeat radiotherapy if good response and symptoms return >3 months after treatment
Management:
🧠 Spine immobilization
🧠 Corticosteroids (16 mg as soon as suspected, taper after radiotherapy/surgery)
🧠 Radiotherapy
🧠 Surgical decompression and/or stabilization
🧠 External spine support (e.g. halo vest or Milwaukee brace) if spine instability and not a surgical candidate
🧠 Spine immobilization
🧠 Corticosteroids (16 mg as soon as suspected, taper after radiotherapy/surgery)
🧠 Radiotherapy
🧠 Surgical decompression and/or stabilization
🧠 External spine support (e.g. halo vest or Milwaukee brace) if spine instability and not a surgical candidate
March 7, 2025 at 1:00 PM
Management:
🧠 Spine immobilization
🧠 Corticosteroids (16 mg as soon as suspected, taper after radiotherapy/surgery)
🧠 Radiotherapy
🧠 Surgical decompression and/or stabilization
🧠 External spine support (e.g. halo vest or Milwaukee brace) if spine instability and not a surgical candidate
🧠 Spine immobilization
🧠 Corticosteroids (16 mg as soon as suspected, taper after radiotherapy/surgery)
🧠 Radiotherapy
🧠 Surgical decompression and/or stabilization
🧠 External spine support (e.g. halo vest or Milwaukee brace) if spine instability and not a surgical candidate
Workup:
🧠 MRI w/in 24 hrs: sagittal T1 and T2-weighted sequence of whole spine + axial imaging of detected lesions
🧠 CT + myelogram if MRI contraindicated
🧠 Bladder scan if relevant + Foley if needed
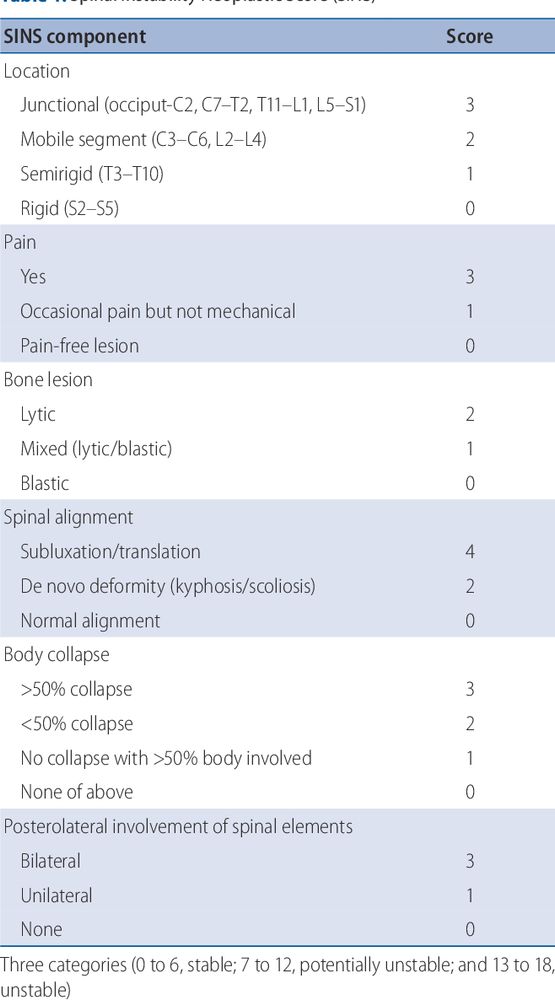
🧠 Assess for spinal instability (e.g. Spinal Instability Neoplastic Score)
🧠 MRI w/in 24 hrs: sagittal T1 and T2-weighted sequence of whole spine + axial imaging of detected lesions
🧠 CT + myelogram if MRI contraindicated
🧠 Bladder scan if relevant + Foley if needed
🧠 Assess for spinal instability (e.g. Spinal Instability Neoplastic Score)
March 7, 2025 at 1:00 PM
Workup:
🧠 MRI w/in 24 hrs: sagittal T1 and T2-weighted sequence of whole spine + axial imaging of detected lesions
🧠 CT + myelogram if MRI contraindicated
🧠 Bladder scan if relevant + Foley if needed
🧠 Assess for spinal instability (e.g. Spinal Instability Neoplastic Score)
🧠 MRI w/in 24 hrs: sagittal T1 and T2-weighted sequence of whole spine + axial imaging of detected lesions
🧠 CT + myelogram if MRI contraindicated
🧠 Bladder scan if relevant + Foley if needed
🧠 Assess for spinal instability (e.g. Spinal Instability Neoplastic Score)
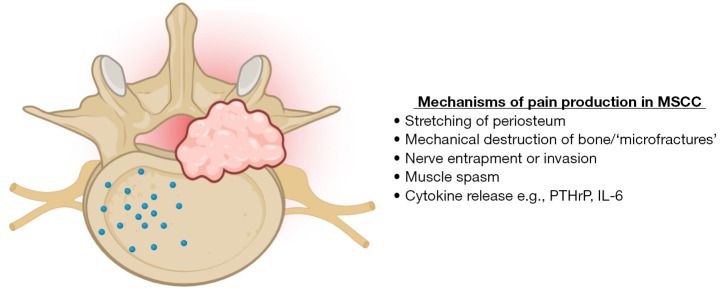
Clinical features:
Back pain is the most common symptom.
🧠 Severe and localized
🧠 Worse when coughing, sneezing, defecating or lying down
🧠 Progressive worsening
🧠 Disturbs sleep
Other features
🧠 Weakness
🧠 Sensory disturbance
🧠 Autonomic dysfunction
🧠 Paralysis
🧠 Cauda equina syndrome
Back pain is the most common symptom.
🧠 Severe and localized
🧠 Worse when coughing, sneezing, defecating or lying down
🧠 Progressive worsening
🧠 Disturbs sleep
Other features
🧠 Weakness
🧠 Sensory disturbance
🧠 Autonomic dysfunction
🧠 Paralysis
🧠 Cauda equina syndrome
March 7, 2025 at 1:00 PM
Clinical features:
Back pain is the most common symptom.
🧠 Severe and localized
🧠 Worse when coughing, sneezing, defecating or lying down
🧠 Progressive worsening
🧠 Disturbs sleep
Other features
🧠 Weakness
🧠 Sensory disturbance
🧠 Autonomic dysfunction
🧠 Paralysis
🧠 Cauda equina syndrome
Back pain is the most common symptom.
🧠 Severe and localized
🧠 Worse when coughing, sneezing, defecating or lying down
🧠 Progressive worsening
🧠 Disturbs sleep
Other features
🧠 Weakness
🧠 Sensory disturbance
🧠 Autonomic dysfunction
🧠 Paralysis
🧠 Cauda equina syndrome
MSCC usually results from hematogenous spread to the vertebrae with the thoracic spine most commonly affected due to its blood supply.
The mechanisms of MSCC include
🧠 tumor invasion into the epidural space
🧠 encroachment of vertebrae on the spinal cord
🧠 obstruction of the epidural vein plexus
The mechanisms of MSCC include
🧠 tumor invasion into the epidural space
🧠 encroachment of vertebrae on the spinal cord
🧠 obstruction of the epidural vein plexus
March 7, 2025 at 1:00 PM
MSCC usually results from hematogenous spread to the vertebrae with the thoracic spine most commonly affected due to its blood supply.
The mechanisms of MSCC include
🧠 tumor invasion into the epidural space
🧠 encroachment of vertebrae on the spinal cord
🧠 obstruction of the epidural vein plexus
The mechanisms of MSCC include
🧠 tumor invasion into the epidural space
🧠 encroachment of vertebrae on the spinal cord
🧠 obstruction of the epidural vein plexus
MSCC is most commonly caused by metastasis to the vertebrae caused most commonly by the following cancers:
Adults
🧠 Lung
🧠 Breast
🧠 Prostate
🧠 Less common: renal cell carcinoma, myeloma, lymphoma, GI cancers, melanoma
Children
🧠 Sarcomas
🧠 Neuroblastomas
🧠 Neuroectodermal tumors
Adults
🧠 Lung
🧠 Breast
🧠 Prostate
🧠 Less common: renal cell carcinoma, myeloma, lymphoma, GI cancers, melanoma
Children
🧠 Sarcomas
🧠 Neuroblastomas
🧠 Neuroectodermal tumors
March 7, 2025 at 1:00 PM
MSCC is most commonly caused by metastasis to the vertebrae caused most commonly by the following cancers:
Adults
🧠 Lung
🧠 Breast
🧠 Prostate
🧠 Less common: renal cell carcinoma, myeloma, lymphoma, GI cancers, melanoma
Children
🧠 Sarcomas
🧠 Neuroblastomas
🧠 Neuroectodermal tumors
Adults
🧠 Lung
🧠 Breast
🧠 Prostate
🧠 Less common: renal cell carcinoma, myeloma, lymphoma, GI cancers, melanoma
Children
🧠 Sarcomas
🧠 Neuroblastomas
🧠 Neuroectodermal tumors
Sources:
1. 2023 Umbrella review by Shah, et. al: buff.ly/3DCwnkJ
2. Overview of Etiologies, Manifestations, and Treatments by Quencer: buff.ly/41ZXIrs
3. Excellent Youtube video by Dr. Strong: buff.ly/4gVG1gP
4. Amboss (Oncological Emergencies)
1. 2023 Umbrella review by Shah, et. al: buff.ly/3DCwnkJ
2. Overview of Etiologies, Manifestations, and Treatments by Quencer: buff.ly/41ZXIrs
3. Excellent Youtube video by Dr. Strong: buff.ly/4gVG1gP
4. Amboss (Oncological Emergencies)
SVC Syndrome (Oncologic Emergencies)
An overview of the clinical presentation, etiologies, diagnosis, and treatment of the superior vena cava syndrome - a serious complication of non-small cell ...
www.youtube.com
February 28, 2025 at 1:01 PM
Sources:
1. 2023 Umbrella review by Shah, et. al: buff.ly/3DCwnkJ
2. Overview of Etiologies, Manifestations, and Treatments by Quencer: buff.ly/41ZXIrs
3. Excellent Youtube video by Dr. Strong: buff.ly/4gVG1gP
4. Amboss (Oncological Emergencies)
1. 2023 Umbrella review by Shah, et. al: buff.ly/3DCwnkJ
2. Overview of Etiologies, Manifestations, and Treatments by Quencer: buff.ly/41ZXIrs
3. Excellent Youtube video by Dr. Strong: buff.ly/4gVG1gP
4. Amboss (Oncological Emergencies)
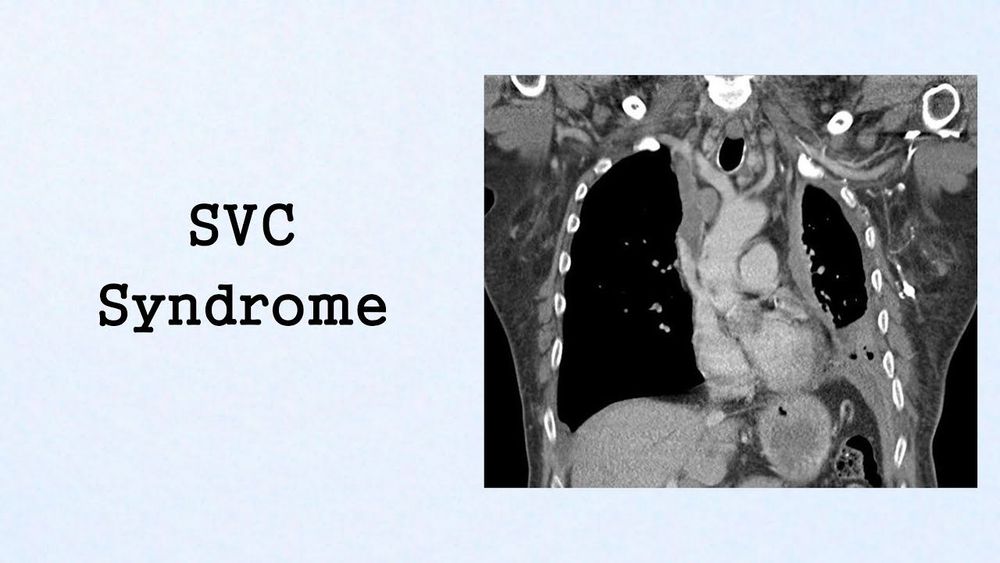
Summary:
🫀SVC syndrome is a medical emergency most commonly caused by malignancies (NSCLC, SCLC, NHL)
🫀Increasingly caused by thrombosis from catheters or pacemakers
🫀Oropharyngeal, respiratory, or cerebral involvement are red flags
🫀Stenting is now the treatment of choice for symptomatic pts
🫀SVC syndrome is a medical emergency most commonly caused by malignancies (NSCLC, SCLC, NHL)
🫀Increasingly caused by thrombosis from catheters or pacemakers
🫀Oropharyngeal, respiratory, or cerebral involvement are red flags
🫀Stenting is now the treatment of choice for symptomatic pts
February 28, 2025 at 1:01 PM
Summary:
🫀SVC syndrome is a medical emergency most commonly caused by malignancies (NSCLC, SCLC, NHL)
🫀Increasingly caused by thrombosis from catheters or pacemakers
🫀Oropharyngeal, respiratory, or cerebral involvement are red flags
🫀Stenting is now the treatment of choice for symptomatic pts
🫀SVC syndrome is a medical emergency most commonly caused by malignancies (NSCLC, SCLC, NHL)
🫀Increasingly caused by thrombosis from catheters or pacemakers
🫀Oropharyngeal, respiratory, or cerebral involvement are red flags
🫀Stenting is now the treatment of choice for symptomatic pts
Treatment for catheter-associated thrombosis
🫀Catheter-directed thrombolysis or thrombo-aspiration
🫀If severe symptoms, mechanical thrombectomy
🫀Anticoagulation for at least 3 months
🫀Catheter-directed thrombolysis or thrombo-aspiration
🫀If severe symptoms, mechanical thrombectomy
🫀Anticoagulation for at least 3 months
February 28, 2025 at 1:01 PM
Treatment for catheter-associated thrombosis
🫀Catheter-directed thrombolysis or thrombo-aspiration
🫀If severe symptoms, mechanical thrombectomy
🫀Anticoagulation for at least 3 months
🫀Catheter-directed thrombolysis or thrombo-aspiration
🫀If severe symptoms, mechanical thrombectomy
🫀Anticoagulation for at least 3 months
Management
🫀If severe symptoms present, emergency endovascular stent
🫀If laryngeal edema present, intubate!
🫀Steroids may be beneficial for laryngeal edema, as well as lymphoma and thymoma (but biopsy first!)
🫀Treat underlying malignancy
🫀If severe symptoms present, emergency endovascular stent
🫀If laryngeal edema present, intubate!
🫀Steroids may be beneficial for laryngeal edema, as well as lymphoma and thymoma (but biopsy first!)
🫀Treat underlying malignancy
February 28, 2025 at 1:01 PM
Management
🫀If severe symptoms present, emergency endovascular stent
🫀If laryngeal edema present, intubate!
🫀Steroids may be beneficial for laryngeal edema, as well as lymphoma and thymoma (but biopsy first!)
🫀Treat underlying malignancy
🫀If severe symptoms present, emergency endovascular stent
🫀If laryngeal edema present, intubate!
🫀Steroids may be beneficial for laryngeal edema, as well as lymphoma and thymoma (but biopsy first!)
🫀Treat underlying malignancy
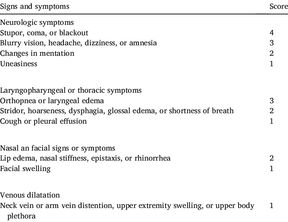
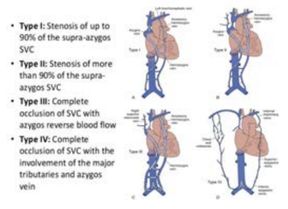
Scoring systems have been created to guide management:
🫀 The Kishi scoring system
- Score >3 indicates need for stenting
🫀 The Yu grading system
- Score of 3 or 4 indicates need for stenting
🫀The Stanford Method
- Venography used to identify patients at risk for airway or brain involvement
🫀 The Kishi scoring system
- Score >3 indicates need for stenting
🫀 The Yu grading system
- Score of 3 or 4 indicates need for stenting
🫀The Stanford Method
- Venography used to identify patients at risk for airway or brain involvement

February 28, 2025 at 1:01 PM
Scoring systems have been created to guide management:
🫀 The Kishi scoring system
- Score >3 indicates need for stenting
🫀 The Yu grading system
- Score of 3 or 4 indicates need for stenting
🫀The Stanford Method
- Venography used to identify patients at risk for airway or brain involvement
🫀 The Kishi scoring system
- Score >3 indicates need for stenting
🫀 The Yu grading system
- Score of 3 or 4 indicates need for stenting
🫀The Stanford Method
- Venography used to identify patients at risk for airway or brain involvement