




Chetan Shenoy
@cshenoy.bsky.social
Cardiologist and researcher, in cardiovascular magnetic resonance imaging, at the University of Minnesota
Thanks for the shoutout! A minor clarification - the high risk phenotype does not even incorporate an abnormal LVEF!!!!
October 2, 2025 at 3:20 AM
Thanks for the shoutout! A minor clarification - the high risk phenotype does not even incorporate an abnormal LVEF!!!!
Here's our paper in Circulation on the topic - bsky.app/profile/para...

Have you ever wondered whether your patient with CAD and cardiomyopathy truly has ischemic cardiomyopathy, or whether the CAD is a “bystander”?
You might be interested in our paper now out in Circulation
#simultaneouspublication
#AHA23
#cardiosky
#Medsky
#WhyCMR
You might be interested in our paper now out in Circulation
#simultaneouspublication
#AHA23
#cardiosky
#Medsky
#WhyCMR

July 17, 2025 at 4:25 PM
Here's our paper in Circulation on the topic - bsky.app/profile/para...
Here's my talk on how to identify the etiology of cardiomyopathy using CMR - www.youtube.com/watch?v=9or8...
Identifying the Cause of Cardiomyopathy Using CMR (Chetan Shenoy, MBBS, MS)
YouTube video by Houston Methodist DeBakey CV Education
www.youtube.com
July 17, 2025 at 12:59 PM
Here's my talk on how to identify the etiology of cardiomyopathy using CMR - www.youtube.com/watch?v=9or8...
In my opinion, both trials are fundamentally useless.
What is ischemic cardiomyopathy?
Both trials defined ischemic cardiomyopathy as LV dysfunction + obstructive CAD.
This does not identify the etiology of cardiomyopathy as ischemic, but identifies the presence of CAD. Two different things!!!
What is ischemic cardiomyopathy?
Both trials defined ischemic cardiomyopathy as LV dysfunction + obstructive CAD.
This does not identify the etiology of cardiomyopathy as ischemic, but identifies the presence of CAD. Two different things!!!
July 17, 2025 at 12:57 PM
In my opinion, both trials are fundamentally useless.
What is ischemic cardiomyopathy?
Both trials defined ischemic cardiomyopathy as LV dysfunction + obstructive CAD.
This does not identify the etiology of cardiomyopathy as ischemic, but identifies the presence of CAD. Two different things!!!
What is ischemic cardiomyopathy?
Both trials defined ischemic cardiomyopathy as LV dysfunction + obstructive CAD.
This does not identify the etiology of cardiomyopathy as ischemic, but identifies the presence of CAD. Two different things!!!
I don't exactly know. But...
1 - There was no real change in ECV in Explorer HCM (PMID 33190524).
2 - An increase in ECV is not necessarily bad. It increases after AVR (PMID 29471937).
3 - The amount of dead myocardium will never decrease. So, a "decrease in LGE" does not mean less badness.
1 - There was no real change in ECV in Explorer HCM (PMID 33190524).
2 - An increase in ECV is not necessarily bad. It increases after AVR (PMID 29471937).
3 - The amount of dead myocardium will never decrease. So, a "decrease in LGE" does not mean less badness.
July 13, 2025 at 4:59 PM
I don't exactly know. But...
1 - There was no real change in ECV in Explorer HCM (PMID 33190524).
2 - An increase in ECV is not necessarily bad. It increases after AVR (PMID 29471937).
3 - The amount of dead myocardium will never decrease. So, a "decrease in LGE" does not mean less badness.
1 - There was no real change in ECV in Explorer HCM (PMID 33190524).
2 - An increase in ECV is not necessarily bad. It increases after AVR (PMID 29471937).
3 - The amount of dead myocardium will never decrease. So, a "decrease in LGE" does not mean less badness.
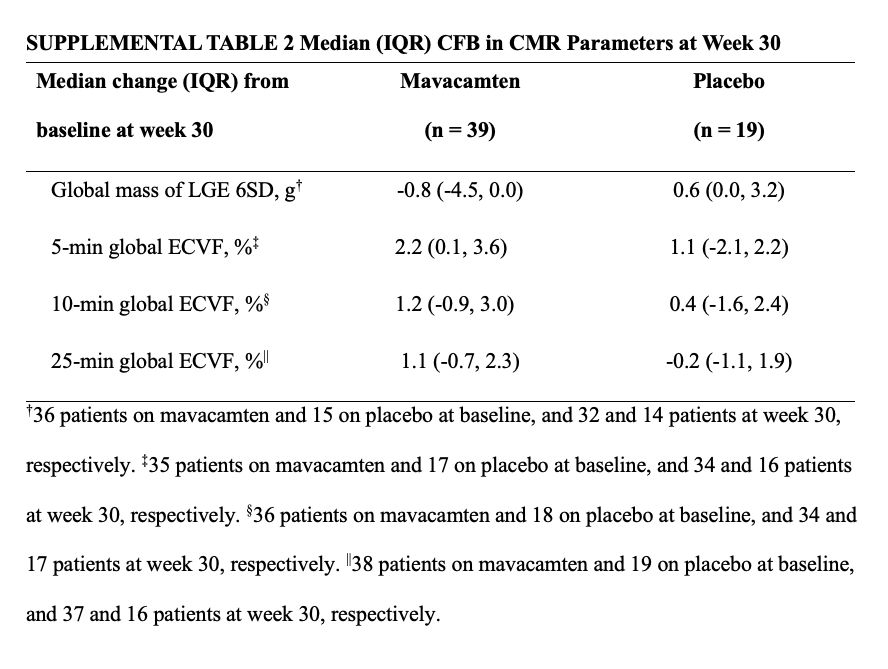
Interesting. The ECV increased 1.1% (25 min) to 2.2% (5 min), which is difficult to explain. But it explains why LGE was less; it was quantified as the amount of myocardium 6SD brighter than "remote". LGE amount will be less if the remote myocardium is brighter after mavacamten than at baseline.
July 13, 2025 at 3:40 PM
Interesting. The ECV increased 1.1% (25 min) to 2.2% (5 min), which is difficult to explain. But it explains why LGE was less; it was quantified as the amount of myocardium 6SD brighter than "remote". LGE amount will be less if the remote myocardium is brighter after mavacamten than at baseline.
June 19, 2025 at 11:49 PM
VT and VF/cardiac arrest - correct. That would be secondary prevention.
AV block is a Class IIa indication for an ICD in the guidelines for cardiac sarcoidosis. But who has cardiac sarcoidosis is not always clear.
What if patient has extracardiac sarcoidosis and complete AV block but no LGE? 🤔
AV block is a Class IIa indication for an ICD in the guidelines for cardiac sarcoidosis. But who has cardiac sarcoidosis is not always clear.
What if patient has extracardiac sarcoidosis and complete AV block but no LGE? 🤔
May 25, 2025 at 5:39 AM
VT and VF/cardiac arrest - correct. That would be secondary prevention.
AV block is a Class IIa indication for an ICD in the guidelines for cardiac sarcoidosis. But who has cardiac sarcoidosis is not always clear.
What if patient has extracardiac sarcoidosis and complete AV block but no LGE? 🤔
AV block is a Class IIa indication for an ICD in the guidelines for cardiac sarcoidosis. But who has cardiac sarcoidosis is not always clear.
What if patient has extracardiac sarcoidosis and complete AV block but no LGE? 🤔
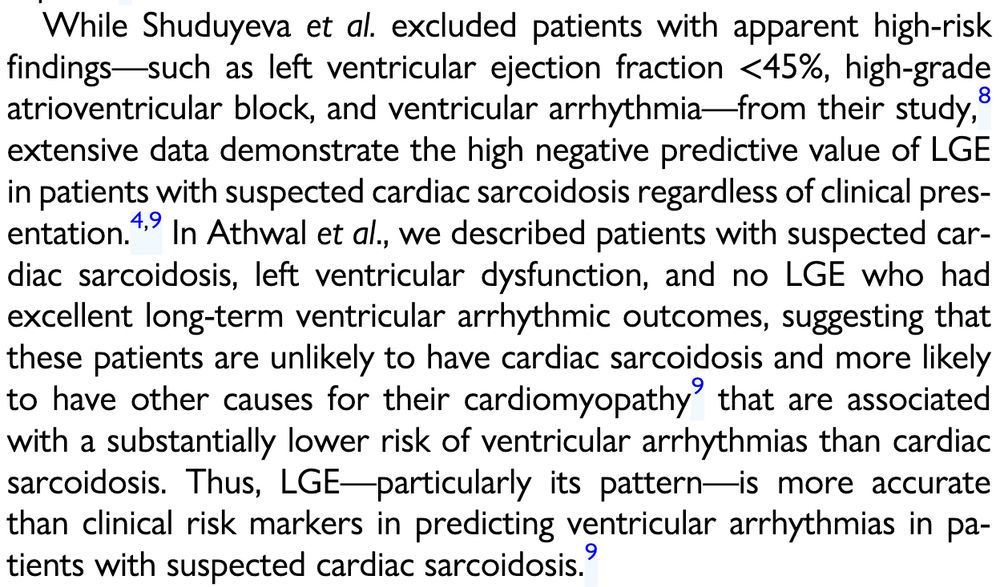
We discuss this in our editorial:
academic.oup.com/ehjcimaging/...
academic.oup.com/ehjcimaging/...
March 23, 2025 at 2:29 AM
We discuss this in our editorial:
academic.oup.com/ehjcimaging/...
academic.oup.com/ehjcimaging/...
Read our accompanying editorial for our thoughts on the important paper –
academic.oup.com/ehjcimaging/...
@paragbawaskar.bsky.social #CardioSky #MedSky #Sarcoidosis
academic.oup.com/ehjcimaging/...
@paragbawaskar.bsky.social #CardioSky #MedSky #Sarcoidosis
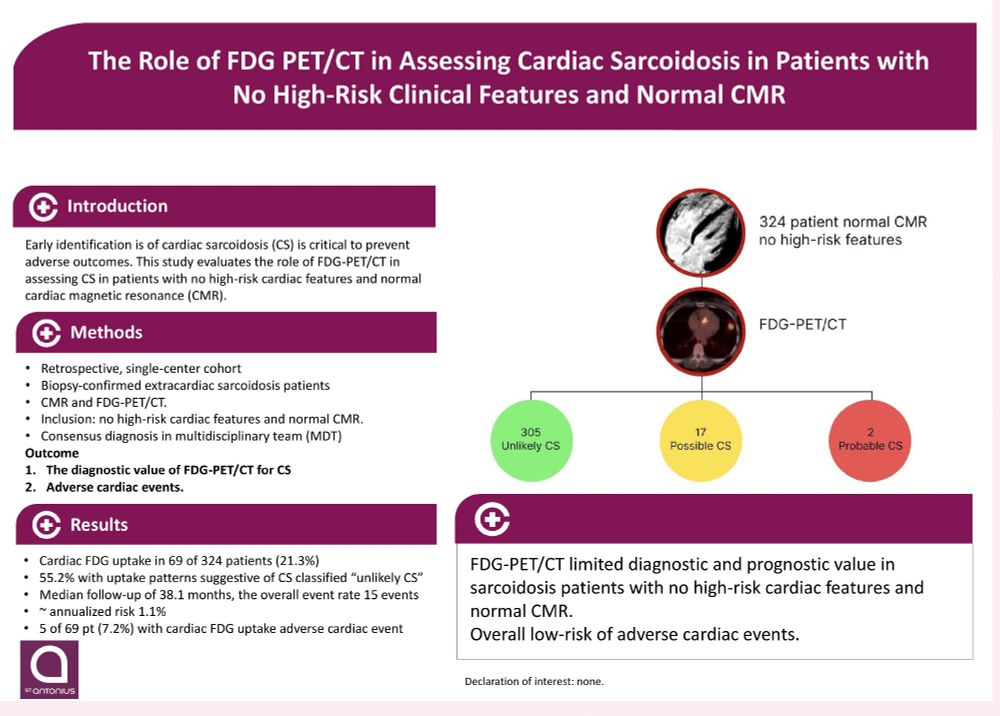
Cardiac FDG-PET imaging in patients with suspected cardiac sarcoidosis and no late gadolinium enhancement on cardiovascular magnetic resonance imaging: the emperor has no clothes!
This editorial refers to ‘The Role of FDG PET/CT in Assessing Cardiac Sarcoidosis with No High-Risk Cardiac Features and Normal CMR’, by F. Shuduyeva et al
academic.oup.com
March 21, 2025 at 11:39 PM
Read our accompanying editorial for our thoughts on the important paper –
academic.oup.com/ehjcimaging/...
@paragbawaskar.bsky.social #CardioSky #MedSky #Sarcoidosis
academic.oup.com/ehjcimaging/...
@paragbawaskar.bsky.social #CardioSky #MedSky #Sarcoidosis
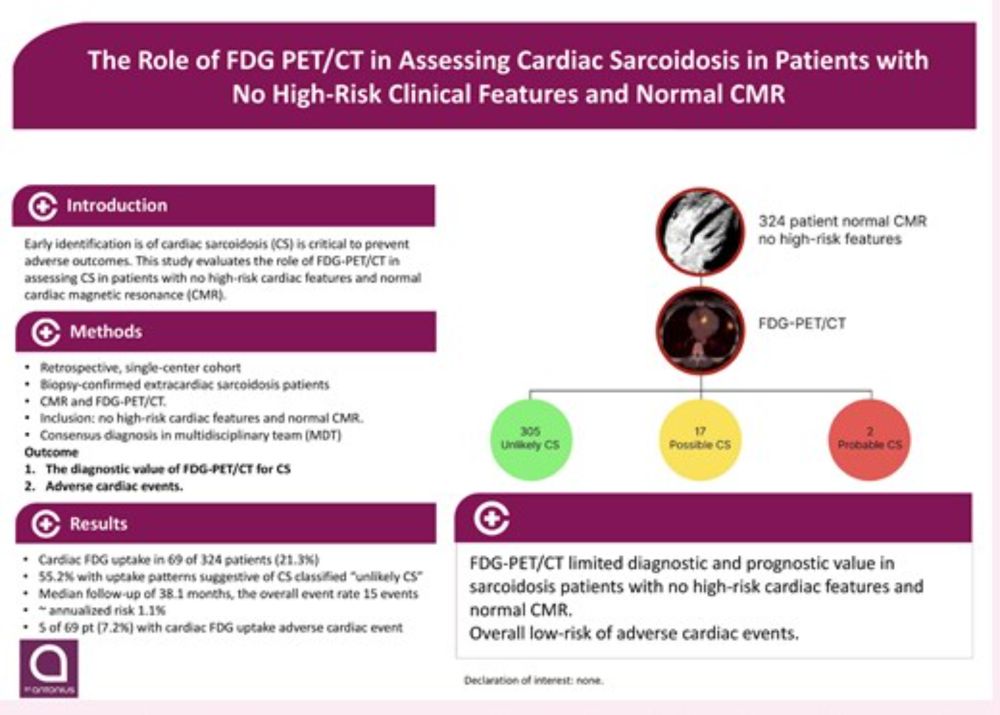
A new study in EHJ - Cardiovascular Imaging describes 324 patients with normal CMR and no high-risk features who all also had FDG-PET.
21.3% had FDG uptake.
Their annualized event rate was <1%, indicating that FDG-PET has little diagnostic or prognostic utility.
21.3% had FDG uptake.
Their annualized event rate was <1%, indicating that FDG-PET has little diagnostic or prognostic utility.
March 21, 2025 at 11:39 PM
A new study in EHJ - Cardiovascular Imaging describes 324 patients with normal CMR and no high-risk features who all also had FDG-PET.
21.3% had FDG uptake.
Their annualized event rate was <1%, indicating that FDG-PET has little diagnostic or prognostic utility.
21.3% had FDG uptake.
Their annualized event rate was <1%, indicating that FDG-PET has little diagnostic or prognostic utility.