


David Warner (he/him)
@davidwarner2.bsky.social
First-generation, non-traditional MS4 at UCincy. UNC ‘14. MSMP CWRU ‘21. Former high school teacher and lab tech. Budding nephrologist.
Interested in physiology, medical education, LGBTQ+ health, and the kidneys.
Skeets are my own/not medical advice. 🏳️🌈
Interested in physiology, medical education, LGBTQ+ health, and the kidneys.
Skeets are my own/not medical advice. 🏳️🌈
AOA induction dinner! Congratulations to my amazing classmates; can’t wait to see where you end up in 2 weeks and hear about your future accomplishments! #Match2025 #UCCOMClassof2025



March 7, 2025 at 8:49 PM
AOA induction dinner! Congratulations to my amazing classmates; can’t wait to see where you end up in 2 weeks and hear about your future accomplishments! #Match2025 #UCCOMClassof2025
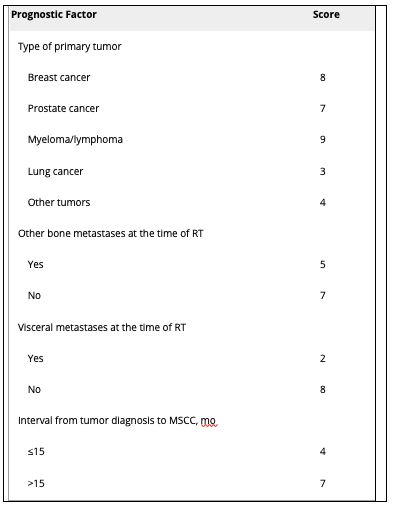
Rades et. al published a validated scoring system to predict prognosis within 6 months to guide radiotherapy.
🧠 Score 20-30 = poor prognosis (short-course recommended)
🧠 Score 30-35 = intermediate prognosis
🧠 Score 36-45 = favorable prognosis (longer course recommended, as more likely to recur)
🧠 Score 20-30 = poor prognosis (short-course recommended)
🧠 Score 30-35 = intermediate prognosis
🧠 Score 36-45 = favorable prognosis (longer course recommended, as more likely to recur)
March 7, 2025 at 1:00 PM
Rades et. al published a validated scoring system to predict prognosis within 6 months to guide radiotherapy.
🧠 Score 20-30 = poor prognosis (short-course recommended)
🧠 Score 30-35 = intermediate prognosis
🧠 Score 36-45 = favorable prognosis (longer course recommended, as more likely to recur)
🧠 Score 20-30 = poor prognosis (short-course recommended)
🧠 Score 30-35 = intermediate prognosis
🧠 Score 36-45 = favorable prognosis (longer course recommended, as more likely to recur)
Workup:
🧠 MRI w/in 24 hrs: sagittal T1 and T2-weighted sequence of whole spine + axial imaging of detected lesions
🧠 CT + myelogram if MRI contraindicated
🧠 Bladder scan if relevant + Foley if needed
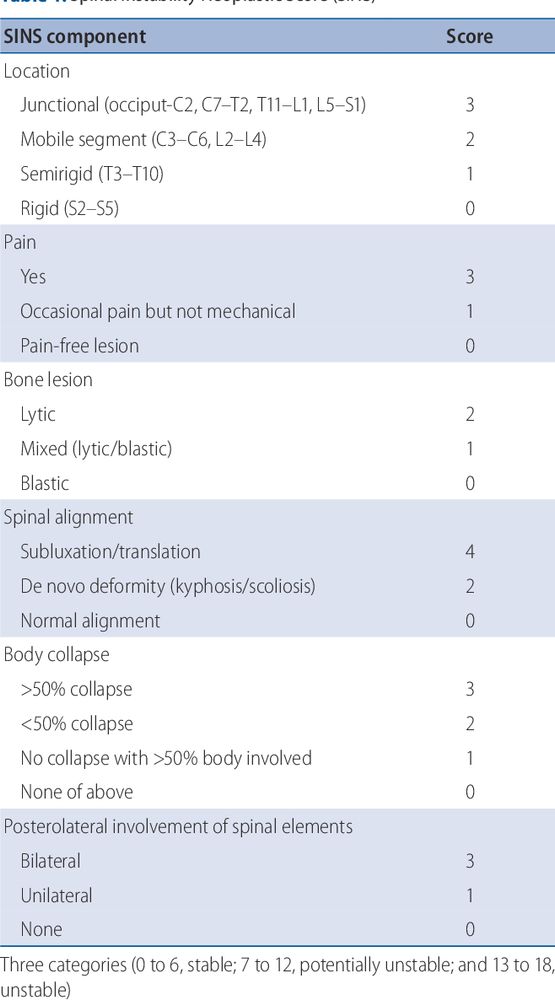
🧠 Assess for spinal instability (e.g. Spinal Instability Neoplastic Score)
🧠 MRI w/in 24 hrs: sagittal T1 and T2-weighted sequence of whole spine + axial imaging of detected lesions
🧠 CT + myelogram if MRI contraindicated
🧠 Bladder scan if relevant + Foley if needed
🧠 Assess for spinal instability (e.g. Spinal Instability Neoplastic Score)
March 7, 2025 at 1:00 PM
Workup:
🧠 MRI w/in 24 hrs: sagittal T1 and T2-weighted sequence of whole spine + axial imaging of detected lesions
🧠 CT + myelogram if MRI contraindicated
🧠 Bladder scan if relevant + Foley if needed
🧠 Assess for spinal instability (e.g. Spinal Instability Neoplastic Score)
🧠 MRI w/in 24 hrs: sagittal T1 and T2-weighted sequence of whole spine + axial imaging of detected lesions
🧠 CT + myelogram if MRI contraindicated
🧠 Bladder scan if relevant + Foley if needed
🧠 Assess for spinal instability (e.g. Spinal Instability Neoplastic Score)
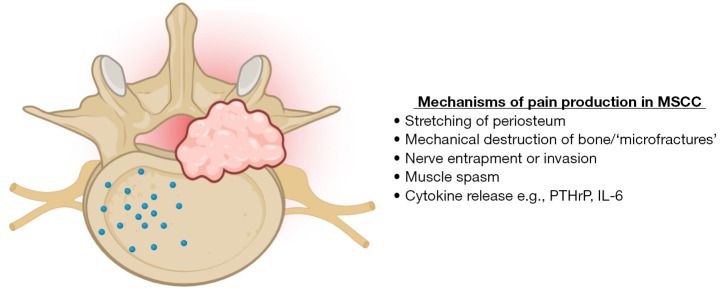
Clinical features:
Back pain is the most common symptom.
🧠 Severe and localized
🧠 Worse when coughing, sneezing, defecating or lying down
🧠 Progressive worsening
🧠 Disturbs sleep
Other features
🧠 Weakness
🧠 Sensory disturbance
🧠 Autonomic dysfunction
🧠 Paralysis
🧠 Cauda equina syndrome
Back pain is the most common symptom.
🧠 Severe and localized
🧠 Worse when coughing, sneezing, defecating or lying down
🧠 Progressive worsening
🧠 Disturbs sleep
Other features
🧠 Weakness
🧠 Sensory disturbance
🧠 Autonomic dysfunction
🧠 Paralysis
🧠 Cauda equina syndrome
March 7, 2025 at 1:00 PM
Clinical features:
Back pain is the most common symptom.
🧠 Severe and localized
🧠 Worse when coughing, sneezing, defecating or lying down
🧠 Progressive worsening
🧠 Disturbs sleep
Other features
🧠 Weakness
🧠 Sensory disturbance
🧠 Autonomic dysfunction
🧠 Paralysis
🧠 Cauda equina syndrome
Back pain is the most common symptom.
🧠 Severe and localized
🧠 Worse when coughing, sneezing, defecating or lying down
🧠 Progressive worsening
🧠 Disturbs sleep
Other features
🧠 Weakness
🧠 Sensory disturbance
🧠 Autonomic dysfunction
🧠 Paralysis
🧠 Cauda equina syndrome
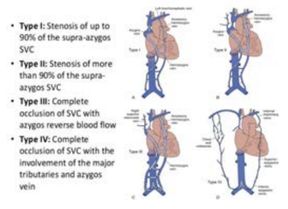
Scoring systems have been created to guide management:
🫀 The Kishi scoring system
- Score >3 indicates need for stenting
🫀 The Yu grading system
- Score of 3 or 4 indicates need for stenting
🫀The Stanford Method
- Venography used to identify patients at risk for airway or brain involvement
🫀 The Kishi scoring system
- Score >3 indicates need for stenting
🫀 The Yu grading system
- Score of 3 or 4 indicates need for stenting
🫀The Stanford Method
- Venography used to identify patients at risk for airway or brain involvement

February 28, 2025 at 1:01 PM
Scoring systems have been created to guide management:
🫀 The Kishi scoring system
- Score >3 indicates need for stenting
🫀 The Yu grading system
- Score of 3 or 4 indicates need for stenting
🫀The Stanford Method
- Venography used to identify patients at risk for airway or brain involvement
🫀 The Kishi scoring system
- Score >3 indicates need for stenting
🫀 The Yu grading system
- Score of 3 or 4 indicates need for stenting
🫀The Stanford Method
- Venography used to identify patients at risk for airway or brain involvement
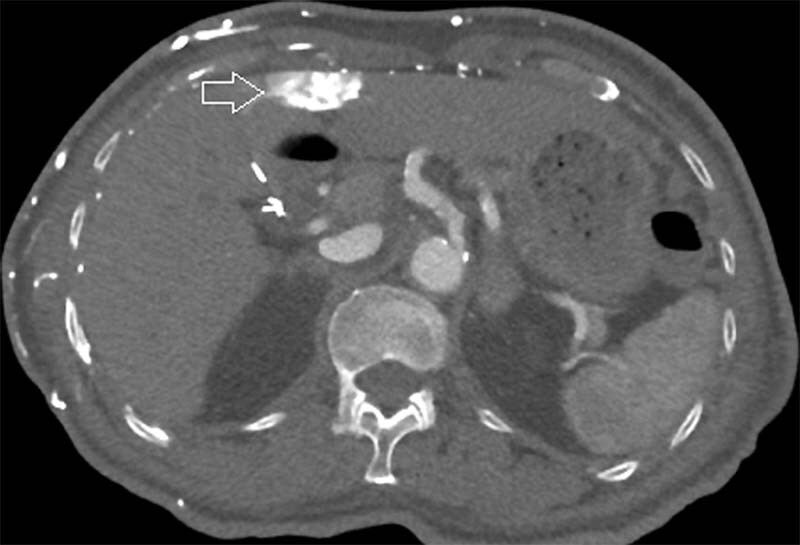
🫀 The drainage of dilated chest wall veins to the left portal vein via the veins of Sappey can lead to perfusion changes and a "hot quadrate sign" around the falciform ligament, seen on this CT.
February 28, 2025 at 1:01 PM
🫀 The drainage of dilated chest wall veins to the left portal vein via the veins of Sappey can lead to perfusion changes and a "hot quadrate sign" around the falciform ligament, seen on this CT.
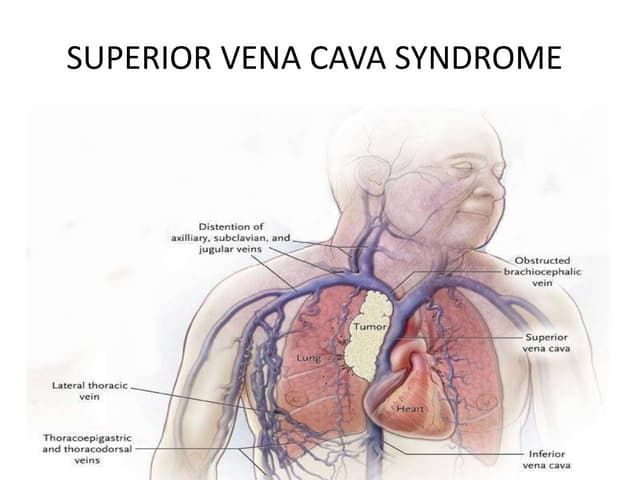
Review of anatomy:
🫀SVC drains blood from the brachiocephalic veins, which receive blood from the head and upper extremities
🫀Collateral supply is important in SVC syndrome
🫀Upper/mid esophageal veins drain into the esophagus, causing "downhill esophageal varices"
🫀SVC drains blood from the brachiocephalic veins, which receive blood from the head and upper extremities
🫀Collateral supply is important in SVC syndrome
🫀Upper/mid esophageal veins drain into the esophagus, causing "downhill esophageal varices"
February 28, 2025 at 1:01 PM
Review of anatomy:
🫀SVC drains blood from the brachiocephalic veins, which receive blood from the head and upper extremities
🫀Collateral supply is important in SVC syndrome
🫀Upper/mid esophageal veins drain into the esophagus, causing "downhill esophageal varices"
🫀SVC drains blood from the brachiocephalic veins, which receive blood from the head and upper extremities
🫀Collateral supply is important in SVC syndrome
🫀Upper/mid esophageal veins drain into the esophagus, causing "downhill esophageal varices"
Summary:
🩸Leukostasis = symptomatic hyperleukocytosis (WBC >100,000)
🩸Clinical features = respiratory and neurological symptoms
🩸May cause falsely high K, low O2, and high platelets
🩸Definitive treatment = induction chemo but perform bone marrow bx first
🩸Use hydroxurea while awaiting studies
🩸Leukostasis = symptomatic hyperleukocytosis (WBC >100,000)
🩸Clinical features = respiratory and neurological symptoms
🩸May cause falsely high K, low O2, and high platelets
🩸Definitive treatment = induction chemo but perform bone marrow bx first
🩸Use hydroxurea while awaiting studies

February 21, 2025 at 1:01 PM
Summary:
🩸Leukostasis = symptomatic hyperleukocytosis (WBC >100,000)
🩸Clinical features = respiratory and neurological symptoms
🩸May cause falsely high K, low O2, and high platelets
🩸Definitive treatment = induction chemo but perform bone marrow bx first
🩸Use hydroxurea while awaiting studies
🩸Leukostasis = symptomatic hyperleukocytosis (WBC >100,000)
🩸Clinical features = respiratory and neurological symptoms
🩸May cause falsely high K, low O2, and high platelets
🩸Definitive treatment = induction chemo but perform bone marrow bx first
🩸Use hydroxurea while awaiting studies
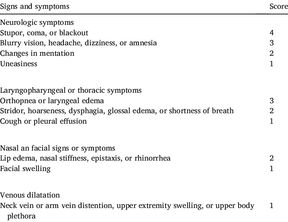
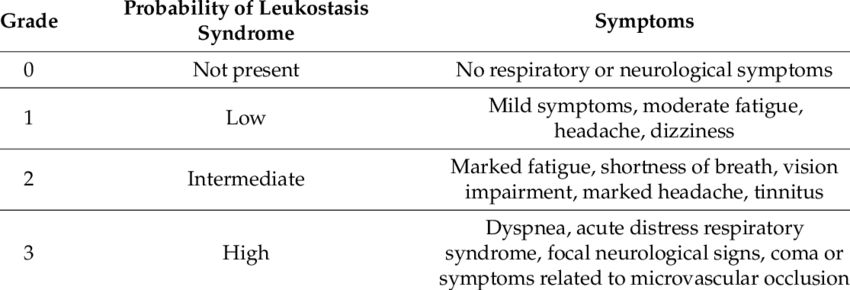
Leukostasis is a clinical diagnosis that should be suspected in patients with leukemia who develop
🩸Respiratory distress
🩸Neurological changes
🩸Other end organ damage
🩸Hyperleukocytosis
Novotny et. al (2005) created the attached grading score to predict the probability of leukostasis.
🩸Respiratory distress
🩸Neurological changes
🩸Other end organ damage
🩸Hyperleukocytosis
Novotny et. al (2005) created the attached grading score to predict the probability of leukostasis.
February 21, 2025 at 1:01 PM
Leukostasis is a clinical diagnosis that should be suspected in patients with leukemia who develop
🩸Respiratory distress
🩸Neurological changes
🩸Other end organ damage
🩸Hyperleukocytosis
Novotny et. al (2005) created the attached grading score to predict the probability of leukostasis.
🩸Respiratory distress
🩸Neurological changes
🩸Other end organ damage
🩸Hyperleukocytosis
Novotny et. al (2005) created the attached grading score to predict the probability of leukostasis.
When to stop abx:
🌡️ Known source: usual duration + ANC is improving and >500
🌡️ Unknown source: no fever for >2 days + ANC is improving and >500
Prophylaxis:
🌡️ IDSA guidelines regarding prophylaxis are outlined in the attached table.
🌡️ Known source: usual duration + ANC is improving and >500
🌡️ Unknown source: no fever for >2 days + ANC is improving and >500
Prophylaxis:
🌡️ IDSA guidelines regarding prophylaxis are outlined in the attached table.

February 14, 2025 at 1:00 PM
When to stop abx:
🌡️ Known source: usual duration + ANC is improving and >500
🌡️ Unknown source: no fever for >2 days + ANC is improving and >500
Prophylaxis:
🌡️ IDSA guidelines regarding prophylaxis are outlined in the attached table.
🌡️ Known source: usual duration + ANC is improving and >500
🌡️ Unknown source: no fever for >2 days + ANC is improving and >500
Prophylaxis:
🌡️ IDSA guidelines regarding prophylaxis are outlined in the attached table.
If hemodynamically unstable:
🌡️ Meropenem/imipenem
🌡️ Vancomycin
🌡️ Aminoglycoside or ciprofloxacin
Only use vancomycin if:
🌡️ Skin/soft tissue infection
🌡️ Catheter-related infection
🌡️ Pneumonia
🌡️ Hemodynamically unstable
Add antifungal if no response within 3-7 days.
🌡️ Meropenem/imipenem
🌡️ Vancomycin
🌡️ Aminoglycoside or ciprofloxacin
Only use vancomycin if:
🌡️ Skin/soft tissue infection
🌡️ Catheter-related infection
🌡️ Pneumonia
🌡️ Hemodynamically unstable
Add antifungal if no response within 3-7 days.

February 14, 2025 at 1:00 PM
If hemodynamically unstable:
🌡️ Meropenem/imipenem
🌡️ Vancomycin
🌡️ Aminoglycoside or ciprofloxacin
Only use vancomycin if:
🌡️ Skin/soft tissue infection
🌡️ Catheter-related infection
🌡️ Pneumonia
🌡️ Hemodynamically unstable
Add antifungal if no response within 3-7 days.
🌡️ Meropenem/imipenem
🌡️ Vancomycin
🌡️ Aminoglycoside or ciprofloxacin
Only use vancomycin if:
🌡️ Skin/soft tissue infection
🌡️ Catheter-related infection
🌡️ Pneumonia
🌡️ Hemodynamically unstable
Add antifungal if no response within 3-7 days.
Treatment:
🌡️ Once blood cultures are drawn, start empiric antibiotics within 1 hr
Inpatient:
🌡️ Empiric cefepime, pip-tazo, or meropenem is recommended
🌡️ Severe penicillin allergy: ciprofloxacin + clindamycin
🌡️ Broaden if suspected MDRO
Outpatient:
🌡️ Ciprofloxacin + Augmentin
🌡️ Once blood cultures are drawn, start empiric antibiotics within 1 hr
Inpatient:
🌡️ Empiric cefepime, pip-tazo, or meropenem is recommended
🌡️ Severe penicillin allergy: ciprofloxacin + clindamycin
🌡️ Broaden if suspected MDRO
Outpatient:
🌡️ Ciprofloxacin + Augmentin

February 14, 2025 at 1:00 PM
Treatment:
🌡️ Once blood cultures are drawn, start empiric antibiotics within 1 hr
Inpatient:
🌡️ Empiric cefepime, pip-tazo, or meropenem is recommended
🌡️ Severe penicillin allergy: ciprofloxacin + clindamycin
🌡️ Broaden if suspected MDRO
Outpatient:
🌡️ Ciprofloxacin + Augmentin
🌡️ Once blood cultures are drawn, start empiric antibiotics within 1 hr
Inpatient:
🌡️ Empiric cefepime, pip-tazo, or meropenem is recommended
🌡️ Severe penicillin allergy: ciprofloxacin + clindamycin
🌡️ Broaden if suspected MDRO
Outpatient:
🌡️ Ciprofloxacin + Augmentin
A few risk scores have also been adopted in society guidelines:
1. MASCC Scoring System
📋 Score <21 = inpatient
2. Talcott's rules
📋 Groups I-III = inpatient
📋Group IV low-risk = outpatient
3. CISNE
📋 Used for stable pts receiving mild-mod chemo for solid malignancy
📋 Score >2 = inpatient
1. MASCC Scoring System
📋 Score <21 = inpatient
2. Talcott's rules
📋 Groups I-III = inpatient
📋Group IV low-risk = outpatient
3. CISNE
📋 Used for stable pts receiving mild-mod chemo for solid malignancy
📋 Score >2 = inpatient




February 14, 2025 at 1:00 PM
A few risk scores have also been adopted in society guidelines:
1. MASCC Scoring System
📋 Score <21 = inpatient
2. Talcott's rules
📋 Groups I-III = inpatient
📋Group IV low-risk = outpatient
3. CISNE
📋 Used for stable pts receiving mild-mod chemo for solid malignancy
📋 Score >2 = inpatient
1. MASCC Scoring System
📋 Score <21 = inpatient
2. Talcott's rules
📋 Groups I-III = inpatient
📋Group IV low-risk = outpatient
3. CISNE
📋 Used for stable pts receiving mild-mod chemo for solid malignancy
📋 Score >2 = inpatient
Clinical presentation:
🦀 Stones (nephrolithiasis)
🦀 Groans (abdominal pain, N/V, pancreatitis)
🦀 Bones (bone pain, muscle weakness)
🦀 Psychiatric overtones (depression, anxiety)
🦀 Cardiac manifestations (short QT, bradycardia, AVN blockade)
🦀 Nephrogenic DI (polyuria, thirst)
🦀 Stones (nephrolithiasis)
🦀 Groans (abdominal pain, N/V, pancreatitis)
🦀 Bones (bone pain, muscle weakness)
🦀 Psychiatric overtones (depression, anxiety)
🦀 Cardiac manifestations (short QT, bradycardia, AVN blockade)
🦀 Nephrogenic DI (polyuria, thirst)


February 7, 2025 at 7:00 PM
Clinical presentation:
🦀 Stones (nephrolithiasis)
🦀 Groans (abdominal pain, N/V, pancreatitis)
🦀 Bones (bone pain, muscle weakness)
🦀 Psychiatric overtones (depression, anxiety)
🦀 Cardiac manifestations (short QT, bradycardia, AVN blockade)
🦀 Nephrogenic DI (polyuria, thirst)
🦀 Stones (nephrolithiasis)
🦀 Groans (abdominal pain, N/V, pancreatitis)
🦀 Bones (bone pain, muscle weakness)
🦀 Psychiatric overtones (depression, anxiety)
🦀 Cardiac manifestations (short QT, bradycardia, AVN blockade)
🦀 Nephrogenic DI (polyuria, thirst)
Hyperuricemia
Options:
🦀 Rasburicase
🦀 Allopurinol
🦀 Febuxostat
🦀 Dialysis
🦀 Rasburicase is preferred over allopurinol
- Faster acting
- Allopurinol does not remove existing uric acid and leads to buildup of xanthine (also nephrotoxic)
🦀 But, rasburicase is contraindicated in G6PD deficiency
Options:
🦀 Rasburicase
🦀 Allopurinol
🦀 Febuxostat
🦀 Dialysis
🦀 Rasburicase is preferred over allopurinol
- Faster acting
- Allopurinol does not remove existing uric acid and leads to buildup of xanthine (also nephrotoxic)
🦀 But, rasburicase is contraindicated in G6PD deficiency

January 31, 2025 at 6:00 PM
Hyperuricemia
Options:
🦀 Rasburicase
🦀 Allopurinol
🦀 Febuxostat
🦀 Dialysis
🦀 Rasburicase is preferred over allopurinol
- Faster acting
- Allopurinol does not remove existing uric acid and leads to buildup of xanthine (also nephrotoxic)
🦀 But, rasburicase is contraindicated in G6PD deficiency
Options:
🦀 Rasburicase
🦀 Allopurinol
🦀 Febuxostat
🦀 Dialysis
🦀 Rasburicase is preferred over allopurinol
- Faster acting
- Allopurinol does not remove existing uric acid and leads to buildup of xanthine (also nephrotoxic)
🦀 But, rasburicase is contraindicated in G6PD deficiency
The work-up for TLS includes:
🦀 BMP (Cr, BUN, K, Phos, and Ca)
🦀 CBC (WBC, may also have anemia/thrombocytopenia)
🦀 Uric Acid
🦀 EKG
🦀 LDH
🦀 Urinalysis + urine microscopy
TLS is diagnosed via the Cairo-Bishop Classification:
🦀 Laboratory (asymptomatic)
🦀 Clinical (symptomatic)
🦀 BMP (Cr, BUN, K, Phos, and Ca)
🦀 CBC (WBC, may also have anemia/thrombocytopenia)
🦀 Uric Acid
🦀 EKG
🦀 LDH
🦀 Urinalysis + urine microscopy
TLS is diagnosed via the Cairo-Bishop Classification:
🦀 Laboratory (asymptomatic)
🦀 Clinical (symptomatic)

January 31, 2025 at 6:00 PM
The work-up for TLS includes:
🦀 BMP (Cr, BUN, K, Phos, and Ca)
🦀 CBC (WBC, may also have anemia/thrombocytopenia)
🦀 Uric Acid
🦀 EKG
🦀 LDH
🦀 Urinalysis + urine microscopy
TLS is diagnosed via the Cairo-Bishop Classification:
🦀 Laboratory (asymptomatic)
🦀 Clinical (symptomatic)
🦀 BMP (Cr, BUN, K, Phos, and Ca)
🦀 CBC (WBC, may also have anemia/thrombocytopenia)
🦀 Uric Acid
🦀 EKG
🦀 LDH
🦀 Urinalysis + urine microscopy
TLS is diagnosed via the Cairo-Bishop Classification:
🦀 Laboratory (asymptomatic)
🦀 Clinical (symptomatic)
So what is the physiologic basis underlying the use of glucagon in BB/CCB overdose?
🫀Cardiac myocytes have glucagon receptors
🫀These receptors also act through Gs proteins to activate PKA, providing the above benefits even in the setting of BB or CCB toxicity
🫀Cardiac myocytes have glucagon receptors
🫀These receptors also act through Gs proteins to activate PKA, providing the above benefits even in the setting of BB or CCB toxicity

January 24, 2025 at 1:00 PM
So what is the physiologic basis underlying the use of glucagon in BB/CCB overdose?
🫀Cardiac myocytes have glucagon receptors
🫀These receptors also act through Gs proteins to activate PKA, providing the above benefits even in the setting of BB or CCB toxicity
🫀Cardiac myocytes have glucagon receptors
🫀These receptors also act through Gs proteins to activate PKA, providing the above benefits even in the setting of BB or CCB toxicity
To start, let's review myocardial contractility to understand how glucagon works.
🫀L-type Ca channels open ➡️ Ca binds RyR ➡️ Ca released from sarcoplasmic reticulum
🫀Ca binds troponin C ➡️ exposes myosin-binding site of actin
🫀SERCA2 pumps Ca back into SR
🫀Phospholamban inhibits SERCA2
🫀L-type Ca channels open ➡️ Ca binds RyR ➡️ Ca released from sarcoplasmic reticulum
🫀Ca binds troponin C ➡️ exposes myosin-binding site of actin
🫀SERCA2 pumps Ca back into SR
🫀Phospholamban inhibits SERCA2


January 24, 2025 at 1:00 PM
To start, let's review myocardial contractility to understand how glucagon works.
🫀L-type Ca channels open ➡️ Ca binds RyR ➡️ Ca released from sarcoplasmic reticulum
🫀Ca binds troponin C ➡️ exposes myosin-binding site of actin
🫀SERCA2 pumps Ca back into SR
🫀Phospholamban inhibits SERCA2
🫀L-type Ca channels open ➡️ Ca binds RyR ➡️ Ca released from sarcoplasmic reticulum
🫀Ca binds troponin C ➡️ exposes myosin-binding site of actin
🫀SERCA2 pumps Ca back into SR
🫀Phospholamban inhibits SERCA2
What are the risk factors for BRASH Syndrome?
📝Elderly patients
📝Pts with underlying kidney disease
📝Volume depletion (dehydration, diuretic use)
📝Use of ACEi or ARBs
📝Use of K-sparing diuretics (spironolactone)
📝Elderly patients
📝Pts with underlying kidney disease
📝Volume depletion (dehydration, diuretic use)
📝Use of ACEi or ARBs
📝Use of K-sparing diuretics (spironolactone)

January 17, 2025 at 1:00 PM
What are the risk factors for BRASH Syndrome?
📝Elderly patients
📝Pts with underlying kidney disease
📝Volume depletion (dehydration, diuretic use)
📝Use of ACEi or ARBs
📝Use of K-sparing diuretics (spironolactone)
📝Elderly patients
📝Pts with underlying kidney disease
📝Volume depletion (dehydration, diuretic use)
📝Use of ACEi or ARBs
📝Use of K-sparing diuretics (spironolactone)
📝 AV node blockers (esp. beta blockers, verapamil, and diltiazem) are renally cleared
📝 In patients with CKD, renal clearance of AVN blockers is impaired
📝 Underlying CKD + AVN blockade (+ARB in this case) ➡️ HyperK
📝 HyperK + AVN blockade ➡️ bradycardia + shock
📝 In patients with CKD, renal clearance of AVN blockers is impaired
📝 Underlying CKD + AVN blockade (+ARB in this case) ➡️ HyperK
📝 HyperK + AVN blockade ➡️ bradycardia + shock

January 17, 2025 at 1:00 PM
📝 AV node blockers (esp. beta blockers, verapamil, and diltiazem) are renally cleared
📝 In patients with CKD, renal clearance of AVN blockers is impaired
📝 Underlying CKD + AVN blockade (+ARB in this case) ➡️ HyperK
📝 HyperK + AVN blockade ➡️ bradycardia + shock
📝 In patients with CKD, renal clearance of AVN blockers is impaired
📝 Underlying CKD + AVN blockade (+ARB in this case) ➡️ HyperK
📝 HyperK + AVN blockade ➡️ bradycardia + shock
Hyperlipidemia in hypothyroidism is both mediated by low T3 and high TSH
T3
🫀⬇️FFA beta-oxidation
🫀⬇️CYP7A1, leading to impaired cholesterol clearance
🫀⬇️Lipoprotein Lipase, decreasing hydrolysis of VLDL
TSH
🫀⬇️CYP7A1
🫀⬆️PCSK9
🫀⬆️HMG CoA reductase
🫀⬆️Hormone-Sensitive lipase
T3
🫀⬇️FFA beta-oxidation
🫀⬇️CYP7A1, leading to impaired cholesterol clearance
🫀⬇️Lipoprotein Lipase, decreasing hydrolysis of VLDL
TSH
🫀⬇️CYP7A1
🫀⬆️PCSK9
🫀⬆️HMG CoA reductase
🫀⬆️Hormone-Sensitive lipase


January 10, 2025 at 6:08 PM
Hyperlipidemia in hypothyroidism is both mediated by low T3 and high TSH
T3
🫀⬇️FFA beta-oxidation
🫀⬇️CYP7A1, leading to impaired cholesterol clearance
🫀⬇️Lipoprotein Lipase, decreasing hydrolysis of VLDL
TSH
🫀⬇️CYP7A1
🫀⬆️PCSK9
🫀⬆️HMG CoA reductase
🫀⬆️Hormone-Sensitive lipase
T3
🫀⬇️FFA beta-oxidation
🫀⬇️CYP7A1, leading to impaired cholesterol clearance
🫀⬇️Lipoprotein Lipase, decreasing hydrolysis of VLDL
TSH
🫀⬇️CYP7A1
🫀⬆️PCSK9
🫀⬆️HMG CoA reductase
🫀⬆️Hormone-Sensitive lipase
The Osborn waves are secondary to hypothermia from the slower metabolic rate in hypothyroidism and are caused by
🫀Slow conduction speeds
🫀Delayed and prolonged repolarization phase
🫀Hypothermia may also block the transient outward current responsible for Phase 1 of the cardiac AP
🫀Slow conduction speeds
🫀Delayed and prolonged repolarization phase
🫀Hypothermia may also block the transient outward current responsible for Phase 1 of the cardiac AP


January 10, 2025 at 6:08 PM
The Osborn waves are secondary to hypothermia from the slower metabolic rate in hypothyroidism and are caused by
🫀Slow conduction speeds
🫀Delayed and prolonged repolarization phase
🫀Hypothermia may also block the transient outward current responsible for Phase 1 of the cardiac AP
🫀Slow conduction speeds
🫀Delayed and prolonged repolarization phase
🫀Hypothermia may also block the transient outward current responsible for Phase 1 of the cardiac AP
Hypothyroidism also leads to the following arrhythmias:
🫀Bradycardia
🫀Long PQ segment
🫀Diffuse flattened or inverted T waves
🫀Low voltage QRS
🫀AV blockage
🫀Acquired long QT syndrome, which can lead to TdP
🫀Osborn waves
🫀Bradycardia
🫀Long PQ segment
🫀Diffuse flattened or inverted T waves
🫀Low voltage QRS
🫀AV blockage
🫀Acquired long QT syndrome, which can lead to TdP
🫀Osborn waves

January 10, 2025 at 6:08 PM
Hypothyroidism also leads to the following arrhythmias:
🫀Bradycardia
🫀Long PQ segment
🫀Diffuse flattened or inverted T waves
🫀Low voltage QRS
🫀AV blockage
🫀Acquired long QT syndrome, which can lead to TdP
🫀Osborn waves
🫀Bradycardia
🫀Long PQ segment
🫀Diffuse flattened or inverted T waves
🫀Low voltage QRS
🫀AV blockage
🫀Acquired long QT syndrome, which can lead to TdP
🫀Osborn waves
Hypothyroidism has various cardiovascular manifestations including arrhythmias, high blood pressure, dyslipidemia, heart failure, and pericardial effusion.
What are the physiologic mechanisms underlying these associations?
Welcome to another #PhysiologyFriday!
A 🧵
#MedSky #CardioSky
What are the physiologic mechanisms underlying these associations?
Welcome to another #PhysiologyFriday!
A 🧵
#MedSky #CardioSky

January 10, 2025 at 6:08 PM
Hypothyroidism has various cardiovascular manifestations including arrhythmias, high blood pressure, dyslipidemia, heart failure, and pericardial effusion.
What are the physiologic mechanisms underlying these associations?
Welcome to another #PhysiologyFriday!
A 🧵
#MedSky #CardioSky
What are the physiologic mechanisms underlying these associations?
Welcome to another #PhysiologyFriday!
A 🧵
#MedSky #CardioSky
